
Abstract
In Asian concentrated HIV epidemics, data on coinfection of sexually transmitted infections (STIs) among HIV-positive individuals are limited. The authors measured the prevalence of Chlamydia trachomatis (CT), Neisseria gonorrhea (NG), and syphilis, and their correlates among 319 HIV-positive individuals in Kathmandu, Nepal. The authors tested blood samples for syphilis and urine samples for CT and NG. Overall, 17 (5.3%) participants had at least 1 STI (CT: 1.3%, NG: 2.8%, and syphilis: 1.2%). Of 226 participants who had sex in past 6 months, 51.3% did not always use condoms. Older (aged 35-60 years) participants were more likely (adjusted odds ratio [AOR] = 3.83; 95% confidence interval [CI] = 1.19-12.33; P = .024) and those who were currently married (AOR = 0.30; 95% CI = 0.09-0.97; P = .046) or on antiretroviral therapy (AOR = 0.21; 95% CI = 0.06-0.71; P = .012) were less likely to have at least 1 STI. Our results suggest the need to strengthen the efforts to screen and treat STIs and to promote safer sexual practices among Nepalese HIV-positive individuals.
Introduction
Coinfection of sexually transmitted infections (STIs) in HIV-positive individuals can compromise their health in various ways. First, the presence of STIs in HIV-positive individuals can decrease the CD4 count and increase the concentrations of HIV viral load in blood plasma 1,2 and genital secretions, 2 -4 which might compromise the effectiveness of antiretroviral therapy (ART). Second, the presence of STIs can increase susceptibility to HIV superinfection or reinfection by disturbing mucosal barriers or by increasing the presence of susceptible immune cells in the genital tract. 5,6 Finally, the presence of syphilis may deteriorate the overall health status of patients as it is more difficult to treat the immune compromised HIV-positive individuals. 7,8
Past studies have reported coinfections of multiple STIs in HIV-positive individuals. For example, a review paper based on the results of 37 clinical and epidemiological studies on STIs among HIV-positive individuals reported a 16.3% overall mean point prevalence of confirmed STIs. 9 The median prevalence of the most common STIs studied was 9.5% for syphilis, 9.5% for gonorrhea, 5% for chlamydia, and 18.8% for trichomoniasis. The review reported the highest mean point prevalence of STIs in Asia (17.4%) using the results of 4 studies (1 each from Australia, 10 China, 11 Republic of Korea, 12 and Thailand 13 ) included in the review; all or most of the participants of these studies were HIV-positive men who have sex with men (MSM).
South and Southeast Asia are the regions where the largest number of HIV-positive individuals reside after sub-Saharan Africa. 14 It is suggested that HIV-positive individuals, particularly of South Asia, become infected with HIV most commonly through risky sexual behaviors. 15 Studies have revealed that a certain proportion of HIV-positive individuals in the region continue to engage in risky sexual behaviors even after learning about their HIV-positive status, 16 thus increasing their exposure to other strains of HIV as well as other STIs. However, little is known about STI coinfection among HIV-positive individuals who are aware of their HIV-positive status in South Asia.
In Nepal, a resource-limited country in South Asia, HIV prevalence among adults aged 15 to 49 years was 0.30% in 2011. 17 However, reported rates were much higher among injecting drug users (6.3%), female sex workers (4.2%), MSM (3.8%), and male labor migrants (1.8%), 18 in particular, labor migrants who seek work in Mumbai, India. 19 As of 2011, approximately 50 200 individuals in Nepal were living with HIV, and 4 of every 5 infections are believed to have been transmitted through sexual activity. 17 Evidence suggests that risky sexual behaviors are common among Nepalese HIV-positive individuals after receiving an HIV-positive diagnosis 16 and that several HIV-positive individuals had negative perceptions toward condom use, particularly in sero-concordant relationships. 20 However, no studies have been conducted to assess the prevalence of various STIs among HIV-positive individuals who are aware of their HIV-positive status in Nepal.
