
Abstract
People living with HIV/AIDS (PLWHA) are surviving longer, with an increased risk of cancer. Cancer screening strategies in PLWHA are lacking. We describe the case of a woman with a history of AIDS, who had a nondetectable viral load on treatment. She is an activist, promoting HIV care, but had not undergone routine screening for breast, cervical, or colonic neoplasia. She presented with a left groin mass, which on biopsy proved to be a p16 immuno-histochemical positive squamous cell carcinoma. Anal and cervicovaginal examinations did not show invasive cancer, although high-resolution anoscopy identified high-grade anal dysplasia. A mammogram followed by magnetic resonance imaging showed invasive ductal carcinoma. Her breast cancer was treated with lumpectomy, adjuvant brachytherapy and chemotherapy. The left groin tumor was treated with chemo-radiation. Herein, we also review medical literature concerning anal, cervical, breast, colorectal, and lung cancer screening for PLWHA, which is important for our aging population of PLWHA.
People living with HIV/AIDS (PLWHA) have an increased risk of cancer. 1,2 This was appreciated early in the AIDS epidemic when a dramatic increase in Kaposi’s sarcoma (KS), intermediate and high-grade peripheral B-cell non-Hodgkin lymphoma (NHL), primary central nervous system NHL, and invasive cervical cancer (ICC) were identified in HIV-infected individuals. By the 1980s, these tumors were designated by the US Centers for Disease Control and Prevention (CDC) as AIDS-defining cancers (ADCs). 1 Even before the widespread implementation of highly active antiretroviral therapy (HAART), the incidence of KS and NHL had begun to decline significantly, and this trend has continued over the past 20 years. 3 Non-ADCs now outnumber ADCs and are an increasingly important cause of morbidity and mortality. 4,5
Cancers in PLWHA are often characterized by earlier age at onset, atypical pathology (including higher tumor grade), more aggressive clinical behavior, and more advanced stage at presentation. 6,7 For many non-ADCs, such as lung cancer and other aerodigestive malignancies, the occurrence of cancer is linked in part to lifestyle choices, such as tobacco use and alcohol consumption. 2 Coinfection with other viruses including hepatitis B and C viruses and human papillomavirus (HPV) can result in additive risks for liver cancer and squamous cell cancers of the anus (SCCA) and of the head and neck. 4 Squamous cell cancers of the anus share multiple similarities with cervical cancer, such as HPV being the predominant causative agent, and HPV-16 the most frequent serotype associated with neoplasia. 8 The relative risk of SCCA in HIV-infected women and men is approximately 30- to 80-fold greater than HIV seronegative age- and sex-matched controls. 9 Women with HIV also have a higher incidence of ICC compared to non-HIV-infected women. 10 The incidence of ICC increases in HIV-infected women as their degree of immunosuppression increases, as suggested by an elevated incidence rate ratio of 2.3, 3.0, and 7.7 when CD4 counts are greater than or equal to 350 cells/mm3, between 200 and 349 cells/mm3, and less than 200 cells/mm3, respectively, compared to age-adjusted HIV-uninfected women. 10
The CDC has noted that the number of PLWHA in the United States has steadily been increasing, and by the end of 2012 was roughly 1 218 400. 11 The highest prevalence rate of HIV occurred within the age-group of 45 to 55 years. With aging, this population will be vulnerable to tumors whose incidence increases with age, such as prostate cancer in men, breast cancer in women, and colon and lung cancers in both men and women. 12 This underscores the importance of cancer surveillance and screening in this vulnerable population.
We present the case of an HIV-infected woman with both high-grade anal intraepithelial neoplasia (HGAIN) and high-grade cervical intraepithelial neoplasia (CIN). She presented to medical attention with an enlarged left inguinal node. At surgery, the node revealed poorly differentiated squamous cell histology and on immuno-histochemical staining was strongly positive for p16, a biomarker associated with HPV E6/E7 mediated cellular proliferation. 13 In the course of her evaluation, she was also diagnosed with an early stage breast carcinoma. The salient point of her story includes a trail of activism, as she promoted HIV medical care for women in her community, yet she herself had not undergone colonoscopy, recent cervical or anal pap evaluation, or mammography. Her case underscores the importance of cancer screening for PLWHA.
