
Abstract
Objectives:
We sought to characterize recent cases of toxic epidermal necrolysis (TEN) in HIV-infected patients at San Francisco General Hospital (SFGH), a large HIV referral center.
Methods:
This was a retrospective analysis of HIV-infected patients diagnosed with TEN from January 2001 to May 2014 at SFGH.
Results:
Ten cases of TEN were identified, 50% of which occurred in HIV-infected individuals. Among the HIV-associated cases, causative agents were trimethoprim–sulfamethoxazole (TMP-SMX; n = 2), atovaquone, clindamycin, and fluconazole. No antiretroviral agents were implicated.
Conclusion:
Although limited by small sample size, our experience is reflective of the well-recognized increased incidence of TEN in HIV-positive patients and suggests that antimicrobial agents, particularly TMP-SMX, are the most common causative agents in this population. As 3 of the 5 HIV-associated TEN cases were caused by potentially inappropriate or unnecessary use of antibiotics, our experience highlights the importance of judicious use of systemic medications in populations susceptible to severe adverse drug reactions.
Introduction
Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) are potentially life-threatening disorders characterized by widespread erythema, necrosis, and bullous epidermal detachment of the skin and mucosa. These disorders exist on a spectrum and are differentiated primarily by varying degrees of body surface area involvement. TEN lies at the more severe end of the spectrum with greater than 30% detachment, while SJS is characterized by greater than 10% detachment. An SJS/TEN overlap syndrome is diagnosed for intermediate cases. 1 While TEN almost exclusively represents adverse drug reactions, SJS can, less commonly, result from exposure to a variety of infectious agents. Extracutaneous complications of SJS and TEN, resulting from the involvement of other epithelial surfaces, are not uncommon. While the eyes are most commonly affected, the gastrointestinal, respiratory, or genitourinary systems can all be involved. 1
HIV infection is a well-known risk factor for the development of SJS and TEN, with HIV-infected individuals having up to a 1000-fold increased risk compared to the general population. 2 While sulfonamide antibiotics, and specifically trimethoprim–sulfamethoxazole (TMP-SMX), are thought to be the most common cause of SJS and TEN in HIV-infected individuals, other commonly implicated medications include analgesics, antiepileptics, allopurinol, and other (nonsulfa) antibiotics, 3,4 mirroring the trends seen in HIV-negative patients. Although much more rare, a number of reports have also linked antiretroviral (ARV) medications to the development of SJS and TEN in HIV-infected patients. Nevirapine (NVP) appears to be the most common ARV-associated cause of SJS and TEN, with 1 study reporting a 0.3% risk. 5 -12
While patients with HIV are, for the purposes of prophylaxis against or management of opportunistic infections, more likely than their HIV-negative counterparts to be prescribed predisposing medications, this factor alone does not appear to completely account for the increased susceptibility to SJS and TEN in HIV-infected patients. 13 Although immune dysregulation is likely involved, the precise mechanisms by which HIV-infected individuals are predisposed to the development of SJS and TEN remain unclear.
Despite the increased risk of TEN in HIV-infected individuals, no randomized controlled trials or case–controlled studies exist to evaluate and compare potential treatment modalities in this vulnerable population. This likely stems from the rarity of TEN itself compounded by the institutional and geographic dispersion of patients with HIV. San Francisco General Hospital (SFGH) is one of the largest HIV referral centers in the United States and serves more than one-third of San Francisco’s HIV-positive population. Accessibility to a large cohort of HIV-positive individuals at 1 institution provides a unique opportunity to more fully explore TEN within this population. Herein, we report our 13-year experience with TEN in HIV-positive patients at SFGH, with the hope that this report encourages further research as well as reflection on ongoing controversies in the management of these patients.
Methods
After appropriate institutional review board approvals, 10 cases of TEN at SFGH were identified retrospectively through queries of the electronic medical record and pathology records dating from January 2001 to May 2014. Search terms included “toxic epidermal necrolysis,” “TEN,” “Stevens-Johnson syndrome,” “Steven-Johnson syndrome,” “SJS,” and “erythema multiforme.” All cases of TEN were diagnosed clinically according to established criteria and confirmed by histological evaluation. For the sake of purity of analysis, this article is focused on TEN and its management. While noted, cases of SJS and SJS/TEN overlap were excluded, as these milder cases are not always biopsied, can sometimes be caused by infectious agents rather than systemic medications, and are often managed differently than cases of TEN. SCORe of Toxic Epidermal Necrolysis (SCORTEN) calculations were made for each case using data from the first 24 hours of admission. Annual SFGH census data summarizing the number of patients seen in both inpatient and outpatient settings were collected from the Quality Data Center at SFGH. Unfortunately, data delineating the number of unique visits by HIV-positive patients were not available.
