
Abstract
We report the case of a 33-year-old HIV-infected man who presented with a recurrent, nonhealing perianal fistula. After multiple benign biopsies, the diagnosis of plasmablastic lymphoma (PBL) eventually was made. The patient underwent chemotherapy and radiation with a complete response. Perianal fistulas are frequent in HIV-positive patients, but PBL as a cause is extremely rare. This often delays the diagnosis and treatment of this highly aggressive disease. We review the literature and discuss the pitfalls in the diagnosis and management of the disease.
Introduction
Perianal fistulas are the second most common manifestation of perianal disease in HIV-positive patients. 1 Common causes of perianal fistula include viral, bacterial, and fungal infections; venereal diseases; cancers; anal fissures; radiation; and trauma. Among the malignant causes, squamous cell carcinoma is the most frequently reported, with lymphomas being unusual in this location. We report the case of plasmablastic lymphoma (PBL) presenting as a perianal fistula in an HIV-infected patient. Plasmablastic lymphoma is a rare, highly aggressive subtype of diffuse large B-cell lymphoma (DLBCL) usually seen in HIV-positive patients. It is commonly seen in the oral cavity, anal PBL is rare with only 10 reported cases. The rarity of the diagnosis and difficulty in obtaining large biopsy samples can often delay diagnosis and hence treatment of this highly aggressive malignancy.
Case Report
A 33-year-old HIV-infected man presented with a 2-month history of perianal pain, subjective fevers, and diarrhea. He had been diagnosed with HIV 8 years ago but had been noncompliant with therapy for the last 3 years. Physical examination revealed a raised, 2 × 1 cm2 perianal ulcer extending from the anus to the left buttock. Digital rectal examination was negative for any anorectal mass. Computed tomography (CT) scan of the abdomen and pelvis did not report any evidence of focal fluid collection, masses, or lymphadenopathy in the rectal area. Complete blood count was normal, HIV-1 RNA was 31 404 copies/mL, CD4 count was 66/mm3, lactate dehydrogenase was 754 U/L, and the test for Epstein-Barr virus (EBV) by polymerase chain reaction on peripheral blood was negative. He was diagnosed with an anal fistula and underwent a fistulotomy.
Four weeks postprocedure, the patient returned with complaints of frequent soiling of his undergarments. Physical examination confirmed a 1 × 1 cm2 draining perianal ulcer, with an open fistulotomy tract. Patient underwent a colonoscopy, which revealed a perianal ulcer in the presence of an otherwise normal colonic mucosa. Biopsies were obtained from the edges of the fistulotomy tract, which revealed sheets of neoplastic cells, with scattered positivity for CD79a and nonspecific staining with plasma cell markers, κ, and lambda stains. This was reported as a poorly differentiated malignant neoplasm, and more tissue was requested for further evaluation. Repeat CT scan of the abdomen and pelvis showed posterior rectal wall thickening, an enterocutaneous fistula, and a 1.4-cm right inguinal lymphadenopathy. No retroperitoneal lymphadenopathy was noticed. An open biopsy was scheduled as an outpatient.
Patient delayed the biopsy and eventually presented 4 weeks later with severe anal pain and discharge. Computed tomography scan revealed a 10.9 × 8.9 cm2 fluid collection in the anal area with bilateral-enlarged inguinal nodes (Figure 1A). Excisional biopsies of the left inguinal lymph node and the perianal mass revealed a poorly differentiated malignant neoplasm composed of large cells with scant cytoplasm and eccentric large round nucleus with prominent nucleoli and increased mitotic activity, consistent with monotypic plasmablasts (Figure 2A). These cells expressed CD38 and CD138 with κ light chain restriction (Figure 2B), while being negative for CD20, CD45, and CD56. Bone marrow biopsy did not reveal any involvement with lymphoma. A diagnosis of stage IIA bulky anal PBL was made.
