
Abstract
Improved understanding of cholesterol levels in HIV- and hepatitis C virus (HCV)-infected persons in Argentina will guide optimal antiretroviral therapy. The authors conducted a cross-sectional study in Argentina to describe associations between HIV, HCV, and cholesterol. Of the 202 participants, 21 were HIV infected, 15 were HCV infected, 46 were HIV/HCV coinfected, and 120 were HIV/HCV uninfected. HIV/HCV-uninfected participants had the highest total cholesterol (TC) and low-density lipoprotein (LDL) levels. Multivariate modeling revealed that HIV/HCV-coinfected patients had the lowest TC levels (−28.7 mg/dL, P < .001) compared to the HIV/HCV-uninfected reference group. Hepatitis C virus and HIV/HCV coinfection were associated with lower LDL levels (−21.4 mg/dL, P = .001 and −20.3 mg/dL, P < .0001, respectively). HIV and HIV/HCV coinfection, but not HCV alone, were associated with lower high-density lipoprotein levels (−9.1 mg/dL, P = .0008 and −6.8 mg/dL, P = .0006, respectively). Further study is needed to examine whether the more favorable lipid profile observed in HIV/HCV-coinfected persons is associated with a reduction in cardiovascular risk.
Introduction
As HIV-infected persons are living longer as a result of highly active antiretroviral therapy (HAART), 1 research efforts have focused on the effects of HIV and its treatment on major comorbid conditions including dyslipidemia and cardiovascular disease. Specific alterations in lipid profiles have been described in persons with HIV. Studies conducted early in the HIV epidemic, prior to the availability of HAART, noted increased triglycerides (TGs) and reduced high-density lipoprotein (HDL) among persons with untreated, advanced HIV infection. 2,3 Initiation of HAART has been associated with increases in total cholesterol (TC), low-density lipoprotein (LDL) cholesterol, and HDL cholesterol as well as further elevation in TGs. 3 The atherogenic lipid profile associated with HAART often requires switching of antiretroviral agents or initiation of lipid-lowering therapy to mitigate increased cardiovascular risk. 4
HIV and hepatitis C virus (HCV) often coexist due to shared transmission risks. In drug-using populations, the rates of coinfection approach 75%. 5,6 Hepatitis C virus infection is associated with lower TC, lower LDL cholesterol, and insulin resistance. 7 –10 Further, studies conducted in drug-using populations in the United States have demonstrated that, after initiation of HAART, HIV/HCV-coinfected persons do not experience elevations in TC and LDL cholesterol to the extent seen in HIV-monoinfected persons. 11,12 Nonetheless, whether the reduced cholesterol associated with HCV confers a reduction in cardiovascular risk remains unclear.
HIV-related global health efforts focus on access, delivery, and management of HAART in developing nations. In 2014, it was estimated that 130 000 persons were living with HIV in Argentina. 13 The prevalence of HIV infection among injection drug users in Argentina ranges from 27% to 80%. 14 The epidemic is largely concentrated in urban areas, with approximately 80% of cases in Buenos Aires. 15 Although there have been several reports of hypertriglyceridemia, insulin resistance, and cardiovascular disease in HIV-infected persons in the United States, 16 –18 less is known regarding the metabolic profile of HIV-infected persons in Argentina.
As such, we sought to examine nutritional status and serum lipids in HIV- and/or HCV-infected Argentinean drug users. Improved understanding of the effect of HIV and/or HCV on cholesterol levels in this subgroup will guide the selection of optimal antiretroviral regimens and will better enable physicians in Argentina to manage HAART-related toxicities and modify cardiovascular risk. The primary objective of this study is (1) to provide descriptive data regarding nutritional status and cholesterol levels in HIV- and/or HCV-infected drug users in Argentina, a population that has not been well studied and (2) to examine the association of HIV and HCV on cholesterol levels in a cohort of Argentinean drug users.
