
Abstract
Introduction:
In 2012, the American Academy of Pediatrics (AAP) and the American Congress of Obstetricians and Gynecologists (ACOG) published recommendations that physicians should discuss with parents the benefits and risks of newborn male circumcision. Our objective was to assess physicians’ perspectives of newborn male circumcision.
Methods:
A self-administered, cross-sectional electronic survey of US physicians was conducted in 2008 (N = 1500).
Results:
Approximately one-third (33.2%) of the respondents reported that their current perspective was that the medical benefits outweigh the risks associated with newborn male circumcision and less than one-third (31.1%) reported they would recommend the procedure when counseling parents.
Conclusions:
In 2008, only about one-third of the physicians surveyed thought that the benefits of male circumcision outweighed the risks and recommended it to parents of newborn sons. These attitudes may be relevant to the declining circumcision rates in the United States. Repeat surveys may be useful, given the new AAP and ACOG recommendations.
Introduction
The routine circumcision of newborn male infants has generated debate in the United States.1,2 Detractors believe that the procedure is unethical, constituting mutilation of the genitalia without the child’s consent, 3 while advocates believe that circumcision is in the long-term best interest of the child.3,4 The medical benefits of male circumcision include lower rates of penile cancer, infant urinary tract infections, and sexually transmitted infections.5,6 In addition, studies have shown a benefit of male circumcision not only for the males but also for their female sexual partners against certain sexually transmitted infections. 7 Since 2005, in Africa 3 clinical trials have found that adult male circumcision is partially effective in preventing the transmission of HIV infection from infected female partners to uninfected males.6,8,9
Prevalence of male circumcision in the United States varies by race/ethnicity, with the highest rates reported in non-Hispanic whites (79%) and the lowest among Mexican Americans (42%). 10 A recent publication that analyzed 3 different independent data sources reported that there has been a significant decline in the newborn male circumcision rates in the United States (eg, National Hospital discharge data 62.5% in 1999 to 56.9% in 2008). 11 Parents are responsible for making the final decision about whether to circumcise their sons; their decision may be influenced by various factors including social norms, the father’s circumcision status,12–15 medical benefits, 16 and possibly the availability of Medicaid coverage 17 as well as the physicians’ knowledge and beliefs about the procedure. In a survey study, 87% of parents reported that their child’s health care provider was one of the 3 most important sources of information that influenced their decisions about their child’s health care. 18 There are little data on physician specialties who perform newborn male circumcision, but 1 survey study of pediatricians, family or general practitioners, and obstetricians/gynecologists (OB/GYNs) reported that 54% perform at least 1 circumcision per month (pediatrician: 35%; family or general practitioner: 60%; and OB/GYN: 70%). 19
In August 2012, the American Academy of Pediatrics (AAP) Task Force on Circumcision published recommendations based on their critical review of the peer-reviewed literature. They changed their previous recommendations on this procedure by stating that the health benefits of newborn male circumcision outweigh the risks. Moreover, they stated that families who choose the procedure for their newborn sons should have access to it. 20 The American Congress of Obstetricians and Gynecologists shortly thereafter endorsed the AAP recommendations. 21
The purpose of the present study was to (1) identify the proportion of physicians who, prior to the issuance of these recommendations, believed the medical benefits of newborn male circumcision outweighed the risks, (2) determine factors associated with these physicians compared to others, and (3) describe how they counseled parents on newborn male circumcision, especially by both physicians who reported they do and who reported they do not believe that the medical benefits of newborn male circumcision outweigh the risks.The current study provides baseline information on physicians’ perspectives on newborn male circumcision prior to the change in AAP recommendations. 20
Methods
Participant Review
The Centers for Disease Control and Prevention, Human Subject Review Office, has determined that Styles surveys (ConsumerStyles, HealthStyles, DocStyles, and YouthStyles) constitute exempt research in accordance with the criteria outlined in 45 CFR 46.101(b)(2). 22
Participants and Procedure
Porter Novelli, Inc conducted a Web-based survey of physicians and other specialties (DocStyles) in 2008 using a quota sampling method. Quota sampling allows a target number of persons to be selected from several classifications. 23 The quota for the DocStyles survey included 1000 primary care physicians, 250 pediatricians, 250 OB/GYNs, 250 dermatologists, and 130 registered dietitians.
