
Abstract
Background:
Provision of antiretroviral therapy in resource limited settings has put pressure on the available infrastructure.
Objectives:
The study examined patients’ adherence to Doctor’s appointment attendance after an intervention changing the model of care and factors that predicted adherence.
Methods:
Observational study was carried out over four years. The model of care was changed in the last year and the effect assessed. SPSS version 15.0 was used for analysis. Predictors of adherence were determined using logistic regression model.
Results:
Over half 148 (59.7%) of the patients were females, with a mean age of 40.4±8.8 years and baseline CD4 cells of 143.5±92.7cells/microliters. “Adherence” rates were 51.3% in 2007, 35.9% in 2008 and 14.9% in 2009 giving patients’ average adherence to Doctor’s appointment attendance of 34.03%. Intervention changing the model of care in 2010 recorded an adherence rate of 93.1%.
Conclusions:
The change in model of care greatly improved patients’ “adherence”. Patients’ knowledge of management, adherence, and smoking and drinking habits were identified as statistically significant predictors of adherence.
Introduction
Free antiretroviral (ARV) medications and investigations have been provided in Nigeria since 2004 as a result of support from the President’s Emergency Plan for AIDS Relief (PEPFAR), Global Funds for Tuberculosis, AIDS and Malaria. This has led to an increase in the number of patients accessing care from a couple of thousands to more than 600 000 in over 491 antiretroviral therapy (ART) sites spread across 36 states of Nigeria and the federal capital territory. 1,2 This development led to improvement in existing health facilities and health care providers’ capacity building to provide optimal care that ensures standard patient management and adherence. Research has shown that the long-term effectiveness of highly active antiretroviral therapy (HAART), which is dependent on achieving maximum and durable suppression of human immunodeficiency virus (HIV) plasma viral load, 3 cannot be realized without consistent adherence to maintain exposure. 4,5 This is important as nonadherence has been found to be the major cause for subtherapeutic drug levels, resistance selection, and therapeutic failure. 6,7
Considering that ART is for life and the dynamic nature of adherence, 8 there is a need to use tools that can help to measure patients’ adherence and predict factors that can assist in ensuring optimal adherence in resource-limited settings. It is known that measuring adherence has no “gold standard.” 9 Multiple approaches are used to assess adherence. Friedland and Andrews 3 classified the measure of adherence as a direct assay of biologic markers or body fluids or by indirect methods: self-report, interview, pill counts, pharmacy records, and computerized medication caps.
One such tool, although rarely used, is the monitoring of patients’ adherence to clinic attendance. Kunutsor et al 10 linked poor clinic attendance with mortality in resource-rich countries and as a predictor for virologic failure. Catz and colleagues, as reported by Nakiyemba et al, 11 also found that consistent or regular clinic attendance played a key role in enhancing quality of life and prolonging life for people living with HIV (PLWH). Pill count and adherence to keeping clinic appointments are among the early warning indicators recommended by the World Health Organization (WHO) as surrogate markers for the emergence of HIV drug resistance. 12
Adherence is a dynamic process in which the levels change over time. 13 Due to these reasons, it has been the norm in designing treatment plans to incorporate adherence to maximize the durability and efficacy of any first-line regimen in resource-constrained countries. Factors that influence adherence have been categorized to include patient factors, treatment regimen, disease characteristics, patient-provider relationship, and clinical setting. 14
Deficiency in infrastructure available in resource-constrained settings has led to the use of various methods in the provision of the much-needed HAART to patients. There is a need to assess the various models used to determine the one most effective with regard to patients’ adherence and monitoring.
Our search in the literature has not revealed any published observational study from resource-constrained settings during which patients were observed for around 4 years and assessed for possible predictors of adherence to ART by HIV-positive patients by using doctor’s appointment attendance. The effect of change in the care model in the last year of study on patients’ adherence to HAART in this study site needed to be assessed for short-term effectiveness.
Methods
Study Setting
The study was conducted in the Lagos State University Teaching Hospital (LASUTH), Ikeja, and HIV Clinic. This is one of the tertiary hospitals located in Lagos State, Nigeria, with a 736-bed capacity that serves the people living in Lagos and neighboring states. In December 2006, funding from PEPFAR through a grant awarded to the Institute of Human Virology Nigeria resulted in provision of comprehensive care for identified HIV-positive patients. There exist both pediatric and adult/adolescent clinics.
At inception, the first model of care involved a protocol that involved patients being attended to by trained medical doctors in the initial first 5 to 6 months. Thereafter, trained nurses were allowed to write out prescriptions for drug refills for patients identified as adherent by one of the adherence counselors. Patients must see an adherence counselor at each clinic visit for adherence monitoring and counseling after collection of their prescription from the doctor or the nurse. This model of care was adopted due to the overwhelming number of patients and shortage of physicians trained in HIV and AIDS care. In this model of care, patients do not have to see the physician unless they have a complaint. In the protocol, the documents assessing adherence that have been filled and signed by these trained adherence counselors must be presented at the pharmacy department before any drug refill.
In 2010, a second model of care was introduced, which led to a change in the protocol. In the new model of care, nurses no longer filled out the prescription sheets for drug refills; rather, patients assessed to be adherent by adherence counselors were placed on a quarterly clinic appointment during which they must see a doctor. After being attended to by the doctor, the patients must see the adherence counselor before proceeding to the pharmacy department for drug refills by the pharmacist and reinforcement of adherence counseling.
Ethical Considerations
Ethical approval was obtained from the hospital, and signed informed consent by patients (who met the inclusion criteria) was the only condition for enlisting participation. The confidentiality of information provided was ensured and patients’ anonymity preserved through the use of only the patient’s unique identity number and the hospital number on all documents used in the study.
Selection Criteria
Patients who were recruited for this study met defined inclusion and exclusion criteria, which included such requirements as patients being 18 years or older, taking first-line ARV medications, and having a baseline CD4 count of fewer than 350 cells/mm3 at the beginning of treatment.
Within the period for patient selection in this study (December 2006 to December 2008), 3152 adult patients were enrolled in the clinic, with 1653 (52.4%) receiving ART. Application of the defined criteria for selection reduced the population size available for the study to 884 patients (Figure 1), from which 294 patients were recruited.