Results
Over the past 13 years (January 2001 to May 2014), there were 10 confirmed cases of TEN at SFGH, 5 of which occurred in HIV-positive individuals. Demographic information for all cases of TEN is presented in Table 1. Table 2 summarizes the details of each of the 5 HIV-associated cases of TEN. Medications implicated in the development of TEN in our HIV-positive cohort during this time were TMP-SMX (n = 2), atovaquone (n = 1), clindamycin (n = 1), and fluconazole (n = 1). Clinically confirmed cases of TEN in HIV-positive individuals had a mean age of 49 years, CD4 count of 265=cells/mm3, and viral load of 400 K copies/mL. Overall, SCORTEN calculations estimated a mortality rate of 24.2% in the HIV-positive cohort and 19.6% in the HIV-negative cohort, with actual mortality rates being 40% for both the groups.
Demographic Information for Toxic Epidermal Necrolysis Patients at SFGH (2001-2014).
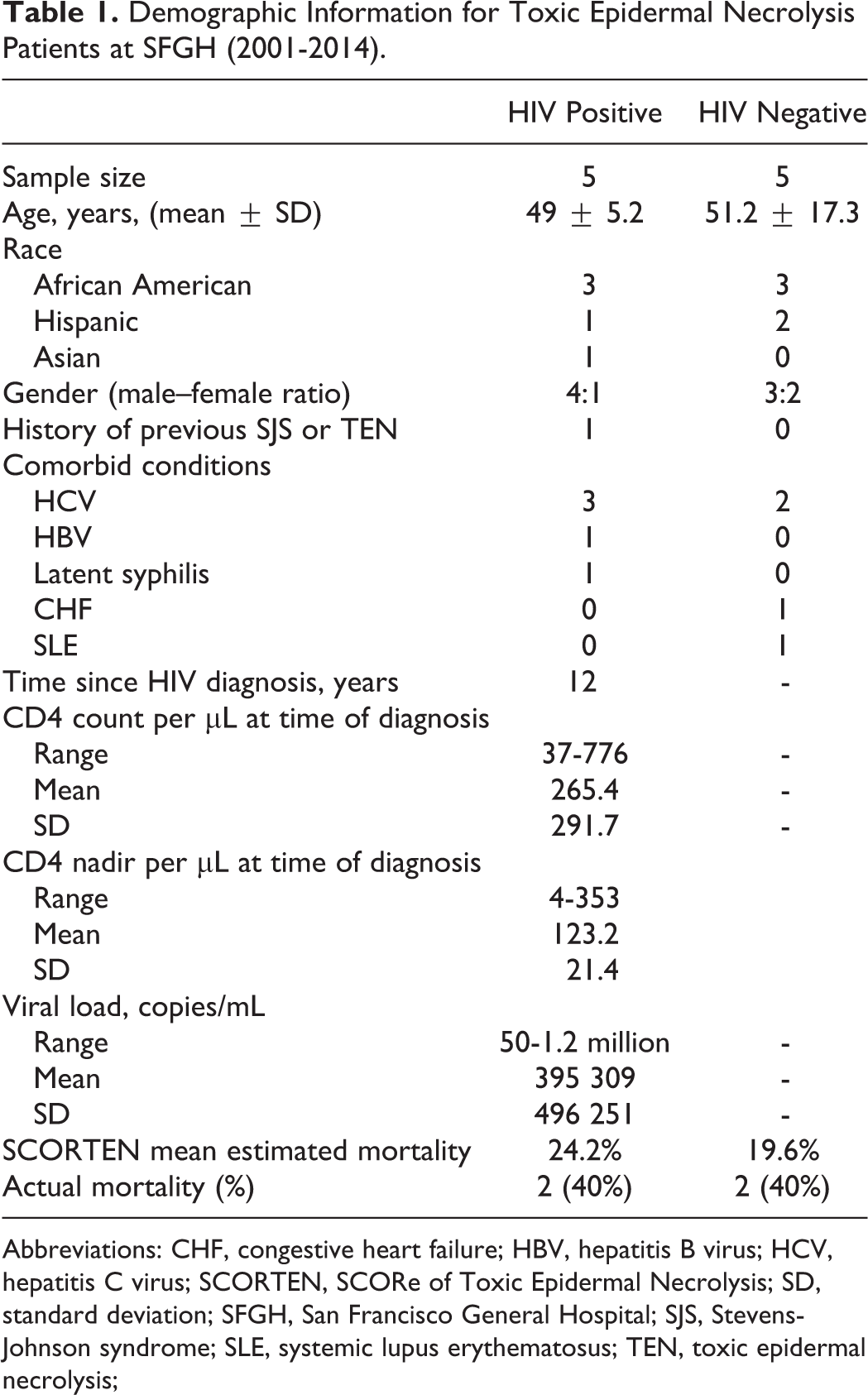
Abbreviations: CHF, congestive heart failure; HBV, hepatitis B virus; HCV, hepatitis C virus; SCORTEN, SCORe of Toxic Epidermal Necrolysis; SD, standard deviation; SFGH, San Francisco General Hospital; SJS, Stevens-Johnson syndrome; SLE, systemic lupus erythematosus; TEN, toxic epidermal necrolysis;
Cases of HIV-Associated Toxic Epidermal Necrolysis at SFGH (2001-2014).