Materials and Methods
As part of a cross-sectional study to describe the associations between HIV infection, drug use, comorbidities, and nutritional and metabolic abnormalities, 202 participants were enrolled from 2007 to 2008 at 2 sites in Buenos Aires: the Fundación de Ayuda al Inmunodeficiente (FUNDAI) HIV/AIDS clinic at the Hospital Muñiz and Centro Nacional de Reeducación Social (CENARESO), a national drug rehabilitation center. Participants were eligible if they were between 18 and 65 years of age and had injected, smoked, or snorted cocaine or coca paste in the past 5 years. Female participants who were pregnant (determined by self-report) were excluded. Persons who agreed to participate signed informed consent and underwent pretest counseling and HIV testing. The protocol was approved by the institutional review boards of CENARESO, FUNDAI, and Tufts Medical Center, Boston, MA, USA.
Participants completed a standardized questionnaire that collected data regarding sociodemographics, medical history and medication use, illicit drug use, and 24-hour dietary recall. The frequency and amount of alcohol intake over the past 30 days were assessed. Responses were categorized as hazardous or nonhazardous using the National Institute on Alcohol Abuse and Alcoholism guidelines. 19 Body composition measurements, including height and weight, and blood samples, including fasting lipid profile (TC, HDL cholesterol, LDL cholesterol, and TGs), were also obtained. For HIV-infected participants, CD4 count and HIV viral load were also measured.
Hepatitis C antibody was detected using IMx-HCV (version 3.0; Abbott, Buenos Aires, Argentina). HIV-1 status was determined by enzyme-linked immunosorbent assay (IMx EIA HIV-1/HIV-2 III Plus; Abbott), with confirmation by Western blot (HIV Blot 2.2; Genelabs Diagnostics, Singapore Science Park, Singapore). HIV-1 viral load copies were quantified by reverse transcription–polymerase chain reaction (PCR) using the AMPLICOR HIV-1 Monitor 1.5 (Roche, Indianapolis, Indiana). Viral load <400 copies/mL was considered undetectable. C-reactive protein (CRP) was quantified by PCR-Latex (Wiener Laboratory, Rosario, Argentina), which qualitatively detects levels above 6 mg/L as reactive. Our statistical models therefore included CRP as a dichotomous reactive/nonreactive variable.
Statistical Analysis
T tests and χ2 tests were used to compare means and proportions of sociodemographic, drug use, laboratory, and clinical characteristics by HCV status, stratified by HIV status. The analysis of variance F test was used to assess overall differences by both HIV and HCV status. The independent associations of HIV and HCV status with cholesterol levels were assessed using multivariate linear regression analysis. Separate models were run using each type of cholesterol (TC, HDL, and LDL) as the outcome. HIV/HCV status was entered in as 3 dummy variables: HIV monoinfection, HCV monoinfection, and HIV/HCV coinfection. The HIV/HCV-negative group was used as the reference. Covariates included gender, race, age, TG levels, body mass index (BMI), dietary intake, and alcohol use. Among HIV-infected participants, we examined the following variables as potential confounders: protease inhibitor (PI), nucleoside/nucleotide reverse transcriptase inhibitor (NRTI), and nonnucleoside reverse transcriptase inhibitor (NNRTI) use as well as CD4 count and HIV viral load. All analyses were performed using SAS v.9.1 (Cary, NC, USA).
Results
Table 1 shows the demographic, drug use, nutritional, and clinical characteristics of the 202 study participants stratified by HIV and HCV status. The majority of participants in all subgroups were white males. The HCV-positive participants were significantly older than those without HCV infection, regardless of the HIV status. Noninjection drug use was high across groups, although HIV/HCV-coinfected participants had the lowest percentage of current use of noninjection drugs. The HCV-infected participants had the highest percentage of injection drug use. Due to the study design, recruitment site differed significantly between the groups, whereby HIV-uninfected participants were more likely to be recruited from the drug rehabilitation center and HIV-infected participants were more likely to be recruited from the HIV clinic.
