
Abstract
Background:
Late presentation of patients contributes significantly to the high mortality reported in HIV -care and treatment programs in sub-Saharan Africa.
Methods:
A cross-sectional study was conducted to assess factors associated with late engagement to HIV care at the Academic Model Providing Access to Healthcare in western Kenya. Late engagement was defined as baseline CD4 ≤100 cells/mm3.
Results:
Of the 10 533 participants included in the analysis, 67% were female and mean age was 36.7 years. Overall, 23% of the participants presented late. Factors associated with late engagement included male gender (adjusted odds ratio [AOR]: 1.54, 95% confidence interval [CI]: 1.35-1.75), older age (AOR: 1.62, 95% CI: 1.02-2.56), and longer travel time to clinic (AOR: 1.18, 95% CI: 1.04-1.34).
Conclusion:
Nearly one-quarter of HIV-infected patients in our setting present with advanced immune suppression at initial encounter. Being male, older age, and living further away from clinic are associated with late engagement to care.
Introduction
Late presentation of patients contributes significantly to the high mortality reported in HIV care and treatment programs in sub-Saharan Africa. Patients presenting with advanced immunosuppression (CD4 count ≤ 100 cells/mm3) have an increased risk of opportunistic infections that are responsible for high mortality rates. 1 –3 Delays in initiation of antiretroviral therapy (ART) further worsen clinical outcomes. 4 –6 In sub-Saharan Africa, only an estimated 59% of those testing positive for HIV are linked to care. 7 Further, there are significant delays between testing positive for HIV and engagement to HIV care. The success of ART programs in sub-Saharan Africa will largely depend on efforts to ensure that transition from HIV testing to medical care is made less complicated and less prone to delays. 8 Factors responsible for late engagement in the era of free ART have not been well studied.
An estimated 30% to 40% of patients initiating HIV care in sub-Saharan Africa are late presenters. 9 –11 Late presentation to HIV care is associated with significantly higher health care–related costs compared with early presentation. 12 This is due to the high cost of treatment for opportunistic infections in patients with advanced immunosuppression. Further, late patient presentation is likely to be a major impediment in the control of the HIV epidemic, even as new evidence shows that early treatment (test and treat) is an effective prevention strategy. 13,14 Factors that have been linked to late engagement to care include unemployment, being unmarried, and lower education level. 9 Others include perception that HIV care is unnecessary until one falls sick, denial of one’s HIV status, nondisclosure, long distance to health facilities, and not receiving help in making HIV care appointments. 15 –18
In 2010, the World Health Organization (WHO) revised its recommendations to the timing of ART initiation in HIV-infected adults. The CD4 count threshold was raised to 350 cells/mm3, up from the previously recommended 250 cells/mm3. 19 This recommendation was adopted by the Kenya National ART guidelines and specifically at the Academic Model Providing Access to Healthcare (AMPATH) program in western Kenya. Despite adopting these recommendations, patients continued to present with advanced immunosuppression at their initial encounter at the clinics. To address the problem of late presentation to care, AMPATH has established a home-based counseling and testing (HBCT) program. 20 This entails community-based door-to-door counseling and testing for HIV and linkage to the nearest ART clinic. HBCT was initiated in 2007 and has covered most of the catchment population of AMPATH. Data from HBCT have shown that patients who are linked to care through it have less advanced disease than those accessing care through provider-initiated testing and counseling (PITC) or tuberculosis (TB) clinics. 21
Overall, in this setting, there has been a trend toward higher median baseline CD4 count for new enrollees between 2001 and 2009. 22,23 However, we continue to see patients who present with advanced immunosuppression within our clinics. The latest WHO HIV treatment guidelines released in June 2013 recommend initiating ART at a CD4 count threshold of 500 cells/mm3 for individuals with asymptomatic HIV infection. 24 To successfully implement these recommendations, a thorough understanding of factors that contribute to late engagement to care is important in order to formulate strategies that promote early testing and treatment. We examined the factors that contribute to late engagement to care at AMPATH clinics in western Kenya.
Methods
Ethical Approval
This study was approved by the Moi University/Moi Teaching and Referral Hospital (MTRH) Institutional Research and Ethics Committee and Indiana University School of Medicine Institutional Review Board. Patient-informed consent was waived by the regulatory bodies since these data are collected for the conduct of clinical care and de-identified prior to analysis.