Case Report
In 2013, a 53-year-old African American female, with a 25-year history of AIDS, a nadir CD4 count of 5 cells/mm3, and a past history of high-grade vulvar intraepithelial neoplasia (VIN) and CIN, sought medical attention for a hard mass in her left groin of 6 months duration. Seven years prior, she had been identified with VIN and CIN. Her VIN was treated with laser ablation, and her CIN was treated with loop electrosurgical excision.
In the early years of her AIDS diagnosis, she was poorly compliant with medical care, took HIV medications sporadically, and had been hospitalized with Pneumocystis jiroveci pneumonia and AIDS-associated wasting. Ten years ago, she remarried and began to take heightened responsibility for her medical care, which included taking her medications more consistently. Despite multidrug HIV resistance, over the past 7 years, she had responded to salvage HAART, which consisted of darunavir boosted with ritonavir (RTV), etravirine, and raltegravir. Her most recent CD4 count was 817 cells/mm3 and her HIV viral load was <4×104 copies/mL.
With the exception of a left groin mass that measured 1.5 × 2.0 cm, her general examination and bimanual pelvic examination were unremarkable. Her Pap smear showed normal appearing cervical cells which stained negative for p16 by immuno-histochemistry. A left vulvar biopsy showed high-grade VIN. Perianal examination was abnormal, showing flat appearing perianal condylomata and patchy hypopigmentation around the anal verge. High-resolution anoscopy (HRA) demonstrated condylomata acuminate, and biopsies showed HGAIN. Further evaluation included a whole body 18 F-fluorodeoxyglucose (FDG) positron emission tomography (PET) and computed tomography (CT). The 18 FDG-PET-CT showed a prominent 2 cm left groin node with a maximum standardized uptake value of 4.1 (Figure 1). An excisional biopsy of the mass revealed a poorly differentiated squamous cell carcinoma, which on immunostaining was positive for p16 (Figure 2).
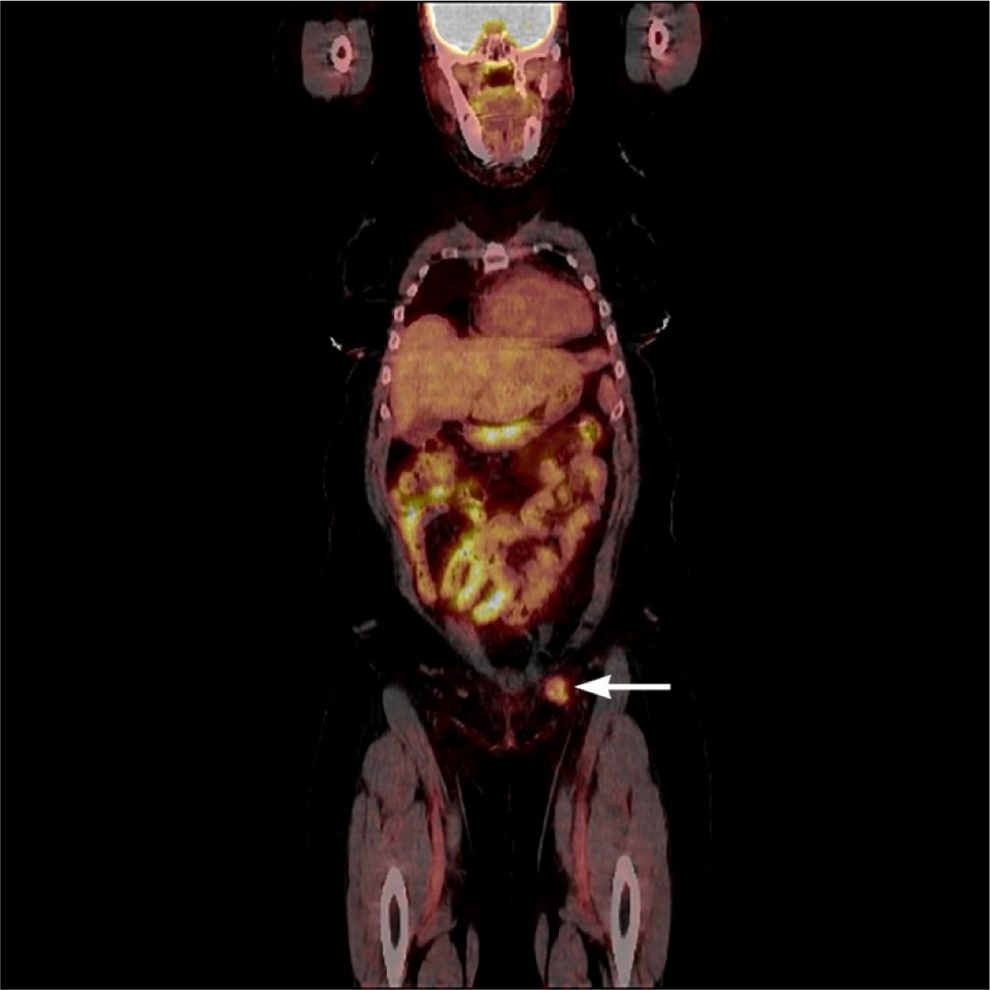
18 FDG-PET-CT from skull base to mid-thigh, coronal view. Enlarged left inguinal lymph node measuring approximately 27 × 20 mm with mildly increased activity, denoted by white arrow.