We, therefore, aimed to assess the prevalence of coinfection of STIs (chlamydia, gonorrhea, and syphilis) and their association with sociodemographic and health status, substance use, and sexual risk behaviors among HIV-positive individuals in the Kathmandu Valley, Nepal. We anticipate that the results of our study would be useful in improving STI screening and treatment services and in designing specific HIV prevention programs that help to protect the health of HIV-positive individuals and to prevent new HIV infections.
Methods
Study Site and Design
This study was conducted in the Kathmandu Valley, Nepal, from February to March 2010 as the baseline survey of a longitudinal healthy living study entitled “Positive Living with HIV” among HIV-positive individuals. 21 -27 The participants were recruited through 5 nongovernmental organizations (NGOs), Shakti Milan Samaj, Sneha Samaj, SPARSHA Nepal, Srijansil Mahila Samuha, and Youth Vision, all of which work with HIV-positive individuals in the study area. These NGOs were active in the Kathmandu Valley and contributed to the recruitment of HIV-positive individuals, both with and without ART, using their networks. HIV-positive women were the major target group of Shakti Milan Samaj, Sneha Samaj, and Srijansil Mahila Samuha, while HIV-positive men, in particular individuals who had used drugs, were the major target group of SPARSHA Nepal and Youth Vision. Main HIV/AIDS-related activities of these NGOs included organizing (1) monthly support group meetings of their members, including clients and HIV-positive staff members, (2) weekly HIV clinics, (3) in-house crisis management services, (4) community and home-based care services, and (5) support for hospital visits for consultation, laboratory investigation, ART initiation, and other services. The responsible NGO staff members also collect antiretroviral medications from designated ART sites and deliver them to specific clients as needed. SPARSHA Nepal also provides HIV counseling and testing services and prescribes ART.
For the purpose of this study, staff members of these NGOs contacted approximately 360 HIV-positive individuals either in person during their service visit or through phone calls 1 week prior to the survey date and provided the information about the study. In total, 330 people visited the study recruitment sites. Of these, 2 people refused to participate, 3 people could not stay for the interview and sample collection because of their work schedule, and 3 people did not provide the evidence of their HIV-positive diagnosis. Thus, a total of 322 HIV-positive individuals participated in the study. All participants were aged between 18 and 60 years, self-reported their diagnosis of HIV prior to the interview date, and provided written informed consent to participate in the study. The procedures of the study were reviewed and approved by the ethical committees of the Nepal Health Research Council, the National Center for Global Health and Medicine, Tokyo, and the Waseda University, Tokyo, Japan. The procedures of the study were also approved by the institutional review board of the University of Massachusetts Amherst, Massachusetts.
Data Collection Procedures
Prior to data collection, research assistants informed each of the participants individually about the study procedures using a prepared information sheet and also answered any questions. Before being interviewed, the participants signed a written informed consent form. To safeguard confidentiality, the participants were reassured that numerical codes would be used on the questionnaire, vials of blood and urine samples, and other forms containing the results of the interview or blood and urine tests instead of their names or other identifying information.
We collected data from 3 sources. First, trained interviewers conducted a face-to-face interview with each participant using a pretested Nepali version of a structured questionnaire. Measures included sociodemographic and health characteristics, substance use, and sexual risk and protective behaviors. Items of these measures were developed based on previous studies conducted in Nepal. 16,28,29 Second, laboratory technicians collected approximately 10 mL of venous blood using an evacuated tube, which was centrifuged immediately for 15 minutes to separate the serum. Finally, participants provided a first-void urine specimen for the examination of Chlamydia trachomatis (CT) and Neisseria gonorrhoeae (NG).
Participants were asked if they had had sexual intercourse in the past 6 months and, if so, whether they had used condoms. We asked about their behaviors separately with regular partners, casual partners (defined as any sexual encounter with a partner other than the primary partner), and commercial partners (defined as a partner, with whom the participant had sexual intercourse in exchange for money or gifts). Condom use was measured using the item, “In the past 6 months, how frequently did you use condoms when you had sex?” with the following choices: (1) “never,” (2) “sometimes,” (3) “most of the time,” and (4) “always.” Similar to a previous study, 16 unsafe sex was defined as not always having used condoms while having vaginal sex with regular, casual, or commercial partners in the past 6 months. We did not collect specific information about anal intercourse as none of the collaborating NGOs provided services specifically for HIV-positive MSM.
