
Abstract
Background:
Chronic renal failure and HIV/AIDS are both prevalent in Nigeria. We performed a cross-sectional analysis of renal function in newly diagnosed, treatment-naive HIV-infected patients before initiating highly active antiretroviral therapy.
Methods:
Treatment-inexperienced individuals were recruited. Patients with diabetes mellitus and hypertension were excluded. Plasma creatinine level was used to measure the estimated glomerular filtration rate ([eGFR] by Modification of Diet in Renal Disease equation). Predictors of creatinine and eGFR were determined by univariate and multivariate analyses.
Results:
We evaluated 183 patients. In all, 44 (24%) patients had a GFR <60 mL/min/1.73 m2, implying moderate chronic kidney disease (CKD). Considering the eGFR, 22 (12%) patients had stage 1, 117 (63.9%) stage 2, 13 (7.1%) stage 3, 27 (14.8%) stage 4, and 4 (2.2%) stage 5 CKD. Creatinine inversely correlated with CD4 (r = −.228, P = .025). CD4 predicts creatinine (odds ratio 1.6, 95% confidence interval 1.0-1.8, P = .003).
Conclusion:
In ART-naive patients, CKD is common, and low eGFR was associated with lower CD4 counts.
Keywords
Introduction
Chronic kidney disease (CKD) is defined as kidney damage or reduced kidney function that persists for more than 3 months. 1 Renal function impairment that results from HIV infection is called HIV-associated nephropathy (HIVAN). Renal disease in HIV-infected individuals is associated with an increased morbidity and mortality. 2 People with advanced disease (associated with lower CD4 counts) are at greater risk of renal injury. Approximately 80% of patients with HIVAN have a CD4 count of less than 200. HIV-associated nephropathy presents with nephrotic syndrome and progressive renal failure.
Race has been stated as a risk factor for CKD. Black persons in the United States constitute only about 10% of the whole population but contribute >30% of patients with end-stage renal disease (ESRD) in the general population. 3 Young male blacks are also said to have a 11-fold risk of CKD compared to their white counterparts. 4 In blacks, 5 new cases of ESRD are reported in every 100 cases of CKD, while in white only 1 new ESRD case is reported in every 100 cases of CKD. 5
HIV-associated nephropathy has been said to be much more common in black and African American patients with HIV. However, further and wider studies among the Africans are still necessary. HIV-associated nephropathy is likely caused by direct viral uptake into certain cells of the kidney, with incorporation of the viral genome into the cellular DNA. Direct cellular injury by the virus is being recognized as the basis of HIVAN. 6 Cellular entry by HIV is not clearly understood. Interplay of molecular factors has been stated. Increased level of cellular death by apoptosis has also been observed in HIV-infected renal cells. 7 Continued presence and replication of HIV in the glomerular epithelial cells, despite undetectable viral load, points to the role of kidney as a reservoir of HIV. 8,9
Despite the fact that combination, antiretroviral therapy (ART) has significantly reduced the impact of kidney disease in HIV/AIDS in the United States, and HIV epidemic in sub-Saharan African populations still has indisputable enormous public health implications. Twenty-seven percent of 99 consecutive kidney biopsies in HIV-infected black South Africans were diagnosed with HIVAN. 10 Creatinine clearance <50 mL/min was found in 43% of 195 highly active antiretroviral therapy (HAART)-naive Ugandans, while 21% had dipstick proteinuria. 11 Median creatinine clearance in 90 HAART-naive Nigerians was found to be <60 mL/min. 12 Moreover, as much as 13% of 740 HAART-naive Rwandan women (with a CD4 count <200) had proteinuria. 13 Data from ART trial in Uganda and Zimbabwe showed improvement in kidney function after HAART is commenced. 14
Studies that suggested improvement in renal function due to ART used the Cockcroft-Gault equation to measure the estimated glomerular filtration rate (eGFR). This raises the possibility that malnutrition and low body weight may have biased the estimates. However, Modification of Diet in Renal Disease (MDRD) equation used in this study has been stated to be superior to Cockcroft-Gault equation in measuring eGFR.