Demographic and Clinical Characteristics by HIV and HCV Status.a

Abbreviations: ANOVA, analysis of variance; BMI, body mass index; CENARESO, Centro Nacional de Reeducación Social; FUNDAI, Fundación de Ayuda al Inmunodeficiente; HCV, hepatitis C virus; HDL, high-density lipoprotein; LDL, low-density lipoprotein; PCR, polymerase chain reaction; SD, standard deviation; TC, total cholesterol.
aValues are presented as mean ± SD or n (%).
bFisher exact test used because 25% or more of cells had expected counts of less than 5.0.
cData for race, alcohol, cigarette smoking, and drug use missing for 1 participant.
dHazardous drinker as defined by the National Institute on Alcohol Abuse and Alcoholism (Hazardous alcohol use definition: 7 drinks per week or 3 drinks per occasion for women and 14 drinks per week or 4 drinks per occasion in men.).
eC-reactive protein was quantified by PCR-Latex (Wiener Laboratory, Rosario, Argentina), which detects levels above 6 mg/L as positive.
There was a significant difference in cholesterol intake, BMI, and cigarette smoking across groups, with healthy uninfected participants consuming the most cholesterol, having the highest BMI, and having the highest proportion of cigarette smokers. Measurements of serum cholesterol levels also demonstrated that uninfected participants had the highest TC and LDL levels (P < .001 for both). There was no difference in fat intake or serum TGs between or across groups.
HIV-infected participants demonstrated significantly lower BMI and HDL levels compared to HIV-uninfected persons, irrespective of HCV status. Similarly, a higher proportion of HIV-infected versus HIV-uninfected participants demonstrated CRP reactivity. There were no statistically significant differences in TGs between or across groups.
Table 2 shows differences in HIV-related variables by HCV status. Nearly half (47%) of the coinfected patients were on HAART compared to only 14% of those infected with HIV alone (P = .01). When compared to HCV-negative patients, the coinfected patients demonstrated lower viral loads (71 417 ± 140 351 versus 327 527 ± 284 442, P = .001) and increased viral load suppression (29% versus 0%, P = .007). There were no significant differences in CD4 counts by HCV status. There was no statistical difference in the number of participants receiving each type of HAART regimen.
Clinical Characteristics for HIV-Positive Participants.a

Abbreviations: HAART, highly active antiretroviral therapy; HCV, hepatitis C virus.
aValues are presented as mean ± SD or n (%).
bData of HAART missing for 1 participant. Data of CD4 and viral load missing for 3 participants.
cFisher exact test used because 25% or more of cells had expected counts of less than 5.0.
Table 3 shows the final multivariate model examining the association of HIV and/or HCV with cholesterol levels. Cholesterol intake and cigarette smoking were not significantly associated with HIV and/or HCV status after controlling for other covariates and therefore were dropped from the final multivariate model. HIV/HCV-coinfected patients had the lowest TC levels (−28.7 mg/dL, P < .001), whereas HCV-positive and HIV-positive patients also had significantly lower TC levels (−22.4 mg/dL, P < .001 and −20.6, P = .002, respectively) compared to the noninfected reference group. Hepatitis C virus and HIV/HCV coinfection were significantly associated with lower LDL levels (−21.4 mg/dL, P = .001 and −20.3 mg/dL, P < .0001, respectively), whereas HIV infection alone showed only a trend toward lower LDL levels compared to the HIV/HCV-uninfected group. HIV and HIV/HCV coinfection, but not HCV infection alone, were associated with significantly lower HDL cholesterol levels (−9.1 mg/dL, P = .0008 and −6.8 mg/dL, P = .0006, respectively).
Factors Associated with TC, LDL, and HDL Cholesterol Levels (Final Multivariate Models).

Abbreviations: BMI, body mass index; CI, confidence interval; HCV, hepatitis C virus; HDL, high-density lipoprotein; LDL, low-density lipoprotein; TC, total cholesterol.