Laboratory Methods
Serum samples were tested for syphilis using the rapid plasma reagin (RPR; Omega Diagnostics, United Kingdom) as a screening test. All RPR reactive samples were, then, confirmed using a Treponema pallidum hemagglutination assay (TPHA; Omega Diagnostics, UK). Syphilis-positive individuals were defined as those who were positive for both RPR and TPHA. Active syphilis-positive individuals were defined as those who were positive for both RPR titre ≥1:8 and TPHA. For the detection of herpes simplexvirus (HSV)-2 immunoglobulin (IgG) antibodies, serum samples were tested using HSV-2 IgG enzyme-linked immunoassay (HerpesSelect 2 ELISA IgG; Focus Technologies, Cypress, CA, USA). 30 First-void urine was collected from the participants for the detection of CT and NG by polymerase chain reaction (PCR) using multiplex-PCR kit for sexually transmitted disease Chlamydia trachomatis (CTR)/Ureaplasma urealyticum (UU)/NG (Cosmo-Bio, Japan), according to manufacturer’s instructions. All participants, who had syphilis, gonorrhea, or chlamydia, received free treatment. Participants, who tested positive for HSV-2 and were symptomatic, received free acyclovir treatment from local health institutions.
Data Analyses
Of the 322 study participants, 3 were excluded from the analysis as they did not provide blood and urine samples resulting in a final study sample of 319 (183 men and 136 women) HIV-positive individuals. For analysis, first, we assessed the differences in sociodemographic, health, alcohol, drug, and sexual behavior–related variables by sex using chi-square tests, independent t tests, Fisher exact tests, or Wilcoxon rank sum test, as appropriate. Second, we reported the prevalence of STIs among all participants as well as by gender. Finally, we explored the factors associated with at least 1 curable STI (chlamydia, gonorrhea, or active syphilis) using bivariate and multivariable logistic regression analyses to estimate odds ratios (ORs) with 95% confidence intervals (CIs). For this, we first examined the bivariate associations between each independent variable and having at least 1 of the curable STIs. As Katz 31 suggested, we then performed multivariable logistic regression analysis including all variables that had a bivariate P value less than or equal to .25 or the variables considered important a priori regardless of bivariate P value, such as consistent condom use. Our final multivariable model adjusted for age, current marital status, education, employment, months since testing HIV positive, ART status, and consistent condom use. In our final model, we did not adjust “number of sexual partners in the past 6 months” and “type of partner” due to multicollinearity with “consistent condom use;” the variance inflation factor of these variables was over 2.0. Finally, we examined the bivariate association between age and having at least 1 STI stratified by ART status of the participants. We used SPSS version 15.0 (SPSS Inc, Chicago, IL, USA) to perform all of the analyses with statistical significance set at P < .05.
Results
Demographic and Health Characteristics
Table 1 shows the characteristics of HIV-positive participants by gender. Compared to women, men were significantly older (mean age: 32.6 years versus 35.6 years; P < .001) and were more likely to have above primary-level education and office employment. A significantly higher proportion of women were on ART than men. Similarly, a significantly higher proportion of older participants (>34 years) were on ART compared with younger participants (20-34 years; 83.2% versus 65.5%; P < .001). A total of 2 participants reported their sexual orientation as “bisexual,” and all others were “heterosexual.”
Characteristics of HIV-Positive Participants of the Positive Living with HIV (POLH) Study.a

Abbreviations: ART, antiretroviral therapy; ARV, antiretroviral.
aN = 319.
b P values were based on the chi-square test (or Fisher exact test) for categorical variables and independent t test (or Wilcoxon rank-sum test) for continuous variables.
cTwo participants (1 male and 1 female) did not respond to this question.
dParticipants are those who were on ART.
eParticipants are those who had sex in past 6 months.