The sample was drawn from Epocrates Honors Panel, a verified panel of 135 000 medical practitioners. These practitioners use Epocrates’ software (about 50% of all physicians) and can choose to sign up or opt in when they download applications and software by filling out a brief application. They are then sent an e-mail with a link to the background survey. For the DocStyles survey, Epocrates randomly selected a sample of eligible physicians from their main database to load into their invitation database. This sample was drawn to match the American Medical Association’s (AMA) master file proportions for age, gender, and region. Invitations included a link to the Web-based survey, which was hosted by ResearchNow. Verification was achieved by checking each physician’s first name, last name, date of birth, medical school, and graduation date against the AMA master file at the time of panel registration. The AMA physician master file includes current data on all physicians in the United States, both AMA members and nonmembers, as well as credentialed graduates of foreign medical schools.
The physicians included in the database were those who practiced in the United States; actively saw patients; worked in an individual, group, or hospital practice; and had been practicing medicine for at least 3 years. Respondents were free to refuse participation and could exit the survey at any time. To protect respondent confidentiality, no individual identifiers were included in the database.
Survey
Porter Novelli developed the DocStyles survey instrument with technical guidance from federal public health agencies and other nonprofit and for-profit clients. The survey, conducted during July 2008, included 140 questions (some with multiple subparts). The questions were designed to provide insight into physicians’ attitudes and counseling behaviors about a range of health issues and to assess their use and trust of available health information sources. Survey questions can be requested from the senior author. To reach the quota for the DocStyles survey, 14 346 physicians were invited to participate. The incentive for participation was US$50 to US$75. Of physicians invited, 1880 completed the entire survey. Thirty-three respondents did not complete the entire survey, 141 were terminated based on the screener questions, 1088 logged in to take the survey but were terminated due to filled quotas for their specialty, and 11 204 did not respond to the invitation or tried to respond after the survey closed, resulting in an overall 22% response rate. Porter Novelli used the following formula to calculate the response rate based on the percentage of qualified or eligible respondents completing the survey: completes/(completes + [completes/completes + terminated or did not meet criteria + terminated due to filled quota for specialty]) × (no response or responded after survey closed + incomplete survey).
Physicians included in this analysis were restricted to those who saw at least 10 patients a week. Dermatologists and registered dieticians were not included due to their lack of experience with newborn male circumcision. Thus, we did not include all respondents to the DocStyles survey. Only responses from 1500 physicians (510 family or general practitioners, 490 internists, 250 pediatricians, and 250 OB/GYNs) contributed to the analysis.
Measures
The main question of interest was “Which of the following best describes your current perspective on the medical risks and benefits of circumcision of newborn males born in the United States?” The response “none of the above” was excluded from analysis. For the main regression analysis, the 4 possible responses were dichotomized into 2 categories. Respondents who selected the option “The medical benefits outweigh the risks associated with the procedure” (1) were categorized as physicians supportive of newborn male circumcision. Respondents who selected the options “The medical benefits do not justify the risk associated with the procedure” (2), “The medical risks and benefits are approximately equal” (3), or “don’t know” (4) were categorized as physicians not supportive of newborn male circumcision. Independent variables included physician characteristics (physician specialty, physician gender, main work setting, number of years in practice, familiarity with the recent studies regarding HIV, and circumcision in Africa) and patient characteristics (race/ethnicity of majority of patients).
A second question of interest for this study was “When counseling parents about circumcising their infant son, which of the following best describes your current perspective?” The possible options were (1) I would generally recommend it, (2) I would recommend it in some cases, (3) I would not offer an opinion beyond presenting risks and benefits, (4) I would generally not recommend it, (5) don’t know, and (6) none of the above.
Analysis
Bivariate and multivariable regression analyses were used to assess the associations of demographic and other factors with physicians supportive of newborn male circumcision. Bivariate analysis was carried out to calculate unadjusted odds ratios (ORs) and 95% confidence intervals (CIs), and multivariable analysis was carried out to calculate adjusted ORs (aORs) and 95% CIs. All variables, regardless of their significance in the bivariate analysis, were included in the model and selected using a forward model selection procedure with a significance P value of .2 cutoff level as screening criteria to retain only those variables most highly associated with the outcome. Regression analyses excluded those who answered “none of the above.”