Flowchart of patient selection. HAART, highly active antiretroviral therapy.
Study Instruments
The data sources and instrument used were patients’ clinical/hospital case files, clinic appointment record book, and questionnaire set to meet the objectives of the study. The questionnaire covered each patient’s sociodemographic information (age, sex, marital status, religion, educational level, and occupation); relevant medical history (years known to be HIV infected; year that ARV drugs were started); various aspect of patients’ knowledge of HIV, AIDS, and its management; and possible factors that could affect adherence (belief, habit, other medications taken, disclosure of HIV-positive status, stigma, self-organization, and sources of information). The administered questionnaire was developed based on literature reviews of adherence publications that identified various factors that influenced adherence in both developed, developing, and resource-limited countries. Very simple English that could be easily understood irrespective of educational background of the patient was used in forming the questions.
For the purpose of this study, a patient’s doctor appointment attendance adherence form was designed to capture patients’ visits to their doctor on clinic appointment dates.
Study Procedure
A record of patients’ clinic appointment dates was obtained from the patients’ appointment card, and the actual visit date was noted for each study patient. When a patient missed an appointment or rescheduled an appointment, this was recorded. Any doctor’s appointment missed as a result of a doctors’ strike or unexpected public holidays was not counted as missed if the patient returned within a week for a reschedule. In this study, a patient is regarded as having missed an appointment if he or she visited the clinic for a refill on the appointment date but failed to see the doctor.
At the end of each year, percent adherence was calculated using the following formula:

Patients with adherence to a doctor’s appointment <95% were categorized as “nonadherent,” and those who attended ≥95% of their appointments were categorized as “adherent.” Although a literature search revealed a paucity of data with regard to the measurement of adherence using a clinic or doctor’s appointment, 2 published studies 10,15 in Uganda provided a longitudinal relationship between clinic attendance and ART adherence close to the defined ≥95% adherence level required by using other measures of adherence. The cutoff of ≥95% was used as the reference in this study for defining doctor’s appointment “adherence.”
Data Analysis
Data were analyzed by using Statistical Package for Social Sciences (SPSS) version 15.0 for Windows (SPSS, Inc). Using logistic regression, model predictors of patients’ adherence to doctor’s appointments were determined. An independent samples t test analysis was used to determine the relationship between patients’ immunologic status as measured by CD4 count. A P value ≤.05 was considered statistically significant.
Results
Sociodemographic Characteristics and Clinical Markers
Baseline characteristics of the 248 (84.3%) patients who completed the study are shown in Table 1. The mean (SD) age of the patients was 40.4 (8.8) years, 148 (59.7%) were women, 134 (54.0%) were married, 106 (42.7%) had secondary school education, and 208 (56.4%) were employed.
Baseline Characteristics of Study Patients.

As illustrated in Table 2, most (84.7%) diagnoses were made between 2007 and 2008. The mean (SD) baseline CD4 count was 143.5 (92.7) cells/mm3 (range, 4-348 cells/mm3). At baseline, more than half (66.1%) of the patients were on a 12-hourly regimen with the combination of zidovudine + lamivudine + nevirapine being the most (37.5%) prescribed. Almost all (98.8%) patients were placed on cotrimoxazole tablet prophylaxis. It was also observed that the WHO disease stage was not stated by the physician for 87 (35.1%) of the patients.
Baseline Treatment Characteristic of Study Patients (N = 248).