Alcohol and Drug Use and Sexual Behaviors
Forty (12.5%) of the 319 participants (16.9% men and 6.6% women) reported having drunk alcohol during the past month (Table 1). A much higher proportion of men (68.3%) reported a lifetime history of injecting drug use compared with women (3.7%).
Regarding sexual behaviors, a total of 154 (84.2%) male and 72 (52.9%) female participants disclosed having had sex in the past 6 months. Of those, 68.8% of male and 94.4% of female participants had sex only with their regular partners.
A total of 23.0% of participants (31.2% males and 5.6% females), who had sex in past 6 months, reported multiple sexual partners. In total, 19.8% of the participants receiving ART reported having had sex with multiple sexual partners compared to 31.3% not receiving ART (P = .064). A lower proportion of married participants reported having had sex with multiple sexual partners in past 6 months compared to single participants (14.5% versus 62.5%; P < .001). Similarly, a lower proportion of unemployed participants reported having had sex with multiple partners in the past 6 months compared to those who were employed (14.5% versus 26.2%), although the difference was not statistically significant (P = .062).
Of the 226 participants who had had sex in past 6 months, 51.3% did not use condoms consistently with their sexual partners. A higher proportion of female participants failed to use condom consistently compared with male participants (63.9% versus 45.5%; P = .010)
Coinfection of STIs
The prevalence of chlamydia, gonorrhea, and syphilis (positive for both RPR and TPHA) among the participants was 1.3% (male: 0.5% and female: 2.2%), 2.8% (male: 3.8% and female: 1.5%), and 4.1% (male: 4.4% and female: 3.7%), respectively (Table 2). The prevalence of active syphilis (RPR titer ≥1:8 and TPHA positive) was 1.2% among participants (male: 1.6% and female: 0.7%). Overall, a total of 17 (5.3%) participants (male: 6.0% and female: 4.4%) had at least 1 of the curable STIs (chlamydia, gonorrhea, or active syphilis).
Prevalence of Sexually Transmitted Infections among HIV-Positive Participants of the Positive Living with HIV (POLH) Study by Sex.

Abbreviations: RPR, rapid plasma regain; STI, sexually transmitted infection; TPHA, Treponema pallidum hemagglutination assay.
aA total of 317 participants (182 male and 135 female) were tested for gonorrhea and chlamydia.
bSyphilis-positive cases are those who were positive for both RPR and TPHA.
cTwo of these cases tested TPHA negative.
dActive syphilis-positive cases are those who were positive for both RPR titer ≥1:8 and TPHA.
Factors Associated with Curable STIs
Factors that were associated with having at least 1 STI in the bivariate and multivariable analyses are shown in Table 3. In the multivariable analysis, older (aged 35-60 years) participants were more likely to have at least 1 STI compared to younger (aged 20-34 years) participants. Currently married participants were less likely to have at least 1 STI compared to single participants. Similarly, participants who were on ART were less likely to have at least 1 STI compared to those who were not receiving such treatment. The participants who had a job were more likely to have at least 1 STI than those who did not have any job; although the difference was not statistically significant, the adjusted OR increased (AOR = 3.10; 95% CI = 0.75-12.76). In the multivariable analysis, the association between educational level, months since testing HIV positive, and consistent condom use in past 6 months and having at least 1 curable STI was not statistically significant.
Factors Associated with Curable Sexually Transmitted Infections among HIV-Positive Participants of the Positive Living with HIV (POLH) Study.a

Abbreviations: AOR, adjusted odds ratio; ART, antiretroviral therapy; CI, confidence interval; HSV, herpes simplex virus; IgG, immunoglobulin; OR, odds ratio; RPR, rapid plasma regain; STI, sexually transmitted infection; TPHA, Treponema pallidum hemagglutination assay.
aN = 319.
bAt least 1 of the chlamydia, gonorrhea, or active syphilis (positive for both RPR titer ≥1:8 and TPHA) positive cases.
cA total of 317 participants were included in the multivariable logistic regression analysis. “Number of sexual partners in past 6 months” and “type of partner” were not included in multivariable analysis because of multicollinearity with “consistent condom use.”
dTwo participants did not respond to this question.
