
Abstract
We describe the rate of death and identify the determinants of survival in a cohort of adults starting antiretroviral therapy (ART) in 2 hospitals in Upper West Region, Ghana. Kaplan-Meier model was used to estimate the survival probability after ART initiation and Cox proportional hazard model used to assess the relationship between baseline variables and mortality. A total of 91 clients who were initiated on ART in both hospitals participated in the study. Clients staged in the World Health Organization (WHO) clinical stage III/IV had a higher risk of mortality than those staging I/II (hazard ratio [HR] of 3.93). Hemoglobin value at baseline with a cutoff ≥12 g/dL for women (and ≥13 for men) was strongly associated with mortality in participants with an HR of 3.87 (95% confidence interval [CI]: 0.71-21.19) for severe anemia, 2.11 (95% CI: 0.45-9.93) for moderate anemia, and 0.88 (95% CI: 0.16-4.82) for mild anemia. Anemia and WHO staging were independent predictors of mortality.
Introduction
The provision of antiretroviral therapy (ART) in the public health care system in Ghana started in June 2003 at 2 pilot sites in the Manya Krobo district. This was part of a comprehensive care package that also included the provision of counseling and testing and prevention of mother-to-child transmission (CT/PMTCT), and management of sexually transmitted infections and opportunistic infections (OIs). 1
Available reference shows that the prevalence rate in Upper West Region (U/W/R) in 2011 is 1.0, which is the same as that in Jirapa district. 2
The available evidence regarding the survival outcomes in ART services in the Jirapa and Lawra districts of U/W/R in Ghana is limited. However, no study has focused on the survival outcome after the initiation of ART services.
Jirapa and Lawra districts are part of the 11 administrative districts in the U/W/R. Lawra district shares boundaries with Jirapa district in the east. In 2013, Lawra district had a population of 50 703, while Jirapa district had 93 537. 3
Subsistence farming, which is the main economic activity undertaken by the inhabitants, accounts for 80% of the district’s economy. Livestock rearing is also considerably engaged by most farmers.
The 2 referral district hospitals in Jirapa and Lawra of the U/W/R were used for this study. Both the hospitals have been providing HIV testing and counseling (HTC) services formally known as voluntary counseling and testing (VCT) and PMTCT for more than 5 years, and a free ART service was started in January 2008.
Clients who tested HIV positive at different service outlets in the hospitals, or who had been referred from elsewhere, are enrolled in HIV care. The clinical services are provided by an ART team comprising a doctor, a nurse, a pharmacist, biomedical scientist, and a data manager. Initial evaluation includes clinical and CD4 staging, which determines whether ART should be initiated. Treatment may also be initiated with clinical parameters alone when the CD4 test is not available. In addition to the medical eligibility, patient adherence and commitment are mandatory. The medical eligibility criterion for ART in the Ghana context is enforced. 1
The role of ART in reducing mortality and preventing OIs is a well-studied and established phenomenon in the Western world. In poor countries, especially sub-Saharan Africa where ART services have been initiated just recently, limited data exist on specific treatment results and recommendations in carrying out such interventions. As a result, the guidelines for implementation of ART include adopting experience from the Western world. The specific nature of disease demographics in resource-poor settings, especially high prevalence of tuberculosis, hepatitis B viral infection, malnutrition, and other bacterial infection, would affect the nature of response to treatment and ultimately changes in survival.
There is limited information regarding treatment outcome and ultimate impact of ART on patient survival in Ghana, in particular Jirapa and Lawra. A couple of studies have been conducted regarding the impact of ART and mortality.
This study assesses the factors that determine the survival of HIV patients undergoing ART in 2 referral hospitals, Jirapa and Lawra in U/W/R of Ghana. Further, a comparative analysis of the estimated survival functions between Jirapa and Lawra was done.
Initiation Criteria for ART
Antiretroviral therapy clinical services are provided by an ART team comprising a doctor, a nurse, a pharmacist, biomedical scientist, and a data manager. Initial evaluation includes clinical and CD4 staging, which determines whether ART should be initiated. Treatment may also be initiated with clinical parameters alone when the CD4 test is not available. In addition to the medical eligibility, patient adherence and commitment are mandatory. The medical eligibility criterion for ART in the Ghana context is as follows.
Antiretroviral therapy may be initiated when patients, including HIV-positive pregnant women, satisfy the following criteria: Patients with CD4 count less than 350 cells/mm3; and/or symptomatic with HIV infection in World Health Organization (WHO) clinical stage III and IV.