The progression rate of CKD in HIV/AIDS and HIVAN in the post-HAART period has reduced tremendously. 15 It has been reported that there is a possibility of recovery of renal function after commencement of HAART in patients who were previously dependent on dialysis. 15 This HAART-related decrease in the rate of progression supports the potential therapeutic role of antiretroviral (ARV) drugs in treating kidney disease. The clinical course of HIVAN is associated with CD4 count and HIV RNA level. CD4 counts below 200 cells/mm3 have been associated with a faster time to doubling of creatinine excretion. 16
However, some HAART drugs have also been associated with renal function impairment in the course of treatment. This could be either inducing or worsening factor of decline in renal function. Diverse findings have been stated from various study populations. Baseline renal function status is thus an important factor in determining the effect of HAART drugs on renal function. Pretreatment renal function impairment informs the proper choice of HAART regimen for individual patients. Other stated factors besides the nadir CD4 count include advanced age and female sex. Inadequate or inappropriate screening of the renal function status prior to initiation of HAART may lead to wrong adduction of renal dysfunction that is subsequently discovered after initiating therapy to adverse effects of drugs. In this analysis, we sought to describe the prevalence and risk factors of CKD in treatment-naive HIV-infected persons prior to initiating HAART in our clinic system.
Methods
This cross-sectional study was carried out at the University of Ilorin Teaching hospital, Kwara state, a tertiary health institution providing tertiary health care services to close to 2 million people in the north central Nigeria. Sample size was calculated by applying the index prevalence of 3.1% of HIV/AIDS in Nigeria at the time of study. The Fisher formula was applied for determining the sample size when studying proportions with population of greater than 10 000. This research was approved by the institutional research ethics committee (institutional review board). Informed consent was sought and obtained from all the patients, and only those who satisfied the inclusion criteria were involved in the study. A total of 183 consecutive newly diagnosed ART-naive patients, with no previous history of HAART use, within the age of 18 to 59 years, and with confirmed HIV/AIDS attending the HIV/AIDS clinic were selected from clinics in family medicine, internal medicine, hematology, and microbiology departments for the study.
Fifty apparently healthy participants (test confirmed non-HIV-infected persons) were used as control. The exclusion criteria included newly diagnosed patients with HIV/AIDS having a history of comorbid diabetes mellitus (ie, diabetic nephropathy), underlying hypertension defined as systolic blood pressure >140 mm Hg or diastolic blood pressure >90 mm Hg, underlying liver cirrhosis, or background kidney disease (eg, glomerulonephritis). From each patient, 4 to 5 mL of blood were drawn and collected into lithium heparin tubes and spun at 3000 rpm for 5 minutes. Whenever the samples could not be analyzed the same day, the supernatant plasma was transferred to storage tubes and stored at −20°C.
Creatinine in plasma samples was determined by modified Jaffe kinetic method, with calibration traceable to isotope dilution mass spectrometry. Within run and interassay precision, studies were carried out consistently. The intra-assay, interassay, and day-to-day precision for creatinine were 0.4%, 1.6%, and 5%, respectively. The creatinine values were used to calculate creatinine clearance by eGFR by MDRD using the available online calculators.
Given the cross-sectional nature of our study, we could not specifically or adequately assess the time frames for the development and persistence of declined GFR of <60 mL/min/1.73 m2, except for prolonged duration of symptoms experienced by the patients before presentation for HIV testing and diagnosis, that is, late stage HIV diagnosis. Blood samples were collected only once for creatinine assays, with no further sample collection for repeat creatinine assays. Case definition of CKD was therefore based on 2 criteria. First, elevated plasma creatinine using the reference intervals of serum/plasma creatinine values for the classification of chronic progressive renal disease: reduced renal reserve (88.4-221 µmol/L), renal insufficiency (221-530.4 µmol/L), renal failure (486.2-972.4 µmol/L), and ESRD (>707.2 µmol/L). Second, because using eGFR is superior to the use of absolute plasma creatinine values in staging CKD, we further categorized the stages of CKD in the patients based on the eGFR values (by MDRD equation) as follows: stage 1 (≥90 mL/min/1.73 m2), stage 2 (60-89 mL/min/1.73 m2), stage 3 (30-59 mL/min/1.73 m2), stage 4 (15-29 mL/min/1.73 m2), and ESRD or stage 5 (≤15 mL/min/1.73 m2).