CI, confidence interval; HAART, highly active antiretroviral therapy; HIV, human immunodeficiency virus; WHO, World Health Organization.
Adherence to Doctor’s Appointments and Effect of Changing Model of Care on Patients
With the first model of care, it was observed, as shown in Figure 2, that patients’ adherence to doctor’s appointments decreased as the years increased (51.3%, 35.9%, and 14.9%), but this trend was significantly reversed in 2010 to 93.1% adherence when the second model of care was introduced.

Trend in doctor’s appointment attendance adherence monitoring.
In the first 3 years, weak monitoring of patients’ CD4 counts was also observed. Only 11 (4.4%) had their CD4 count assessed 12 weeks (ie, 3 months) after commencement of ART; 85 (34.3%) were monitored between 3 and 6 months. Monitoring, however, improved in 2010 when the second model of care was introduced. Most (82.3%) patients had at least one CD4 count monitoring that year (Table 3). Retrospective analysis of CD4 count monitoring for 2011 and 2012 was 75.6% and 70.6%, respectively.
Monitoring of Patients’ CD4 Counts.

Assessment of a possible relationship between immunologic status as assessed by the CD4 counts and adherence of these patients using the independent samples t test method of analysis (Table 4) showed that adherent patients had a higher mean CD4 count, but the difference was not statistically significant (P = .4). The paired samples test, however, showed that there was a significant difference between the baseline CD4 count and last CD4 count (Table 5).
Doctor’s Appointment Attendance Measure of Adherence and CD4 Count Group Statistics.a

aUsing Levene’s test for equality of variances and assuming equal variances of the mean CD4 count gave a P value of .4.
Patients’ Baseline and Last CD4 Count Paired Samples Test.a
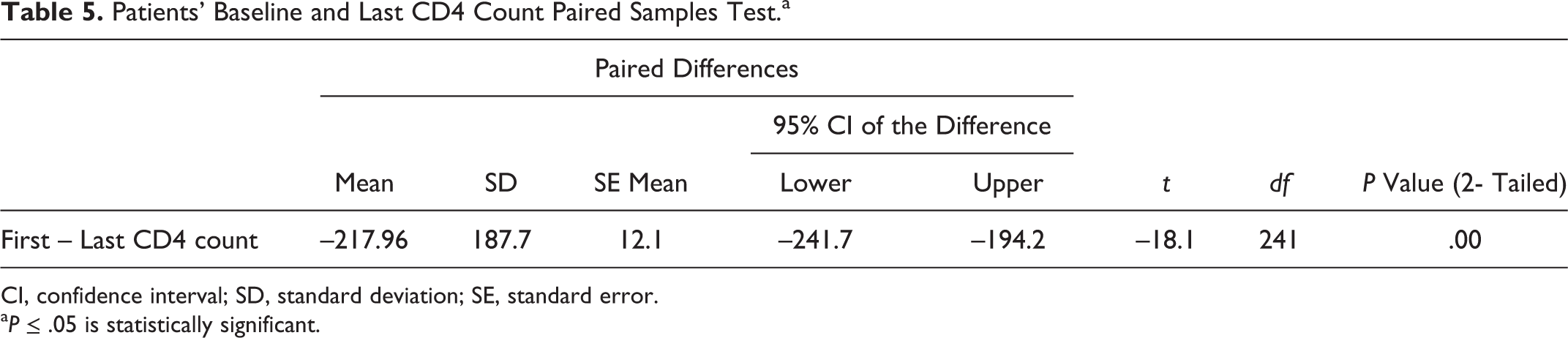
CI, confidence interval; SD, standard deviation; SE, standard error.
a P ≤ .05 is statistically significant.
Predictors of Adherence to Doctor’s Appointments
Predictors of adherence are summarized in Table 6. Throughout the study period, none of the sociodemographic data was a predictor of adherence using the doctor’s appointment attendance measure of adherence.
Effect of Patients’ Knowledge about Human Immunodeficiency Virus and Antiretroviral Therapy on Doctor’s Appointment Attendance Measure of Adherence.a