Setting
This study was conducted at the AMPATH program in western Kenya. This is a well-established ambulatory HIV care and treatment program that serves a catchment population of 4 million people in western Kenya. Academic Model Providing Access to Healthcare is a collaboration between Moi University School of Medicine, MTRH, and a consortium of North American Universities led by Indiana University. Since its inception in 2001, AMPATH has enrolled over 150 000 HIV-infected patients of whom over 90 000 have initiated ART. Academic Model Providing Access to Healthcare has established 80 regional HIV treatment clinics in county and subcounty hospitals as well as in health centers across the region. Patient data are captured and stored in the AMPATH Medical Record System, an electronic database that served as the sampling frame for this study. 25 The HIV prevalence in the region is 7.1%. 26
The adult ART guidelines in use during the period of this study recommended initiation of treatment for patients with a CD4 count of
Study Population
We included patients aged 14 years and older enrolled into the AMPATH clinics between December 1, 2010, and December 31, 2011. The initial date mentioned previously coincided with the local adoption of the ART guidelines recommending initiation of ART at a CD4 count threshold of
Study Design and Data Sources
We performed a retrospective analysis of prospectively collected data from an HIV clinical program. Data were extracted from the database of AMPATH electronic medical records. All participants meeting the inclusion criteria mentioned previously were included in the analysis.
Data Analysis
Variables included
The baseline CD4 count was considered the dependent variable. A CD4 count of ≤100 cells/mm3 was used as a surrogate for late engagement. An a priori decision was made to include the following explanatory variables suspected to be associated with late engagement to care in this analysis: travel time to clinic (<1 versus ≥1 hour), gender (male or female), age (<19, 19-24, and >24 years), education (number of school years completed), disclosure status (yes and no), and economic status (employed versus unemployed). Others were social support (living with partner versus not having a partner), alcohol use (yes and no), presence versus absence of psychiatric illness, presence or absence of TB at baseline, having clinical symptoms at baseline, and point of entry into care (voluntary counseling and testing [VCT] or PITC/TB clinic versus HBCT/prevention of mother-to-child transmission [PMTCT] clinic).
Statistical analyses
Parametric and nonparametric descriptive statistics were employed to summarize both categorical and continuous variables. For continuous variables, mean and median together with standard deviation (SD) and interquartile range (IQR) were calculated. The chi-square test was used to test for associations between categorical/dichotomous variables. T test was also used to compare means across the groups (early versus late engagement to care).
The main outcome variable was late engagement to care. The explanatory and dependent variables were coded as binary/categorical variables or left at their continuous scale prior to fitting in the final model. For late engagement to care this meant that 1 = participants with baseline CD4 count ≤100 cells/mm3 (late engagement) and 0 = if otherwise. Initially, explanatory variables were included in the model one at a time to examine their bivariate association with late engagement to care. Univariate logistic regression models were performed to determine the variables that were associated with late engagement to care. For both univariate and multivariate logistic regression models, the following predictor variables were considered: age, gender, years of schooling, HIV disclosure, travel time to clinic, presence of clinical symptoms, TB status, alcohol use, social support, and employment status. Multivariate logistic regression model was used to model the effects of all the variables simultaneously or those hypothesized a priori to be strong predictors of late engagement to care. Adjusted odds ratios (AORs) and 95% confidence intervals (CIs) were reported. All the analyses were carried out by using SAS® version 9.3 (SAS Institute Inc., Cary, NC).
Results
Of the 10 533 participants included in the analysis, 67% were female. The mean age at enrollment was 36.7 years (SD 11.0). Only 25% had completed secondary school education. The median baseline CD4 count was 258 cells/mm3 (IQR 111-437). Overall, 2421 (23%) participants presented late (baseline CD4 count ≤100 cells/mm3). Of these, 1413 (58%) had baseline CD4 count ≤50 cells/mm3. Among the late presenters, the median CD4 count was 41 cells/mm3 (IQR 17-70). Other baseline demographic characteristics are shown in Table 1. As illustrated, over 80% of the participants were unemployed and over 70% had disclosed their HIV status. Among ART-eligible patients, the median time from program enrollment to ART initiation was 28 days (IQR 14-44).