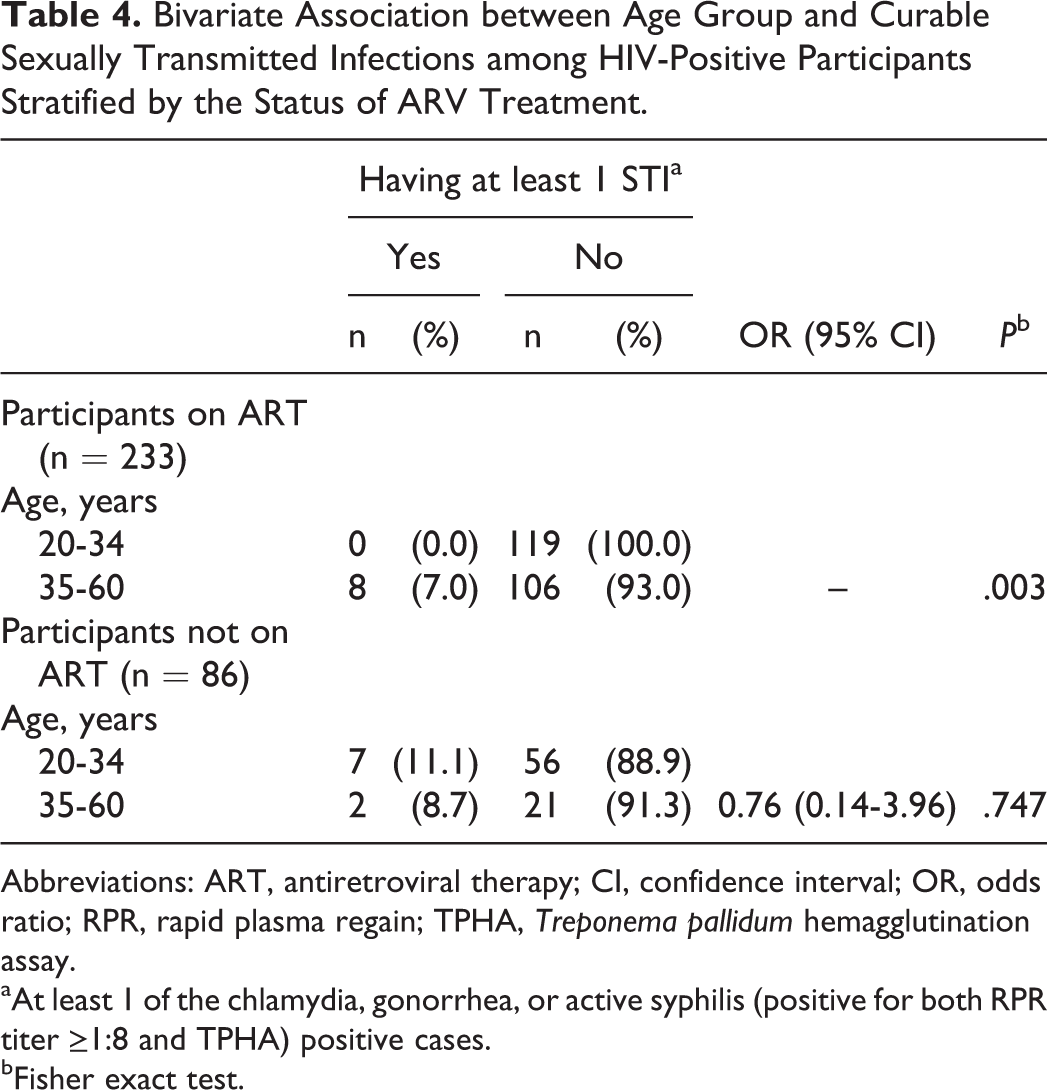
In the stratified analysis, the bivariate association between age group of the participants and diagnosis of at least 1 STI was statistically significant among participants receiving ART, in that all the participants having at least 1 STI were in the older (35-60 years) age group (Table 4).
Bivariate Association between Age Group and Curable Sexually Transmitted Infections among HIV-Positive Participants Stratified by the Status of ARV Treatment.