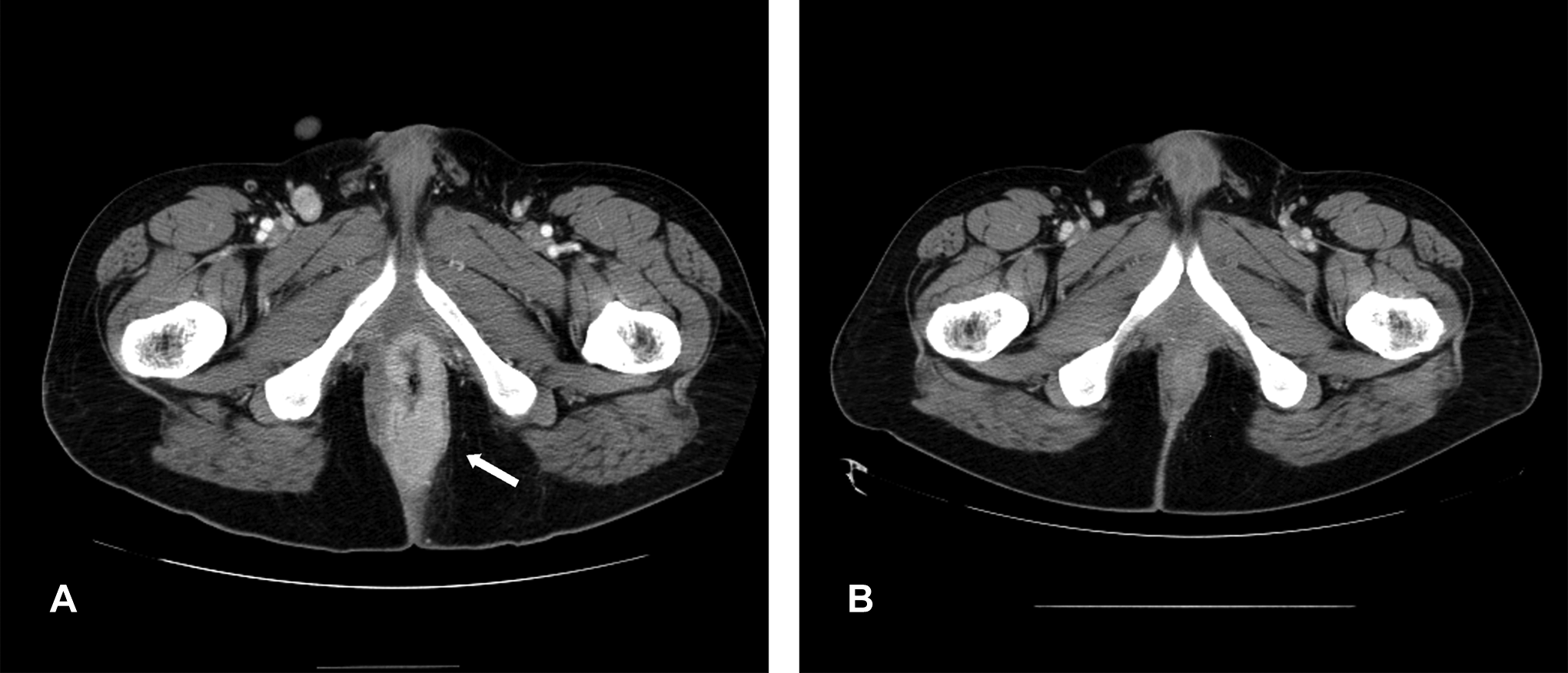
A, Pretreatment CT scan of the pelvis showing a 10.9 × 8.9 cm2 mass (white arrow) in the anal area. B, Posttreatment CT scan of the pelvis showing complete resolution of the rectal wall thickening and perianal mass. CT indicates computed tomography.

A, Hematoxylin and eosin stain. Diffuse infiltration of large plasmablastic cells with tangible body macrophages. B, Immunoperoxidase stain CD138 strongly positive.
Chemotherapy with cyclophosphamide, doxorubicin, vincristine, and prednisone (CHOP) regimen was initiated. After just 3 cycles of treatment, there was complete healing of the anal fistula with resolution of the rectal wall thickening and inguinal lymphadenopathy. He went on to complete 6 cycles of chemotherapy followed by 5 weeks of radiation therapy (3000 cGy with accumulated dose of 4190 cGy). A CT scan done 5 months after completing treatment did not reveal any residual disease (Figure 1B). Patient subsequently moved to a different state and was lost to follow up.
Discussion
Plasmablastic lymphoma is an aggressive and rare variant of DLBCL and accounts for approximately 3% of all HIV-related non-Hodgkin lymphomas. 2 It was first described in 1997 in the oral cavity of an HIV-positive patient. 3 Although mostly reported in HIV-positive patients, it has been reported in other immunocompromised states and even in immunocompetent individuals.4,5 Plasmablastic lymphoma was initially thought to be an exclusively oral disease, 3 but subsequent reports described its occurrence at sites like the stomach, 6 lungs, 7 skin lymph nodes, soft tissue, and bone marrow.8 –11 There are fewer than 50 reported cases of extra oral PBL in HIV-positive patients, of which only 7 were reported to originate in the anal canal.8,12 –15 Most of them presented with bleeding and anal mass. Three other cases of anal PBL have also been reported in non-HIV-positive patients.5,16,17 The findings are summarized in Table 1.
Cases of Perianal PBL Reported in Literature.