Frequencies were used to describe physicians who chose the 4 different options to the question of interest, “Which of the following best describes your current perspective on the medical risks and benefits of circumcision of newborn males born in the United States?” by demographic and practice characteristics. Frequencies were also used to describe how physicians supportive of newborn male circumcision and physicians not supportive of newborn male circumcision counsel parents by physician type.
Results
Demographic and background characteristics of the DocStyles sample of primary care physicians were generally comparable to the AMA master file (Table 1), with the exception of a slightly higher proportion of male physicians. Of the 1500 physicians in our analysis, 498 (33.2%) reported that their current perspective of newborn male circumcision was that the medical benefits outweigh the risks associated with the procedure (supportive of newborn male circumcision), 267 (17.8%) reported that the medical benefits do not justify the risk associated with the procedure, 516 (34.4%) reported that the medical risks and benefits are approximately equal, and 219 (14.6%) reported that they didn’t know (157) or selected the option “none of the above” (62). Characteristics of the physicians stratified by their response are presented in Table 2.
Demographics and Background Characteristics of Physicians Who Identified as Family or General Practitioners, Internists, and Pediatricians in the 2008 DocStyles Survey with a Comparison to the American Medical Association (AMA) Master Filea for Gender, Age, and Region.

Abbreviations: NA, not available; OB/GYN, obstetrician/gynecologist.
a AMA master file numbers taken from Final DocStyles Methods 2008 and do not include dermatologists and registered dieticians who participated in survey.
Demographic and Practice Characteristics of Physicians Who Responded to the Question “Which of the Following Best Describes Your Current Perspective on the Medical Risks and Benefits of Circumcision of Newborn Males Born in the US?”a
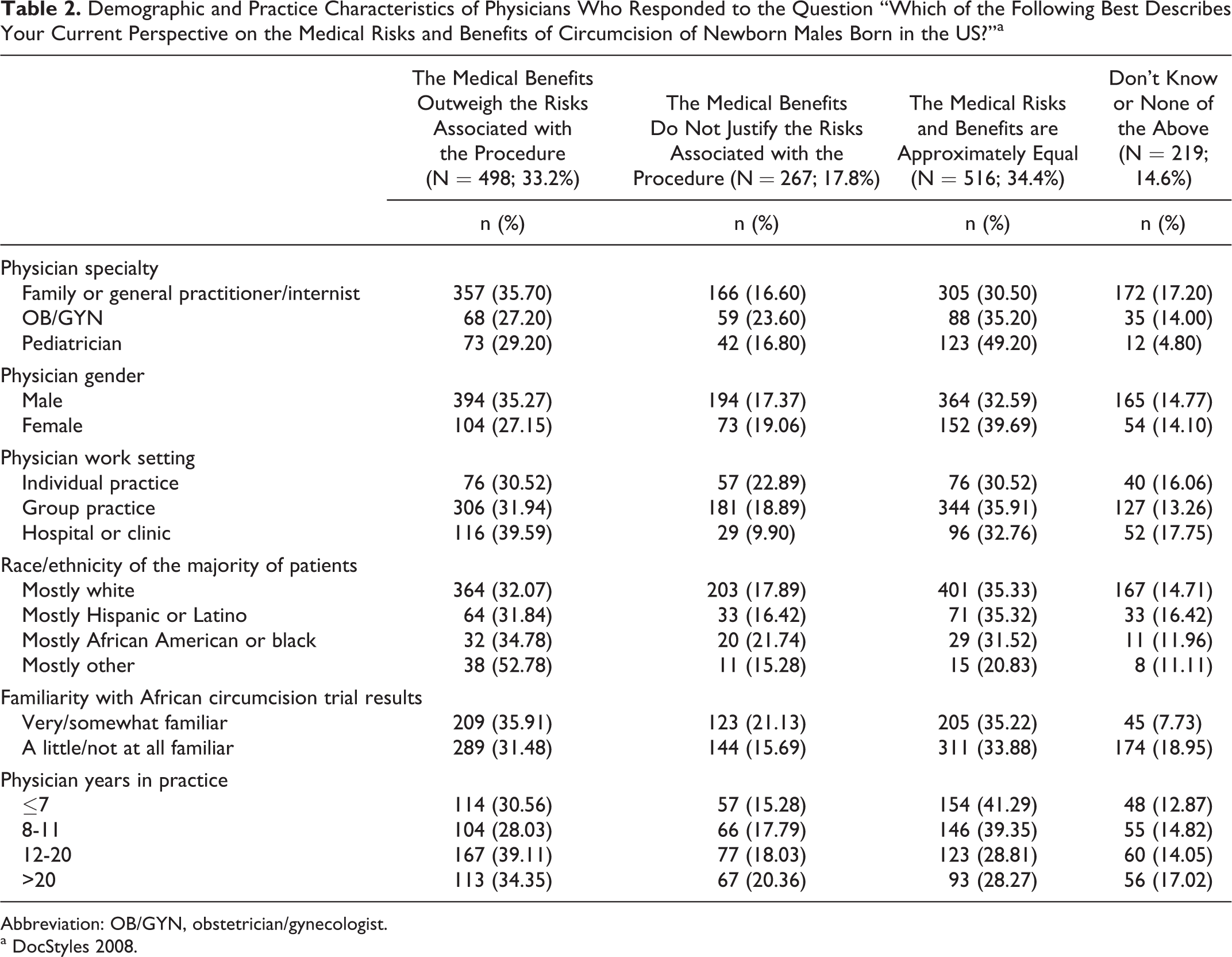
Abbreviation: OB/GYN, obstetrician/gynecologist.