Statistical process control for Microsoft Excel software (SPCXC 2007) was used to determine the descriptive statistics for each variable analyzed. The mean pretreatment values of plasma creatinine and eGFR of the patients and the apparently healthy controls were compared using 2-tailed independent Student t test with SPSS-PC (SPSS Incorporated, Chicago, Illinois, USA). Linear regressions and multivariable sensitivity analyses were done to determine the possible predictors/factors associated with changes in plasma creatinine and eGFR-MDRD (baseline CD4, age, weight, basal metabolic index [BMI], and gender). Significance was set at P ≤ .05. Data were analyzed with the SPSS version 16 (SPSS Inc, Chicago, Illinois, USA).
Results
The mean age of the patients was 37.9 ± 10.9 (18-59 years), mean CD4 count was 149 ± 116 (7-347 cells/1000 mm3), systolic blood pressure was 90 to 140 mm Hg, while their diastolic pressure was 60 to 90 mm Hg. Their mean weight, height, and BMI values are shown in Table 1. In all, 105 (57.4%) patients were females, while 78 (42.6%) were males. There was a significant difference in age between male and female patients (P = .017), and younger age-groups were infected among females than males. No significant difference exists between male and female groups for weight, height, BMI, and CD4 (Table 2). The seronegative controls had a mean age of 27.7 ± 8.0 years (minimum 18, maximum 56), systolic blood pressure was 100 to 130 mm Hg with diastolic pressure of 60 to 90 mm Hg. Their mean weight, height, and BMI values are also shown in Table 1. The mean plasma creatinine level of the controls was 56.82 µmol/L (standard deviation 29.65). The mean plasma creatinine levels of the patients were 131.09 µmol/L (above the upper limit of the accepted reference values for plasma creatinine [53-106 µmol/L]) in our population.
Descriptive Statistics of Biodata and Biochemical Parameters of the Patients and Controls.

Abbreviations: BMI, basal metabolic index; eGFR, estimate glomerular filtration rate; SD, standard deviation.
Comparison of Biodata and Biochemical Variables between Male and Female Patients.
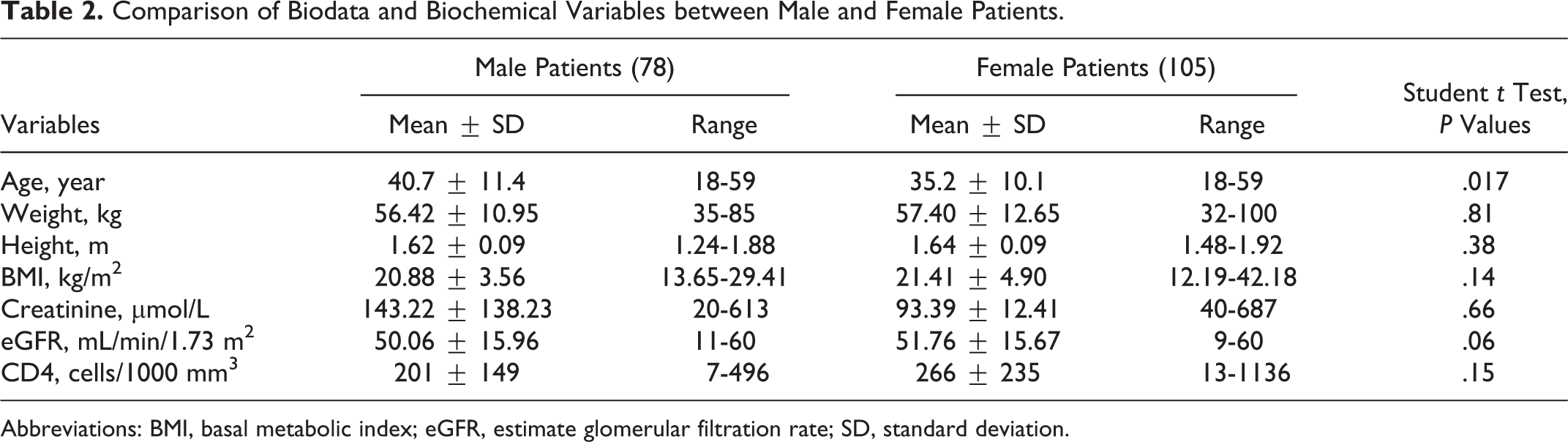
Abbreviations: BMI, basal metabolic index; eGFR, estimate glomerular filtration rate; SD, standard deviation.