Abbreviations: ART, antiretroviral therapy; CI, confidence interval; OR, odds ratio; RPR, rapid plasma regain; TPHA, Treponema pallidum hemagglutination assay.
aAt least 1 of the chlamydia, gonorrhea, or active syphilis (positive for both RPR titer ≥1:8 and TPHA) positive cases.
bFisher exact test.
Discussion
Our findings revealed that 5.3% of the HIV-positive individuals in our study had at least 1 of the 3 curable STIs, chlamydia, gonorrhea, or active syphilis. Our results indicate that approximately three-fourths of our participants (71.0%) were sexually active in the past 6 months and over half of them did not always use condoms during sexual intercourse. Our results suggest that the sexual partners of our participants are at high risk for HIV/STI infection. Likewise, our participants who are practicing unprotected sexual intercourse are at increased risk of HIV superinfection or infection with other STIs.
Although some studies in Europe 32 and the United States 33,34 have reported low rates of STIs among HIV-positive individuals, the rates of STIs among our participants are comparable to the results from several other studies. For example, the rate of gonorrhea was 1.3% among men and 1.4% among women in a study in Thailand, whereas the rate of chlamydia was 0.8% among men and 0.9% among women. 35 The rate of chlamydia was higher (6.6%) among female participants in another study in Thailand, but the rate of gonorrhea (1.0%) was lower 36 than the corresponding rates among female participants in our study. The STI rates were much higher in other studies conducted in Australia, 10 China, 11 Republic of Korea, 12 and Thailand 13 than those reported in our study. However, this discrepancy can be explained by the differences in target populations. For example, all or most of the participants in those studies were HIV-positive MSM, a population at high risk for STIs, while the participants in our study comprised the general HIV-infected population. We did not aim to exclude HIV-positive MSM individuals from our study. Rather, as none of our collaborating NGOs provided services specifically for this population, they were undersampled.
Our results on STI coinfection have important implications for STI screening among HIV-positive individuals. As our participants demonstrated a relatively low prevalence of chlamydia and gonorrhea, universal screening for these infections among HIV-positive individuals using sensitive tests may not be practical in resource-poor settings. Screening of such infections among populations reporting high-risk behaviors along with the periodic monitoring of STIs might be more useful. In contrast, strategies to screen all HIV-positive individuals for syphilis would be useful as syphilis screening is relatively inexpensive, the tests are easy to perform at local laboratories, and the disease may cause serious complications when left untreated.
Participants receiving ART were less likely to have one of the curable STIs compared with those not receiving ART. A lower proportion of our participants, who were on ART, reported having sex with multiple sexual partners than those who were not on ART, though the difference was not statistically significant. It is possible that the participants on ART contacted health care providers more frequently, particularly during their visit to refill medicines, and that counseling of participants during such sessions may have resulted in the reduced risk of STI infection.
Contrary to previous studies, our findings revealed that older participants (aged 35-60 years) had a 4 times greater likelihood of having one of the curable STIs than those of younger participants (aged 20-34 years). In a study carried out in Malawi, Tanzania, and Zambia, younger HIV-positive women had a higher prevalence of chlamydia and gonorrhea than those of older participants. 37 In Thailand, 2 studies reported no statistically significant association between age and STI prevalence among HIV-positive individuals. 35,36 Interestingly, a significantly higher proportion of our older participants were on ART compared with younger participants.
In the stratified analysis by ART status, older participants (aged 35-60 years) receiving ART had a greater likelihood of having one of the curable STIs than those of younger participants (aged 20-34 years). This result is contrary to our expectation. Although further studies are needed to explore the reasons for the high rates of curable STIs among older participants on ART, our findings suggest that health care providers should seriously consider providing STI screening for this group. In resource-poor settings, such as Nepal, testing may have to be limited only to the most serious STIs, such as syphilis. In addition, efforts should be made to broadly disseminate health promotion messages that promote safe sexual practices.