a DocStyles 2008.
Multivariable Regression Analysis: Factors Associated with Physicians Supportive of Newborn Male Circumcision
The odds of reporting being supportive of newborn male circumcision were greater among family or general practitioners/internists than among OB/GYNs (aOR = 1.478, CI = 1.072-2.038) and among physicians with mostly African American or black patients (aOR = 2.577, CI = 1.552-4.278) than among physicians with white patients. There was no significant difference between pediatricians and OB/GYNs (aOR = 0.978, CI = 0.650-1.472; Table 3).
Factors Associated with Physicians Who Believe the Medical Benefits of Newborn Male Circumcision Outweigh the Risks (Supportive of Newborn Male Circumcision).a

Abbreviations: OR, odds ratio; aOR, adjusted odds ratio; CI, confidence interval; OB/GYN, obstetrician/gynecologist.
a DocStyles 2008.
b The above analysis excluded those who answered the question, “none of the above.”
c Significant aOR.
Odds of reporting being supportive of newborn male circumcision were less among female (aOR = 0.651, CI = 0.497-0.853) than among male physicians and also among physicians in an individual (aOR = 0.554, CI = 0.376-0.817) and group practice (aOR = 0.647, CI = 0.481-0.869) than among physicians in a hospital setting. There was no significant association between physicians supportive of newborn male circumcision and familiarity with African male circumcision trial results (aOR = 0.820, CI = 0.651-1.033).
Counseling Parents about Circumcising Their Infant Son
Overall, less than one-third (31.1%) of the 1500 physicians in our analysis reported they would generally recommend male circumcision when counseling parents about circumcising their newborn son. However, of the 498 physicians supportive of newborn male circumcision, nearly 72% said they would generally recommend the procedure (Table 4), compared to approximately 11% of the 940 physicians who did not support newborn male circumcision (Table 5). In both of the subgroups, a higher proportion of family or general practitioners/internists reported they would generally recommend newborn male circumcision (support newborn male circumcision, 75.4%; not support newborn male circumcision, 12.0%) than the mean proportion for all specialties combined (support newborn male circumcision, 71.7%; not support newborn male circumcision, 10.7%).
Physicians Supportive of Newborn Male Circumcision: How They Counsel Parents.a,b

Abbreviation: OB/GYN, obstetrician/gynecologist.
a n = 498.
b DocStyles 2008. Those who answered the question “none of the above” were excluded.
Physicians Not Supportive of Newborn Male Circumcision: How They Counsel Parents.a,b

Abbreviation: OB/GYN, obstetrician/gynecologist.
a n = 940.
b DocStyles 2008. Those who answered the question “none of the above” were excluded.