Baseline Demographic Characteristics of the Study Patients.a
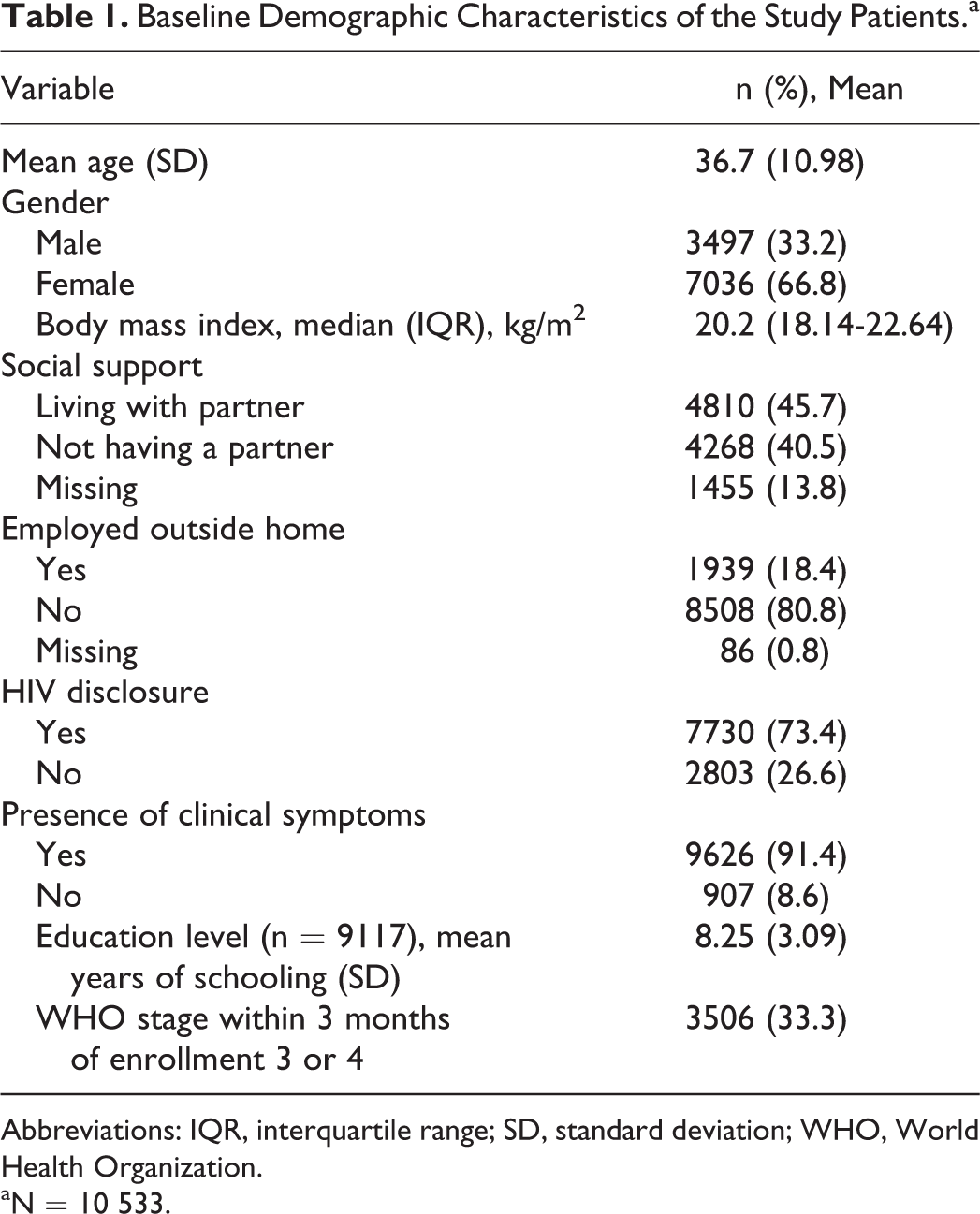
Abbreviations: IQR, interquartile range; SD, standard deviation; WHO, World Health Organization.
aN = 10 533.
Results of bivariate association between early versus late engagement to care among HIV-infected adult patients are shown in Table 2. As illustrated, factors significantly associated with late engagement to care included male gender, older age, longer travel time, having TB, and being employed.
Results of the logistic regression model of factors associated with late engagement to care are presented in Table 3. As illustrated, factors that were associated with late engagement to care included male gender (AOR: 1.54, 95% CI: 1.35-1.75), older age (AOR: 1.62, 95% CI: 1.02-2.56), and more than 1-hour travel time to clinic (AOR: 1.18, 95% CI: 1.04-1.34). In addition, individuals with TB tended to present late for care compared with those without (AOR: 2.77, 95% CI: 2.40-3.19). Point of entry into HIV care was also an important factor. Participants who accessed care through VCT were more likely to present late compared to those who accessed care through HBCT (AOR: 3.23, 95% CI: 2.38-4.39). Similarly, those who accessed care through PITC/TB clinic were more likely to present late compared to those who accessed through HBCT (AOR: 4.03, 95%CI: 3.00-5.43).
HIV disclosure and years of education were not significantly associated with late engagement to care. Unexpectedly, alcohol use was associated with reduced likelihood of late engagement to care (AOR: 0.67, 95% CI: 0.57-0.80).