Hematoxylin and eosin staining of left inguinal node showing squamous cell carcinoma at 20× magnification. Insert: Positive P16 immunohistochemical stain of the left inguinal node.
Complete blood count, chemistry, and liver enzyme panels were all within normal limits, but her mammogram showed a right breast mass which on magnetic resonance imaging measured 15 × 6 × 6 mm in size. Subsequent needle biopsy demonstrated an invasive ductal carcinoma, with high mitotic count, but no lymphatic invasion, no tubule formation, and no ductal carcinoma in situ. She subsequently underwent right partial mastectomy. Her tumor measured 12 × 7 × 6 mm, and a single sentinel node was without cancer (stage T1bN0). The tumor was estrogen and progesterone receptor negative and did not overexpress human epidermal growth factor receptor 2 by gene amplification using fluorescence in situ hybridization. Postlumpectomy, she received adjuvant intraoperative brachytherapy to the breast tumor bed, at a dose of 2000 cGy. The pros and cons of additional adjuvant chemotherapy directed at her breast cancer were discussed, and a joint decision by the patient and her medical team was made to pursue additional chemotherapy. Once she had recovered from her initial treatment and restaging studies, she is to receive 12 weeks of weekly paclitaxel at a dose of 80 mg/m2 given together with weekly trastuzumab followed by an additional 9 months of trastuzumab delivered every 3 weeks.
For her cancer of unknown primary (CUP), most likely arising from either the anal canal, vagina, or cervix, she received intensity-modulated radiation therapy to the pelvis, inguinal lymph nodes, and anal region (180 cGy per fraction for 28 fractions, for a total of 5040 cGy). Systemic treatment consisted of concurrent 5-fluorauracil (1000 mg/m2 via continuous infusion on days 1-4 and 29-33) and mitomycin C (10 mg/m2 as an intravenous push on days 1 and 29). Her treatment was complicated by moderate nausea, mild perianal and left groin desquamation, dermatomal shingles, and short-lived pancytopenia. Breast cancer treatment was complicated by several episodes of diverticulitis. Six months postchemotherapy completion, she underwent a colonoscopy where benign polyps were retrieved. She is currently disease free 18 months after initial CUP diagnosis.