Abbreviations: 2/2, secondary to; AA, African American; F, female; G6PD, glucose-6-phosphate dehydrogenase deficiency; H, Hispanic; HBV, hepatitis B virus; HCV, hepatitis C virus; HTN, hypertension; IVIG, intravenous immunoglobulin; M, male; MAC, mycobacterium avium complex; ppx, prophylaxis; PSA, polysubstance abuse; S/p, status post; SCORTEN, SCORe of Toxic Epidermal Necrosis; SFGH, San Francisco General Hospital; TMP-SMX, trimethoprim-sulfamethoxazole; URI, upper respiratory tract infection.
aAll patients received aggressive supportive care including IV hydration, topical antibiotics, and topical emollients.
Discussion
Although SFGH is the medical home for more than 3000 HIV-infected individuals, it is perhaps still not surprising that only 5 cases of HIV-associated TEN were documented over a 13-year period, given the overall rarity of TEN. Precise incidence rates were not calculated due to a lack of HIV-specific annual census data. Nonetheless, given that the vast majority of patients seen at SFGH are HIV negative, the fact that half of our patients with TEN were HIV-positive seems to mirror the well-recognized trend toward an increased incidence of TEN in patients with HIV.
Consistent with prior reports, TMP-SMX was the most common medication to cause TEN in our HIV-infected cohort. Although several ARV agents have been reported to cause TEN, with the exception of NVP, induction of TEN by ARV agents is an uncommon occurrence. To this effect, no ARV medications were implicated in the 5 cases of HIV-associated TEN at our institution.
All patients with TEN at our institution received aggressive supportive care, including intensive nursing, intravenous hydration, meticulous wound management, and appropriate specialty consultations. Despite the fact that the role of systemic immunomodulators in the treatment of TEN remains controversial, all of our patients also received intravenous immunoglobulin (IVIG) at doses of 1 to 1.5 mg/kg daily for 4 to 5 days. Intravenous immunoglobulin was thought to be mechanistically promising in the treatment of TEN because of its ability to block Fas-Fas ligand binding, a process that has been proposed to play a role in keratinocyte apoptosis. Because of this, and encouraging early data suggesting a survival benefit, IVIG became a widely used treatment for TEN at many institutions in the last decade, largely replacing systemic corticosteroids. 13,14 Nonetheless, it is worth noting that the 2 published meta-analyses evaluating IVIG in the treatment of TEN reached different conclusions regarding whether there is a dose-dependent survival benefit. 15,16 For now, the standard of care remains immediate discontinuation of causal medications and aggressive supportive care, ideally in the setting of an intensive care unit or a burn unit.
Although the role of IVIG, and other systemic agents, in the management of TEN remains unclear in general, there is even less data specifically examining the use of systemic immunomodulators in the treatment of HIV-associated cases of TEN. More HIV-specific data are needed to evaluate the safety profile and efficacy of these therapies in this vulnerable population. Moreover, as the potential use of systemic immunomodulators in patients with HIV to reduce virally induced immune activation has recently become a topic of active investigation, it is also important to assess whether immunomodulatory therapies used in the treatment of HIV-associated TEN have subsequent effects on inflammatory markers, HIV-related parameters, and long-term outcomes in TEN survivors.
The SCORTEN calculations underestimated actual mortality rates in both our HIV-positive and HIV-negative TEN cohorts. While SCORTEN is a well-established severity-of-illness score for TEN, to date, only 1 study has validated this measure in a cohort with high rates of HIV infection. 17 HIV-specific validation of SCORTEN would be beneficial, as predictors of morality in patients with HIV may be different than those in the general population.
Finally, this study highlights the importance of judicious use of systemic medication in patients, particularly in those populations who are predisposed to severe adverse drug reactions. Indeed, 3 of the 5 cases of HIV-associated TEN seen at our institution were caused by potentially inappropriate use of antibiotics (Table 2). Patient 2 had a known history of SJS due to TMP-SMX but was given the same medication for what was a mild, likely viral, upper respiratory infection. Patient 5 was given fluconazole by his primary care provider for an axillary rash that, on follow-up examination after discharge, was determined to be seborrheic dermatitis. This patient was left with residual visual deficits due to ocular involvement. Patient 4 was given clindamycin after an incision and drainage of an uncomplicated axillary abscess. This patient ultimately died from TEN-associated multiorgan system failure.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.