In all, 56 (30.6%) patients had elevated creatinine levels of 0.3 mg/dL or 26.5 µmol/L above the upper reference limit of 106 µmol/L (ie, ≥ 132.5 µmol/L). Of these 56 patients (ie, 24% of 183), 44 had eGFR <60 mL/min/1.73 m2, thus meeting the criteria for stage 3 and lower CKD. With reference to the absolute plasma creatinine values, 29 (15.8%) patients had reduced renal reserve, 32 (17.5%) had renal insufficiency, 7 (3.8%) had renal failure, while 3 (1.6%) had ESRD/uremic syndrome. The remaining 112 (61.2%) patients had plasma creatinine values <88.4 µmol/L (ie, residual renal function >75%; Table 3). The reference intervals of serum/plasma creatinine values for this classification of chronic progressive renal disease are shown in Table 3. The patients had significantly higher mean plasma creatinine (131.09 ± 3.29 µmol/L) compared to the seronegative controls (56.82 ± 29.65 µmol/L), P = .006. Fifty-six (30.6%) of the patients had plasma creatinine 0.3 mg/dL or 26.5 µmol/L above the normal (ie, ≥132.5 µmol/L).
Distribution of the Patients into Stages of Chronic Progressive Renal Disease Based on Plasma Creatinine Values. 17,a

Abbreviation: ESRD, end-stage renal disease.
aThe remaining 112 (61.2% of 183) patients had plasma creatinine values <88.4 µmol/L.
bReference 18.
Also, the patients had a significantly lower mean eGFR compared to the controls (47.94 ± 15.83 mL/min/1.73 m2 vs ≥60 mL/min/1.73 m2; P = .000). In all, 44 (24% of 183) had eGFR <60 mL/min/1.73 m2, thus meeting the criteria for CKD. Thus, using eGFR, which is superior to absolute plasma creatinine values in staging CKD, the pattern of CKD in the patients was as follows: 22 (12%) had stage 1, 117 (63.9%) stage 2, 13 (7.1%) stage 3, 27 (14.8%) 4, and 4 (2.2%) ESRD (stage 5), Table 4.
Distribution of the Patients into CKD Stages based on eGFR Values Reference.

Abbreviations: CKD, Chronic kidney disease; eGFR, estimate glomerular filtration rate; MDRD, Modification of Diet in Renal Disease.
No significant difference in plasma creatinine and eGFR existed between male and female groups of patients (P = .6 and .07, respectively). Overall, there was a significant negative correlation between plasma creatinine and CD4 (r = −.228, P = .025). CD4 also significantly correlates inversely with plasma creatinine among males (r = −.408, P = .034), while age correlates negatively with creatinine among the females (r = −.2, P = .043). Significant negative correlation existed between eGFR and plasma creatinine (r = −.95, P < .001). There was no significant association between baseline plasma creatinine elevation and age, weight, height, and BMI. Univariate analysis showed baseline CD4 count was significantly associated with creatinine level (adjusted odds ratio 1.4, 95% confidence interval 1.0-1.8, P = .003). Patients with lower CD4 count had higher values of creatinine with lower eGFR. Using multivariable sensitivity analysis with stepwise selection (dependent variable: creatinine and independent variables: age, weight, height, BMI, and CD4 count), it was showed that adding age to the model first yielded an R 2 of .015. With addition of weight, the R 2 remained the same. Adding height increased the R 2 to .220, which was not significant (P = .293). Addition of BMI led to reduction in R 2, which was not significant (P = .565). Adding CD4 count resulted in an increase in R 2 to .042, which was not quite significant (P = .078). Thus, in the multivariate sensitivity analysis, there was no significant independent association between creatinine and age, weight, height, or BMI. Summary of the stepwise selection is shown in Supplemental Table 1. Using multivariate sensitivity analysis of probable factors affecting eGFR with stepwise selection (dependent variable: eGFR [MDRD] and independent variables: age, weight, height, BMI, and CD4 count), it was shown that adding age to the model first yielded an R 2 of .014, which remained the same when weight and height were added consecutively. Additions of BMI led to an increase in R 2 to .018 with nonsignificant P (.762). Finally, addition of CD4 count further increased R 2 to .027, which was also not significant (P = .209). Thus, in the multivariate sensitivity analysis, there was no significant independent association between eGFR (MDRD equation) and age, weight, height, BMI, or CD4 count. Summary of the stepwise selection is shown in Supplemental Table 2.