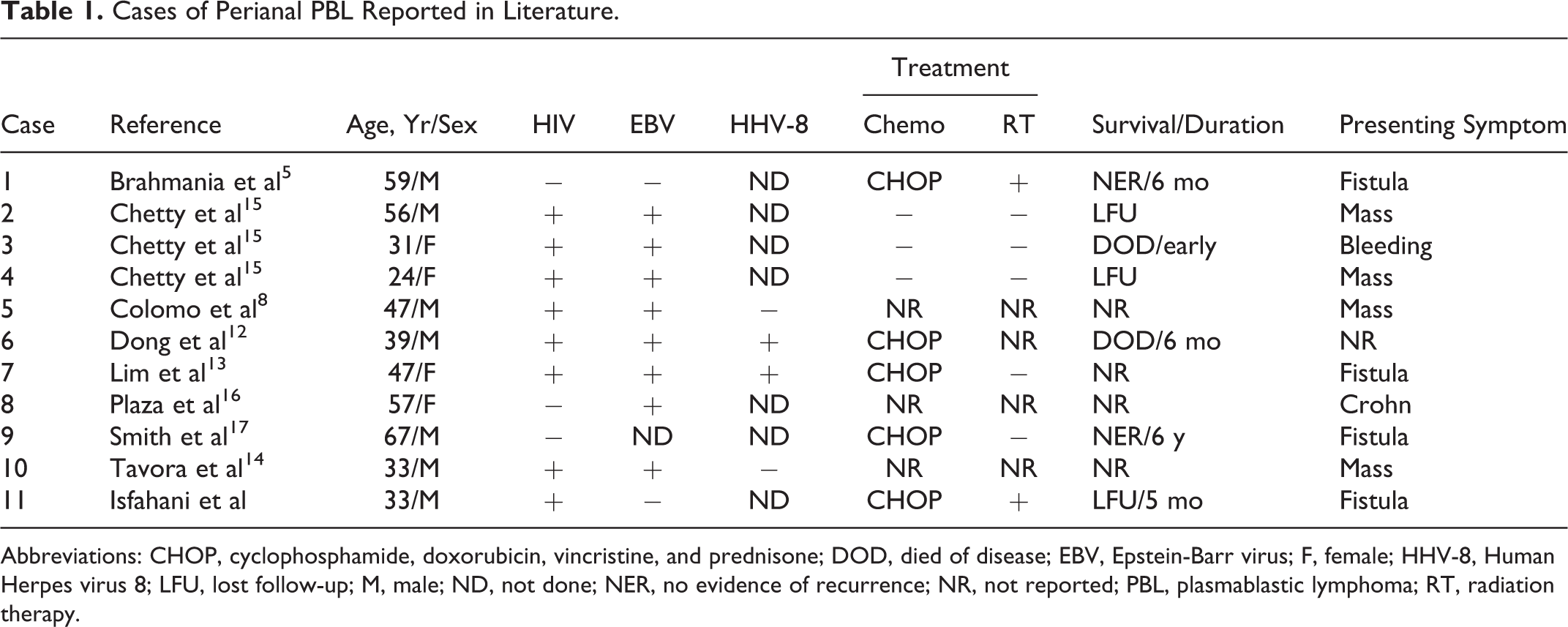
Abbreviations: CHOP, cyclophosphamide, doxorubicin, vincristine, and prednisone; DOD, died of disease; EBV, Epstein-Barr virus; F, female; HHV-8, Human Herpes virus 8; LFU, lost follow-up; M, male; ND, not done; NER, no evidence of recurrence; NR, not reported; PBL, plasmablastic lymphoma; RT, radiation therapy.
Pathologic features of PBL are characterized by large monotypic cells with large nucleus and prominent nucleoli and blastoid morphology. These cells show strong expression of plasma cell markers like CD38 and CD138 but weak/absent expression of B-cell markers such as CD20 and CD45. 8 Pathogenesis of PBL is strongly associated with EBV infection. 2 Human herpesvirus 8 has also been linked to PBL but not as strongly as EBV, and its exact role remains unclear.12 –14
Plasmablastic lymphoma is a highly aggressive tumor and is poorly responsive to treatment. Most commonly used therapy is CHOP with or without radiation therapy. More aggressive regimens such as cyclophosphamide, oncovin, doxorubicin, methotrexate, ifosfamide, etoposide, and cytarabine have also been used with limited success. Prognosis is based on the response to highly active antiretroviral therapy and immunologic status. Median survival in 1 series was only 15 months despite therapy. 18
Conclusion
Plasmablastic lymphomas should be considered as a possible diagnosis in any HIV-infected patient presenting with a nonhealing perianal lesion or fistula. As illustrated by our case, initial benign biopsies can often mask this highly aggressive tumor. Delay in diagnosis can be prevented by having a low threshold for performing an open or excisional biopsy in cases of recurrent perianal fistulas not responding to conventional therapy.
Footnotes
Authors’ Note
This article has not been submitted for publication elsewhere, although it has been previously presented as a poster at an American College of Physicians Meeting.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.