Discussion
The introduction of HAART has transformed HIV/AIDS into a chronic medical condition. Newly infected individuals with access to HAART have experienced a significant reduction in excess mortality compared to those diagnosed in the early years of the AIDS epidemic. 14 In the United States, the median age of PLWHA is 50 years. With this change in demographics, a paradigm shift is taking place in the type of cancers that are now seen in this population. In 2010, an estimated 7760 cancers occurred among PLWHA, one-third of which were ADCs and two-thirds of which were non-ADCs. 15 This illustrates the importance of matching cancer screening and surveillance with the changing needs of this population to reduce the incidence of these cancers and their associated morbidity and mortality.
Our patient, although now 55 years of age, had never undergone breast cancer screening and had not received recent routine gynecologic care. She presented to cancer care after moving from North Carolina to Washington State and revealing to her medical providers that she had a groin lump of 6 months duration. It is difficult to be certain as to where her tumor originated. Potential primary sites include anus, cervix, or vagina, but given that cervical and vaginal samplings were negative for high-grade changes, and the anal biopsies more clearly showed high-grade dysplastic changes, we believe the anus to be the most likely site of cancer origin.
Anal cancer is a non-ADC, the incidence of which in PLWHA has far exceeded the expected results. 15 The little attention anal cancer has received may, in part, be due to the low incidence of this tumor in the general population, which is estimated to be approximately 1 to 2 per 100 000. 16 Survival from anal cancer significantly improves when it is diagnosed at an earlier stage; however, most anal cancers are detected when they are locally advanced. 16 A central argument for anal cancer screening, in addition to its increased incidence and mortality in the HIV population, is the biological similarity between the cervix and the anus. 15 Both anatomical areas include a transition zone and squamous cell epithelium, with the propensity for HPV infection. High-resolution anoscopy can be likened to colposcopy, allowing visual identification of dysplastic lesions and the ability to biopsy suspicious lesions. 17 It is plausible that the benefits of cervical cancer screening in women could be implemented for the anus and be beneficial in similar ways for both men and women with HIV/AIDS.
Although similarities between anal and cervical cancer screening can be argued, outcome research into anal cancer screening is lacking. 15,17 Different screening approaches include digital anal rectal examination (DARE), anal Papanicolaou test, and HRA. Unfortunately, there is no randomized control trial (RCT) to ascertain the reliability and validity of anal cancer screening, nor evidence of improved survival rates from anal cancer screening. 15,16 There is also no general agreement on who should be screened with DARE. 16 Evidence is still lacking regarding the sensitivity, specificity, negative predictive value, positive predictive value, or the quality of life and costs associated with false-negative and false-positive DARE. Also among the many barriers to the widespread use of HRA are the paucity of highly trained anoscopists, the challenges of getting insurance carriers to cover this procedure, and variations in interpreting biopsy specimens. Ironically, the CDC does note that anal cytology screening is a useful preventive measure in PLWHA, but they have qualified this notation by pointing to the need for further studies addressing screening and treatment programs. 18
Although consensus guidelines are lacking, one financial analysis came out in favor of anal cancer screening. Researchers estimated that biennial screening of HIV-infected women would account for a 4.4-year increase in quality-adjusted life years (QALY), at an incremental cost-effectiveness ratio of $34 763 (USD) per life-year gained compared to no screening. 19 Other researchers also estimated that yearly anal Papanicolaou test for HIV-infected men who have sex with men would translate to $16 000 (USD) per QALY gained compared to no screening. 20
A National Institutes of Health funded study will hopefully shed more light on the utility of anal cancer screening. The Anal Cancer/High-Grade Squamous Intraepithelial Lesion Outcomes Research (ANCHOR) Study is a phase 3 multicenter RCT currently enrolling HIV-sero-positive individuals of at least 35 years of age and who have not received prior therapy for HGAIN. One-half of the participants will have their HGAIN treated and the other half will be monitored carefully but not receive active treatment unless they develop SCCA. The primary outcome is time from randomization to anal cancer diagnosis. 21 Secondary end points include incidence of adverse events subsequent to treatment and quality of life. Treatment arms include imiquimod, fluorouracil, infrared photocoagulation, thermal ablation, and laser therapy.