Body mass index, TG, and glucose levels were positively associated with TC and LDL levels. Triglycerides were negatively associated with HDL levels. Hazardous drinking was negatively associated with LDL levels. Female sex, amerindios ethnicity, and CRP nonreactivity were all associated with higher HDL levels.
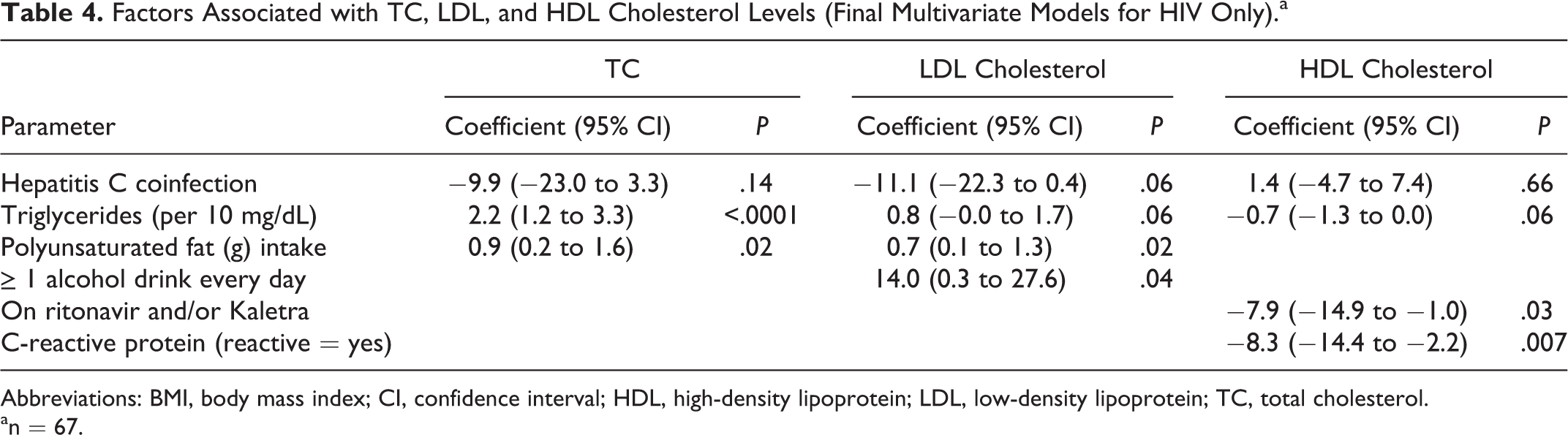
In a subgroup analysis of factors associated with cholesterol levels among HIV-infected participants (n = 67; Table 4), daily alcohol intake was associated with increased LDL cholesterol. Participants on ritonavir (RTV) and/or Kaletra (AbbVie Inc, North Chicago, IL, USA; n = 10), adjusted for the effects of hepatitis C, had significantly lower HDL levels (−7.9 mg/dL, P = .03). Ritonavir/Kaletra was not associated with TC or LDL levels.
Factors Associated with TC, LDL, and HDL Cholesterol Levels (Final Multivariate Models for HIV Only).a
Abbreviations: BMI, body mass index; CI, confidence interval; HDL, high-density lipoprotein; LDL, low-density lipoprotein; TC, total cholesterol.
an = 67.
Discussion
This study is one of the first to examine cholesterol levels in HIV- and/or HCV-infected drug users living in Argentina. Specifically, we compared cholesterol levels among HIV-monoinfected, HCV-monoinfected, and HIV/HCV-coinfected persons to a control group of uninfected persons with a similar ethnic background, diet, and drug use history. Despite similar total caloric and fat intake among the groups, HIV/HCV-uninfected participants had the highest BMI, TC, and LDL levels, which may be a marker of better overall health. The HCV-infected persons were older than HCV-negative persons in this cohort, which could be a result of lower incidence of injection drug use and successful needle distribution and exchange programs which began in Argentina in 1999 to 2000. 15,20 HIV-monoinfected persons had the lowest HDL cholesterol, which supports observations early in the HIV epidemic in the United States prior to the widespread use of HAART. 2,18 Only 14% of the HIV-monoinfected persons were receiving HAART, so the low HDL observed in this group is most likely attributed to direct effects of HIV infection. The low HDL associated with HIV infection was also seen in persons coinfected with HIV/HCV.