Discussion
In 2008, approximately one-third of physician survey respondents were supportive of newborn male circumcision. Reasons were not asked, but the relatively low proportion may reflect, in part, subject to additional research, the general downward trend in circumcision of newborn males born in the United States, from 62.5% in 1999 to 56.9% in 2008. 11 Among physicians supportive of newborn male circumcision, nearly 72% said they would generally recommend the procedure when counseling parents about circumcising their infant son, in contrast to just 11% of the physicians who did not support newborn male circumcision. These results are particularly relevant because the 2012 AAP recommendations noted that physicians should explain the benefits and risks of male circumcision to parents in a nonbiased manner and help them understand the voluntary nature of the procedure. 20
Several factors were associated with physicians supportive of newborn male circumcision. Although there was no significant difference between pediatricians and OB/GYNs, the odds of reporting being supportive of newborn male circumcision were greater among family or general practitioners/internists than among OB/GYNs. The reason for this is not clear, especially given the results of a survey study that found 60% of family practice physicians perform 1 or more circumcisions per month, which is similar to the 70% rate reported for OBs, but higher than the 35% reported for pediatricians. 19 It is possible, however, that it may have to do with the broad-based training family physicians receive, including training in performing minor surgical procedures. Odds were also greater among physicians who saw mostly black or African American patients than those who saw mostly white patients. In the United States in an earlier study of male circumcision, among uncircumcised men, the odds of being likely or very likely to get circumcised if their health care provider told them it would reduce their risk of becoming HIV infected were higher for black than white men. 24 It may be that African American men inquire about male circumcision from their physicians because of the disproportionate number of infections among African Americans. 25 Odds of being supportive of newborn male circumcision were less among female physicians than among male physicians. A previous study reported that circumcisions are more commonly performed by male physicians 19 ; having less experience with male circumcision may be one reason why female physicians were less supportive of the procedure. Physicians in an individual and group practice had lower odds of being supportive of newborn male circumcision than physicians in a hospital setting. It may be that physicians working in a hospital setting are more comfortable with and accepting of surgical procedures like circumcision of newborn males than physicians not in a hospital setting 26 and in addition, the discussion about circumcision may be more routine in the hospital setting just after the birth than in the clinic setting.
There were several potential limitations to our study. First, the opt-in sampling frame may not be representative and may have resulted in a voluntary response bias where the persons who choose to participate have strong opinions about medical topics. Second, the response rate was low so there may be selection bias. However, the nonresponse weights that were applied in the analysis sought to reduce bias by attempting to have the respondents reflect the composition of physicians in the AMA master file. Third, a survey quota sampling technique was used, not a probability sampling technique, thus physicians in each specialty may not be representative. Fourth, it is likely that not all relevant variables were measured (eg, male physician circumcision status and circumcision status of son). Finally, since the survey questions were self-reported, this may have resulted in an over- or underestimation of the percentage of physicians who were supportive of newborn male circumcision. However, the strength of the study is that the overall sample of physicians is generally comparable to the AMA master file in terms of gender, age, and region.
In conclusion, our study showed that just one-third of physicians were supportive of newborn male circumcision and still fewer would recommend it to parents of newborn sons (31.1%). Although it seems that familiarity with the African clinical trial results might be a reason for the support, 27 it is of note that this variable was not significantly associated with the group of physicians supportive of newborn male circumcision. Not surprisingly, physician support for newborn male circumcision appears to translate into positive recommendations to parents of newborn sons (72%). This is in contrast to physicians not supportive of the procedure, where only 11% recommended circumcision to parents of newborn sons. The majority (60%) of the physicians not supportive of the procedure reported they would not offer an opinion. It may be that in physicians’ lack of recommendations to parents, an unspoken message is relayed that circumcision may not be the best choice. This is important because while parents by and large make their decision about circumcising their newborn sons based on factors such as social norms and the father’s circumcision status,12–15 parents also often rely on physicians as a source of information in making decisions about their child’s health care. 18 This result has implications for the 2012 AAP recommendations that noted that physicians should explain the benefits and risks of male circumcision to parents in a nonbiased manner. 20 Tobian and Gray 28 assert that Medicaid and other health insurance carriers should cover male circumcision costs for parents who choose to circumcise their sons. Once there is an equal opportunity for all parents to have their sons undergo the circumcision procedure if they choose, monitoring the perspectives of physicians regarding newborn male circumcision in the future may be one useful means to understanding the uptake of this procedure among parents.
Footnotes
Acknowledgments
We would like to thank Adam Burns and Deanne Weber for their assistance with question development and Charley LeBaron for comments on an earlier version of this article.
Authors’ Note
Sources of Support: Division of HIV/AIDS Prevention, CDC. Human Subjects: Styles surveys conducted by Porter Novelli are considered exempt research in accordance with criteria outlined in 45 CFR 46.101(b)(2). The findings and conclusions in this report are those of the authors and do not necessarily represent the views of the Centers for Disease Control and Prevention.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.