Our patient’s case also highlights the importance of breast cancer screening in HIV-positive women. Breast cancer is the second leading cause of cancer death in women. 22 The importance of breast cancer screening in the general population is widely accepted. The US Preventive Services Task Force (USPSTF) currently recommends biennial screening mammography between 50 and 74 years of age for women, with the caveat that those younger than 50 can pursue earlier screening depending on the individual, with consideration of benefit versus harm. 23 The CDC recommends mammographic screening every 2 years for women between 50 and 74 years of age and an individualized discussion with the physician regarding screening between 40 and 49 years of age. 24 In contrast, the American Cancer Society (ACS) recommends that women with an average risk of invasive breast cancer undergo regular mammography starting at 45 years old, with annual mammography from 45 to 54 years old, and biannual mammography with the opportunity to continue screening annually as long as the woman’s overall health is good, and as long as her life expectancy remains 10 years or longer. 25 The ACS also recommends that women be given the opportunity to begin annual screening from 40 to 44 years old. Breast cancer screening recommendations differ between the USPSTF, CDC, and ACS (Table 1).
Recommendations for Breast Cancer Screening Mammography: USPSTF, CDC, and ACS.

ACS, American Cancer Society; CDC, Centers for Disease Control and Prevention; USPSTF, US Preventive Services Task Force.
The epidemiology of breast cancer in HIV-infected women may be changing. During the HAART era, the incidence of breast cancer in HIV-infected women is approaching that of the general female population, where it had once been thought to be much less. 22 Small studies have shown a younger median age of 46 years old in HIV-positive women, at time of breast cancer diagnosis, compared to 61 years old in the general population at time of breast cancer diagnosis. In a recent retrospective chart review at the University of Miami/Jackson Memorial Medical Center, between January 1, 1989, and December 31, 2013, 47 HIV-infected females were identified with breast cancer. Breast cancer–specific survival for these HIV-infected women appears inversely associated with initial stage, showing 100% survival for stage I, 66% for stage II, 43% for stage III, and 0% for stage IV, over a 5-year period after diagnosis of breast cancer. This highlights the importance of further research into breast cancer in the HIV population, given that the incidence may be approaching that of the general population, and it is unclear whether current screening guidelines are applicable to women living with HIV/AIDS.
Our patient also had not undergone colorectal cancer (CRC) screening. Colorectal cancer is the third most common cancer for both women and men and is the second leading cause of cancer death when both genders are combined. 12 The USPSTF recommends screening for CRC between the age of 50 and 75, using high-sensitivity fecal occult blood test (FOBT), sigmoidoscopy, or colonoscopy. 26 Intervals for screening vary depending on which modality is used. Fecal occult blood test can be repeated yearly. Sigmoidoscopy can be repeated every 5 years, with the use of FOBT every 3 years. Colonoscopy can be repeated every 10 years. The CDC also notes that earlier screening intervals may be needed if the person or close relative have had colorectal polyps or CRC, inflammatory bowel disease, familial adenomatous polyposis, or Lynch syndrome. 27
In PLWHA, the prevalence of colonic adenomas may be increased. 28 For example, in a prospective CRC screening study, the prevalence of adenoma or adenocarcinoma of the distal colon was 26% for HIV-infected patients compared to 13% for controls, a statistically significant difference. 29 Additionally, the incidence of CRC in PLWHA during the HAART era appears comparable to that of the general population. 28 Yet CRC screening in the HIV population is employed less frequently than in the general population. Among 205 consecutive patients interviewed in outpatient clinics with either average risk of CRC as defined as age greater than or equal to 50 years old or high risk for CRC as defined as having a family history or personal history of colon cancer or adenomas, those who were HIV positive were significantly less likely to undergo CRC screening (41% versus 67%). 30 Those who were HIV sero-positive and who had >10 annual clinic visits were more apt to receive up-to-date CRC screening. The reasons for the disparity between CRC screening in PLWHA, and non-HIV patients, are likely multifactorial, including patient and physician education regarding CRC screening, lack of CRC screening guidelines for PLWHA, and health care disparities which are more frequent in this population. 31 Further research is needed to help clarify the appropriate CRC screening in PLWHA, particularly pertaining to modality, initiation, and frequency of screening. 28
Our patient had undergone cervical cancer screening but had been lost to gynecologic care for several years when she presented to our clinic. The current guidelines for cervical cancer screening by the USPSTF published in 2012 include women from 21 to 65 years old. Grade A recommendations include a Papanicolaou test, every 3 years between 21 and 65 years old, or cytology with HPV testing every 5 years between 30 and 65 years old. 32 This recommendation does not include those with precancerous cervical lesions, in utero exposure to diethylstilbestrol, or those with immunosuppression such as HIV positivity.