Bivariate Association between Early versus Late Engagement to Care among HIV-Infected Adult Patients.

Abbreviations: SD, standard deviation; TB, tuberculosis. asignificant p value (p < 0.05)
Unadjusted and Adjusted Logistic Regression Models of Factors Associated with Late Engagement to Care.

Abbreviations: CI, confidence interval; HBCT, home-based counseling and testing; PITC, provider-initiated testing and counseling; PMTCT, prevention of mother-to-child transmission; TB, tuberculosis; VCT, voluntary counseling and testing.
aReference category.
Discussion
Despite the changing epidemiology of HIV (increasing median CD4 count at presentation), we still have a large number of patients presenting late. Compared to earlier studies in the same setting (in the 2001 to 2004 period), the median CD4 count at ART initiation has increased significantly from 86 to 258 cells/mm3 in this study. 22,23 Our study demonstrates that nearly one-quarter of new enrollees continues to be severely immunosuppressed when they engage with care. Those most likely to engage in care late in their disease are men, those who are older, those who live further from clinics, or those have TB. In addition, those who access care through entry points other than HBCT or PMTCT are likely to present late. Our findings are generally in keeping with data from other programs in sub-Saharan Africa as discussed subsequently.
Our study confirmed findings from previous studies that male gender is an independent predictor of late engagement to care. 9,10,23,27,28 It is presumed that African males tend to seek health care much later compared to their female counterparts because of masculine ideas of strength, pride, and time constraints among working breadwinners. 29,30 In addition, health care systems in Africa have failed to address challenges that hinder men’s access to care. For instance, many ART programs in Africa have documented poorer access and higher mortality among men compared to women, but there has not been any policy framework targeted at improving men’s access to health care. 31 Many programs concerned with gender equality have brought to the fore issues affecting women and children but often fail to address problems affecting men.
We found that older patients had a higher likelihood of late presentation compared to younger patients. Similar observations have been made in other studies. 32 –35 Older patients are perceived to be at low risk for HIV infection and are not frequently offered HIV testing by health care practitioners. 36 Indeed, heterosexual individuals older than 50 years are hardly a target of HIV prevention efforts. 37 Psychological factors such as depression, which is more common in older adults, may also hinder access to health care. 38
We observed that patients with TB presented later for care than those without. HIV-associated TB can occur at diverse CD4 counts, including the upper end of the spectrum. 39 However, TB tends to be more common at CD4 counts <200 cells/mm3. 38,40,41 Thus, this observation may simply reflect colinearity between low CD4 count and susceptibility to TB. However, another possible explanation is that patients with TB delay seeking HIV care because of perceived stigma fueled by the dual epidemic. 42 –51 Alternately, the observed association between TB and late presentation may be attributed to the fact that TB infection in itself leads to rapid progression of HIV disease. 52,53
In our program, there are minimal delays in the initiation of ART among enrolled participants who are known to be eligible for ART. The median duration between enrolment into care and initiation of ART was 28 days (IQR 14-44). This is a much shorter period compared with a study in Uganda, which reported a median of 105 days. 54 Our data show that patients who access HIV care through HBCT tend to present earlier than their counterparts who access care through VCT, PITC, or TB clinics.
Study Limitations and Strengths
The main limitation of this study is that we used baseline CD4 count as a surrogate marker for late engagement into care. Since the HIV virus has a different trajectory in each host, an individual with low baseline CD4 count may not necessarily have had a longer duration of HIV infection compared to one with higher CD4 count. Another limitation is that since this was a retrospective review, we were not able to conduct interviews with patients to establish the impact of factors such as stigma and health beliefs on health-seeking behavior. The main strength of this study is that it was conducted in routine (nonresearch) clinical setting and included a large sample size. The results are therefore a true reflection of HIV care programs in similar settings.
Conclusion and Recommendations
Nearly one-quarter of HIV-infected patients in our setting presents with advanced immune suppression at initial encounter. Being male, older in age, living further away from clinic, having TB, and accessing care through VCT or PITC as opposed to HBCT are associated with late engagement to care. There is an urgent need to identify innovative ways to engage males in testing, target older individuals, establish more satellite clinics, expand HBTC coverage, and ensure that TB clinics are testing for HIV at presentation into care.
Footnotes
Acknowledgements
The authors thank the patients, clinicians, and the data team who made this work possible.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The AMPATH clinical care program is supported by the President's Emergency Plan for AIDS Relief (PEPFAR) through USAID under the terms of Cooperative Agreement No. 623-A-00-08-00003-00.