Discussion
Our study shows that HAART-naive people living with HIV/AIDS have significantly lower eGFR compared to healthy individuals. Renal function impairment manifests as reduced GFR with elevation in serum or plasma creatinine. Thus, in this population of ART-naive Nigerian patients with late-stage HIV diagnosis (ie, median CD4 count below 200), there was a high prevalence of abnormal renal function. We observed elevated creatinine concentrations in slightly less than one-third of this cohort of ART-naive patients, which demonstrated that they were already in the different stages of chronic progressive kidney disease (reduced renal reserve or stage 1 renal disease through to ESRD). This corroborates the findings of most other cohort studies that show CKD with elevated creatinine. 1,2,19 –21
Declined eGFR in the range of stages 3 to 5 CKD observed in a significant proportion of our participants (slightly less than one-quarter) shows that CKD is highly prevalent in this population of Nigerian patients with late stage HIV diagnosis. The findings provide evidence that HIV/AIDS as a disease state is associated with renal impairment independent of the possible nephrotoxic effects of ARV agents or other drugs used in the treatment of opportunistic infections in persons living with HIV. This finding is consistent with previous reports in the HIV/AIDS literature, and it confirms HIV as an established cause of damage to the kidney. 6,8,9,22 The basis of HIV-induced renal damage has been recognized as direct cellular injury by the virus or by changes in the release of cytokines during HIV infection. 23 –27
The mean CD4 count of the patients in this study is consistent with the finding that HIVAN usually occurs only in advanced disease and mostly in patients with a CD4 count of less than 200. 26,27 The finding of this renal impairment from HIV infection in these sub-Saharan African natives is also consistent with the fact that HIVAN is much more common in black and African American patients with HIV. 27 Our findings are also similar to those of Southern African indigenes and black adults in the United States where it is found to be the third most common cause of ESRD. 27 However, no renal biopsies were performed on the patients in our study.
Although renal function impairment is a frequent complication of HIV/AIDS, much is yet to be done/reported about its prevalence among diverse populations in Africa. Our finding of a CKD prevalence of 30.6% (abnormal/elevated serum creatinine) and 24% (reduced eGFR, <60 mL/min/1.73 m2) among patients 28 with HIV/AIDS in a Nigerian tertiary health institution providing tertiary health care services to close to 2 million people in the north central Nigeria is akin to the finding of 38% by Enem et al 19 in a study to determine the prevalence, clinical features, and risk factors for renal disease in HIV-positive Nigerians, which was carried out among outpatients attending the HIV/AIDS clinics at 2 other tertiary centers (University Teaching Hospitals), at Ile-Ife (South-Western Nigeria) and Port Harcout (Southern part of Nigeria). This prevalence of renal disease among Nigerian patients with HIV/AIDS (24%-30.6% or 30.6%-38%) is similar to those of some other African countries: Zambia (33.5%) 29 and Uganda (20%-48.5%) 20,29 but more than others like Kenya (25%), 21 Cote d’Ivoire (26%), 30 and Tanzania (28%). 31 It is however far above Southern Africa (6%). 32
Also, creatinine clearance determined by MDRD equation showing significant difference between the patents and controls’ means demonstrated the evidence that our patients were in moderate through ESRD before initiating HAART. This finding using MDRD equation is similar to the findings by Mauss et al. 33 Racial predilection and genetic factors have been stated to be involved in the development of renal disease in patients with HIV/AIDS. Thus, this finding of renal function impairment in this population of Africans is consistent with previous studies. In this study, majority of patients were in stage 2 CKD, while some had already progressed to stages 3, 4, and 5 of CKD. It can thus be inferred that HIV/AIDS is one of the major factors to be considered in the etiopathogenesis of chronic renal failure in Nigeria. This is consistent with the fact that over the last 2 decades, there has been an exponential increase in the prevalence of HIV in different communities of the Nigerian population. 34 The increase in the prevalence of chronic renal failure thus parallels that of HIV/AIDS. This has been corroborated by other researchers who found the estimated prevalence of chronic renal failure among Nigerian patients to be about 300 to 400 per million. 35,36
Our study has some important limitations. First, renal biopsies were not performed on the patients in our study. This would have been included in our original design, and it would have assisted in diagnosing those with HIVAN (especially among those with eGFR values consistent with stages 3-5 of CKD), since the definitive diagnosis of HIVAN is based on renal biopsy. Second, urinary protein to creatinine ratio, whose elevation is a useful indicator of kidney damage, was not done for our patients, and it should have added more strength to our findings of declined GFR since heavy proteinuria and rapid progression to ESRD are characteristic of HIVAN. Third, given the cross-sectional nature of our study, we could not assess adequately the time frames for the development of CKD (declined GFR). However, the predominantly low CD4 counts suggest late presentation for assessment, testing, and diagnosis, and of course the possibility of persistently reduced GFR even beyond the 3 months’ duration for CKD case definition, as most of the patients have been experiencing the symptoms for a long time before ever presenting themselves for investigation and appropriate diagnosis. The late presentations for HIV testing despite the advanced signs and symptoms could have been contributed to by ignorance in some patients and also fear of stigmatization after testing in some others.