In a multicohort analysis between 1996 and 2010, data from the North American AIDS Cohort Collaboration on Research and Design suggested that HIV-infected women had higher risk of incidence of ICC compared to HIV-uninfected women, and that this risk increased as the CD4 counts declined. 10 Yet in an interview study which lasted 4 years and encompassed 18 states, approximately a quarter of the 2417 HIV-infected women reported not receiving cervical cancer screening within the previous year. 33 For women with HIV infection, the CDC recommends cytology screening every 6 months after initial diagnosis of HIV, and if both tests are normal, then annual screening. 34 Although screening guidelines for cervical cancer in PLWHA are more defined compared to other cancer screening modalities for this population, a large proportion of these patients are not receiving state-of-the-art gynecological care.
Lung cancer is the leading cause of cancer death in the United States in both men and women, and with an estimated 158 000 deaths for 2015, it accounts for approximately 27% of cancer-related deaths. 12 The USPSTF released a Grade B lung cancer screening recommendation in December 2013 stating, annual screening for lung cancer with low-dose CT (LDCT) in adults aged 55 to 80 years who have a 30 pack-year smoking history and currently smoke or have quit smoking within the past 15 years, and that screening should be discontinued once a person has not smoked for 15 years or develops a health problem that substantially limits life expectancy or the ability or willingness to have curative lung surgery. 35
Although our patient did not meet the current screening guidelines for lung cancer, it is clear that lung cancer is overrepresented in PLWHA. 15 The incidence rate ratio for lung cancer in HIV-infected individuals compared to HIV-uninfected individuals is as high as 6.9 in the United States. 36 In 2010, the estimated percentage excess of lung cancer cases in PLWHA was approximately 52%. 15 Currently, there are no lung cancer screening guidelines for PLWHA. Further research is required to address the utility of lung cancer screening and the associated efficacy and efficiency of the different screening modalities in this high-risk population. Research is also lacking regarding the physical, financial, and psychological consequences of lung cancer screening in PLWHA.
When we consider cancer screening in our patient, it is difficult to know what the results may have been if testing had occurred routinely, and whether this would have led to earlier detection of our patient’s breast cancer and left groin CUP. One of the important ironies of our patient’s medical care is that she had been a strong and passionate advocate within her community for access to medications to combat HIV infection; yet, she was unaware of the importance of general cancer screening and had not undergone widely accepted age-appropriate cancer screening (Table 2). Her experience underscores the importance of cancer screening education, not just for physicians, but for patients as well. However, for PLWHA, appropriate guidance in the form of evidence-based recommendations is lacking. Research is still needed, with emphasis on high-value screening strategies rather than high-intensity screening approaches. 37 It is our hope that a balance can be struck between the benefits of earlier detection of life-threatening cancers (whose treatment can alter the disease course) and the harms, costs, and psychological effects of screening. 37
Age-Appropriate Cancer Screening Guidelines.

Abbreviations: ACS, American Cancer Society; CDC, Centers for Disease Control and Prevention; FOBT, fecal occult blood test; HPV, human papilloma virus; USPSTF, US Preventive Services Task Force.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.