HIV/HCV-coinfected persons had the lowest TC, despite almost half of this group receiving HAART. This observation lends further support to prior studies which have demonstrated less dyslipidemia upon initiation of HAART in HIV/HCV-coinfected persons. 11,12 In addition, HCV monoinfection and HIV/HCV coinfection were associated with LDL levels approximately 20 mg/dL lower than the uninfected persons and approximately 10 mg/dL lower than the HIV-monoinfected persons. This observed lower LDL is clinically meaningful and supports the findings of prior observational studies in the United States. 9,11 Further studies are needed to examine whether the lower TC and LDL in HIV/HCV-coinfected persons confers a reduction in cardiovascular risk. Increased cardiovascular risk in HIV-infected persons has been well described in developed countries, and more recent studies have confirmed this risk in Latin American countries. 16,21,22 In a cohort of >4000 HIV-infected persons receiving HAART in Latin America, Cahn et al 22 reported an increased prevalence of dyslipidemia and metabolic syndrome and an intermediate 10-year risk of cardiovascular disease. Further, the low HDL and increased CRP positivity observed among our HIV-infected study participants suggest increased cardiovascular risk in this population.
There are several findings worthy of emphasis. Only approximately one-third of the HIV-infected population was on HAART, despite free access to antiretroviral therapy by the National AIDS Program of Argentina since 1996. 23 This observation highlights the need to engage drug users in HIV care. Zala et al 24 also reported limited use of HAART in Argentina and, in particular, noted that initiation of HAART was associated with older age, AIDS-defining illness, lower CD4 count, and higher viral load. Drug shortages and insufficient monitoring of response to HAART have also been reported. 25 In contrast, more recent data from the EuroSIDA cohort, a prospective study of HIV-infected persons in Europe, Israel, and Argentina, reported that, in Argentina, over 95% of the HIV-infected persons with a CD4 count <350 cells/mm3 were receiving HAART. However, this large cohort study includes only 1 clinical site in Argentina; a more detailed study evaluating HAART uptake and response to treatment at several sites throughout Argentina is warranted.
Interestingly, almost half of the coinfected persons were on HAART versus only 14% of the HIV-monoinfected persons. This finding is in sharp contrast to studies conducted early in the HAART era in the United States where HIV/HCV-coinfected persons were less likely than HIV-monoinfected persons to be prescribed HAART. 5,11 Further, 29% of the HCV/HIV-infected persons had a HIV viral load <1000 copies/mL versus none of the HIV-monoinfected persons. One possible explanation for our observation is that the coinfected patients were older and may have had more symptoms or a more advanced stage of HIV disease, thereby prompting initiation of HAART.
Some study limitations should be noted. We used HCV antibody, rather than HCV RNA, to identify persons infected with HCV. A small percentage of HIV-infected persons coinfected with HCV may be HCV antibody negative but have detectable HCV RNA. 5 Similarly, some persons may have had detectable HCV antibody but negative HCV RNA and thus cleared HCV infection. The cross-sectional design and low percentage of participants on HAART preclude us from assessing causality and the effects of HAART on serum lipids.
In summary, this work provides much needed data on cholesterol profile in HIV- and/or HCV-infected Argentinian drug users. Our findings suggest that HIV-infected Argentinean drug users will benefit from interventions aimed to improve engagement in medical care, including access to and monitoring of HAART. As HAART use becomes more widespread in Argentina and the HIV-infected population ages, further study is needed to examine the effect of antiretroviral therapy on cardiovascular disease.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded in part by NIH grants P30DA013868 and P30AI042853.