Because there is a growing concern that HIV/AIDS has a significant contribution to the prevalence of CRF worldwide, further studies of the prevalence of this causation in different populations are necessary. Findings from all such studies can be useful for better population-based health care planning and delivery. Therefore, the data from this study will influence decisions on ART selection and provisioning in Nigeria—especially as potentially nephrotoxic drugs are introduced (like tenofovir [TDF] or ritonavir (RTV)-boosted protease inhibitors). The data obviously will be a form of alert message to the providers of AIDS care in Nigeria, knowing this high prevalence of abnormal renal function in our HIV-infected population. It will provide a basis for appropriate pre-HAART screening of the renal function status to preclude wrong adduction of renal dysfunction that is subsequently discovered after initiating HAART to adverse effects of drugs. Also, the data will enhance their compliance with and adherence to the guidelines for initial ART and considerations in patients with specific conditions. 18 For example, in individuals with CKD, possible backbone drugs will include abacavir (ABC), emtricitabine, and lamivudine (3TC); TDF will be avoided in persons with glomerular and tubular damage; possible third agent will be efavirenz (EFV), nevirapine (NVP), raltegratvir, or maraviroc; other potentially nephrotoxic drugs will be avoided; and if potentially nephrotoxic drugs must be used, renal function will be monitored closely. For patients with reduced eGFR, dose adjustment for drugs with renal metabolism (emtricitabine, 3TC, TDF, and maraviroc) will be appropriately advised.
Footnotes
Acknowledgments
The authors wish to thank Dr H. O. Olawumi and Dr S. B. Babatunde of the Department of Haematology, University of Ilorin Teaching Hospital, Ilorin, Nigeria, for their assistance during the proposal stage of the work. The authors are also grateful to their colleagues in the Department of Chemical Pathology, University of Ilorin Teaching Hospital; Dr Sikiru A. Biliaminu, Dr Abdulazeez, Dr Abdulrahaman, and Dr Oni for their logistics support. The authors also appreciate the efforts of research assistants, Mr Wale Olalere (HND, Science Laboratory Technology) and Sola (OND, Science Laboratory Technology) in the aspect of sample collection. Unforgettable are the efforts of Mrs Alhaja Ajayi, Mr Latifat Vincent, Mr Festus, and Mr Francis (specimen reception staff members of the Department of Chemical Pathology, University of Ilorin Teaching Hospital) in the aspect of sample separation, aliquoting, and storage. The authors appreciate the great assistance of Miss Matthania Erasmus (BSc Economics) in the aspects of mathematical calculations and final data entry into excel sheet. We appreciate the indispensable effort of the public health statisticians (Mr Ezra Babatunde, HND Statistics and Mr Adegboye Yemi, BSc Statistics) for their assistance in the statistical analysis of the data using SPSS (Statistical process control for Microsoft Excel software). The authors also wish to thank all the participants who participated in this study.
Authors’ Note
Study conception and design was originally by Dr Tewogbade Adeoye Adedeji and Prof Simeon Adelani Adebisi. Data were acquired by Dr Tewogbade Adeoye Adedeji (with research assistants: Mr Wale Olalere, Mr Sola, and Miss Matthania Erasmus). Data analysis was handled by Dr Tewogbade Adeoye Adedeji (with public health statisticians: Mr Ezra Babatunde and Mr Adegboye Yemi). Dr Tewogbade Adeoye Adedeji and Prof Simeon Adelani Adebisi interpreted the data. Drafting of the article was done by Dr Tewogbade Adeoye Adedeji and Prof Simeon Adelani. Proofreading of the article and other general corrections were done by Dr Nife Olamide Adedeji and Dr Ademola Idowu. All authors critically reviewed the article for its important intellectual content. All authors finally approved the version to be submitted. The corresponding author “had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.”
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.