Compared to currently unmarried participants, married participants were less likely to have any of the curable STIs. Sexual exclusivity norms are stronger in marriage than for other types of relationships in Nepal. Similar to previous findings, 16 married participants in our study were less likely to report multiple sexual partners in the past 6 months than were single participants. We also assume that married individuals in our study area would adhere to better health care practices following an STI diagnosis than unmarried individuals in order to prevent infecting their spouses.
Employed participants tended to have one of the STIs compared with those who were unemployed. Although the association was not statistically significant, the OR increases after adjusting other potential confounding variables. A previous study from Nepal revealed that income allows men to interact with and have sex with local women, increasing their vulnerability to STIs. 38 In our study, a higher proportion of employed participants reported having sex with multiple partners in the last 6 months than did unemployed participants. Such high-risk behaviors might have accounted for the increased prevalence of STIs among the employed participants.
To our knowledge, this is the first study to report the coinfection prevalence of concurrent, active STIs among an HIV-positive population in Nepal. Noted strengths of our study are the use of sensitive tests to diagnose STIs as well as the inclusion of both genders, those receiving ART and those not receiving ART, the latter being a hard-to-reach HIV-positive population in regular service settings.
This study has some limitations. First, the participants in this study might not be representative of all HIV-positive individuals in the Kathmandu Valley as they were recruited through an outreach network consisting of multiple NGOs. In particular, only 2 bisexual participants were included in our study and MSM, a group at high risk for HIV infection in Nepal, 18 were not identified by the recruiting NGOs. Second, it is possible that during administration of the questionnaire, participants might have responded with what they perceived to be socially desirable answers. However, our methodology to reassure the confidentiality of participants’ information might have minimized such bias as reported in a previous study. 39 Finally, our study placed little emphasis on symptomatic infection that could be an important factor for screening and syndromic management of STIs. In Nepal, etiological diagnosis of syphilis is recommended whenever syphilis testing is available, while syndromic management of STIs in settings without laboratory facilities is a standard procedure. 40 The latest national HIV/AIDS strategy (2011-2016) 41 envisioned providing standardized and quality etiological diagnosis for common STIs, including syphilis and gonorrhea at HIV testing and counselling centers as well as where laboratory services are available. Therefore, a syndromic approach may not be the best option for the management of STIs among HIV-positive individuals residing in the Kathmandu Valley where laboratory testing facilities are available. One issue of concern with the syndromic management of STIs is that HIV-positive individuals may not exhibit signs or symptoms of STIs, including chlamydia, gonorrhea, and syphilis. 36,42,43 Moreover, HIV-positive individuals with STI signs or symptoms may be free from STIs as several signs or symptoms are not specific to STIs. 36
Conclusion
In conclusion, the prevalence of concurrent STIs as well as risky sexual behaviors among our participants suggests an urgent need for HIV prevention interventions for HIV-positive individuals and their sexual partners. Such interventions should provide education about the potential consequences of having unprotected sex among HIV-positive individuals and promote safer sexual practices. Moreover, routine STI screening should be conducted within clinical settings and, more importantly, STI screening strategies should be identified for those who are not receiving ART.
Footnotes
Acknowledgments
The authors extend their sincere thanks to all the study participants for their important information, time, and participation. The authors thank the interviewers, research assistants, and laboratory technicians for their efforts in conducting the fieldwork and processing the blood samples. The authors gratefully acknowledge 5 nongovernmental organizations: SPARSHA Nepal, Sneha Samaj, Srijansil Mahila Samuha, Shakti Milan Samaj, and Youth Vision Nepal for their invaluable support in recruiting the study participants and providing other support.
Authors’ Note
This study was presented in part at the Sixth Annual Consortium of Universities for Global Health Conference, Boston, Massachusetts, March 26-28, 2015; Abstract Number: 01CD014.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partly supported by a Grant for Research on Global Health and Medicine (21A-2) from the National Center for Global Health and Medicine, Japan and by a Grant-in-Aid for Young Scientists (B 22790581), Japan Society for the Promotion of Science, The Ministry of Education, Culture, Sports, Science and Technology, Japan. The funding agency had no role in the study design; in the collection, analysis and interpretation of data; in the writing of the report; and in the decision to submit the article for publication.