aB is the coefficient of the variable and P ≤ .05 is statistically significant.
Various aspects of patients’ knowledge predicted adherence in the course of the study. Patients’ knowledge of management, defined as patients’ ability to manage their condition, was a predictor of adherence in 2007; in 2008, patients’ knowledge of adherence was the predictor, while in 2010, it was patients’ knowledge of HIV pathogenesis.
In 2010, most patients’ nonconsumption of alcohol and nonsmoking habits predicted adherence (P < .05), using the doctor’s appointment attendance measure of adherence. However, for this study, only 9 (3.6%) patients were cigarette smokers, and 49 (19.8%) admitted to alcohol consumption.
Patients’ beliefs, disclosure of HIV status, social support, positive behavior, and self-organization had no statistically significant effect on adherence using the doctor’s appointment attendance measure of adherence.
Discussion
In this study, most (74.2%) of the patients were within the age range from 30 to 49 years, with a mean (SD) age of 40.4 (8.8) years (Table 2), which is consistent with HIV and AIDS age prevalence in Nigeria 16 and the mean age obtained in adherence studies carried out in other African countries such as Botswana, 17 Senegal, 18 Kenya, 19 and Nigeria. 20 -26 The higher number of female PLWH observed in this study is also in tandem with the Nigeria Global AIDS Response Country Progress Report, 2 as well as studies carried out in Nigeria, 20 -26 which show higher HIV infection in females than in males.
Results obtained from this study cannot be strictly compared with other studies 10,15 as clinic appointment attendance adherence in other studies had more to do with patients’ drug refills and missed doses. Preintervention patients were “nonadherent” to doctor’s appointments, as defined in this study. Postintervention, the mean doctor’s appointment adherence measure recorded was 93.1%, about the same value as what was obtained from the Ugandan studies. 10,15 These observations indicate that there exists a similar clinic adherence pattern in resource-limited settings.
The mean CD4 counts for adherent patients were higher than those for nonadherent patients, but this was not statistically significant. The inability to link CD4 count with doctor’s appointment attendance adherence occurred because doctor appointment attendance was not synonymous with patients’ drug refills in the first 3 years. As a result, patients cannot be said to be missing their ARV drugs.
The WHO recommended guidelines 16 adopted by the FMOH Nigeria recommends that patients’ monitoring of CD4 count after commencement of ART should be on the 12th week and thereafter every 24 weeks (ie, 6 months). If monitoring was done according to the prescribed schedule, each patient in the course of the study should have been monitored after HAART treatment commencement at least 7 times. Only 15 (6.0%) had CD4 count monitoring up to 7 times, which was not even scheduled as recommended. It was observed that this poor scheduling of assessing patients’ immunologic status still persisted even after the intervention changing the model of care. Weak monitoring of patients’ immunologic status has been shown in earlier studies 18 and explained as a weakness in providing comprehensive care in resource-limited settings. Thus, there is need for intervention designed for both patients and the caregivers to ensure that patients’ CD4 counts are assessed when due before every doctor’s appointment for optimal monitoring and relevant decision making on patients’ management.
In our study and that by Shumba et al, 15 none of the sociodemographic variables had a statistically significant effect on adherence, unlike the study by Kunutsor et al, 10 in which age was a significant predictor of clinic attendance. This reinforces the fact about the dynamic nature of adherence.
Various aspects of the knowledge variable had a significant effect on adherence within the study period. Knowledge of management, knowledge of drug action, and patients’ knowledge of HIV pathogenesis had a statistically significant effect on adherence (P < .05). Such a result has also been shown in other studies 13 that patients’ knowledge of their medication regimen and their understanding of the relationship between nonadherence and buildup of resistance to medication also predict better adherence. The statistical significance with regard to various aspects of patients’ knowledge observed in this study could be as a result of the adherence protocol used by adherence counselors in LASUTH, whereby various aspects of knowledge were addressed during the counseling process before every drug refill.
The consumption of alcohol and cigarette smoking has been shown to be statistically significant determinants or predictors of lower adherence 27,28 ; in the present study, this can also be inferred.
Study Limitations and Strengths
Although this study gives a glimpse of how PLWH assessing a tertiary treatment site in Nigeria are managed, it had some limitations. Accurate doctor’s appointment adherence level could not be determined due to the weak monitoring of the patients’ CD4 counts. As a result, a ≥95% adherence level was assumed. Being an observational study, it was not possible for us to intervene unless the treatment site deemed it fit to do so. Thus, our study had the strength of providing an insight on typical conditions of treatment and care provided at that level of health care in a resource-limited setting. As a result, interventions to correct weaknesses in the model of care can be elucidated, and identified areas of strength can be built on.
Conclusion
The first model of care prior to intervention gave a mean (SD) adherence level of 34.0% (14.8%) using doctor’s appointment attendance. The intervention whereby doctor’s appointment attendance is tied to patients’ drug refills provided a better model of care, which on short-term assessment improved adherence (93.1%) and CD4 cell monitoring. Statistically significant predictors of adherence were patients’ knowledge of drug management, knowledge of adherence, knowledge of HIV pathogenesis, and no alcohol and nonsmoking habits.
Footnotes
Acknowledgments
The authors thank the Lagos State University Teaching Hospital (LASUTH) management, the HIV clinic staff, and all the patients who participated in this study.
Declaration of Conflicting Interests
The author(s) declare no conflicting interest with respect to research, authorship, and /or publication of this article
Funding
The author(s) received no financial support for the research, authorship and publication of this article.