Although initiation is based solely on the WHO clinical staging, the CD4 count must be done as soon as possible. For pregnant women, where the CD4 count is greater than 350, they shall be put on antiretroviral medication (ARV) prophylaxis starting from 14 weeks for the purpose of PMTCT. 1
Based on the 2010 ART guidelines of Ghana, the preferred first-line regimen for adults and adolescents comprises zidovudine (ZDV), combined with lamuvidine (3TC) and either efavirenez (EFV) or nevirapine (NVP), and depending on the patient’s clinical condition AZT is replaced with tenofovir (TDF). 1 Stavudine (d4T) was included in 2008 ART guidelines of Ghana.
Once the decision is made to initiate ART, the appropriate regimen of highly active antiretroviral therapy (HAART) will be started. Patients are given 2 weeks of ARV medication to determine the toxicity/tolerance or adherence problems. The subsequent appointment schedule depends on the condition of the patient but usually medications are dispensed for 1 month, and clients are advised to have a review after day 28 and appointments are extended for clients with better adherence to treatment and an improved clinical condition. Cotrimoxazole (CTX) prophylaxis therapy is also provided at the initial stage based on the guidelines.
During every visit, the clients are counseled. A CD4 test is repeated every 6 months, and clients showing signs of treatment failure or poor clinical response are referred to tertiary care for viral load tests and initiation of a second-line regimen. Liver enzyme tests are also performed when necessary.
The cost of care has been substantially subsidized by the government of Ghana to GH¢ 5 for a month’s supply of ARV drugs, OI drugs, laboratory and other investigations, and other services. 1
Methodology
This study considered the retrospective cohort study of HIV-positive adults who started ART in the 2 hospitals. A cohort from January 1, 2009, to December 31, 2009, with a 3-year period of follow-up from 2010 to 2012, was used for the analysis.
The entire cohort of HIV-positive native client who started ART at the 2 hospitals was studied. Review records show that 91 clients started ART in the 2 hospitals (46 and 45 clients from Jirapa and Lawra hospitals, respectively). Each client was given an identification number by the hospital, which was used to generate the necessary data.
Individuals were included in the analysis if they were HIV infected, were ≥13 years of age, and had received ART on at least 1 clinical visit. Patients starting treatment in other places, who had previous ART history, were excluded.
Sociodemographic characteristics and baseline and follow-up clinical and laboratory measurement information were extracted from the client’s register using NACP ART Adult Database version 3.4b software. The data were collected by the principal investigators at each hospital. The primary outcome is the hazard of dying. R 2.15.3 and SPSS (PASW Statistics) version 20 software were used for statistical analysis. The main outcome variable was death within the follow-up time.
The Kaplan-Meier model 4 was used to estimate the survival probability after ART initiation, and P values were used to compare the estimated survival curves for Jirapa and Lawra. The Cox proportional hazard model was used to assess the relationship between baseline variables and mortality. The predictor variables used in the analysis were sex, WHO clinical stage, and baseline hemoglobin. Variables that were statistically significant (P < .05) in the univariate analysis were subsequently fitted into the multivariate analysis.
Results
A total of 91 new clients were initiated on ART in both the hospitals during the study period. The cohort contributed to a total of 195.6 person-years of follow-up and a median follow-up of 36 months.
Demographic characteristics of the study clients are summarized in Table 1. About 37% of the clients were of age 25 to 34 and 35 to 44 years, 17.6% were 45 years or older and 7.7% were 24 years or younger at the time of treatment initiation. The median age of the clients at treatment initiation was 35 years (range, 17-60 years). The majority (59.3%) of the clients were females. In Jirapa hospital, 50.5% of the clients started treatment. About 58% of the clients were illiterate, while 40.7% of the clients had at least primary school education or more, and 1.1% did not respond to the education status. Of the study clients, 57% were married, 8.8% were single and divorced, 2.2% were separated and cohabiting, and 18.8% were widows or widowers at the time of the treatment initiation, and 1.1% did not response to the status of marriage.
Sociodemographic Characteristics of the Study Clients.

Clinical parameters of clients are summarized in Table 2. Of the study clients, 35% were in WHO stage II and III and 2% in WHO stage IV. Of the clients in Jirapa and Lawra hospitals, 65% and 35%, respectively, were clinically staged as III/IV. About 98% of the clients participating in the study started treatment with a CD4 count ≤350 cells/mm3 and 2% with a CD4 count >350 cells/mm3 and stage III/IV. Before treatment initiation, the median CD4 count of the clients was 161 cells/mm3 (range, 2-438 cells/mm3). Clients had a baseline hemoglobin ranging from 5.40 to 15.40 g/dL. In all, 50% of the clients had mild anemia (10-11.9 g/dL for women and 10-12.9 g/dL for men).
Clinical Characteristics of Clients on Initiation of ART.

Abbreviations: ART, antiretroviral therapy; NR, nonresponse; WHO, World Health Organization.
Descriptive Survival Analysis
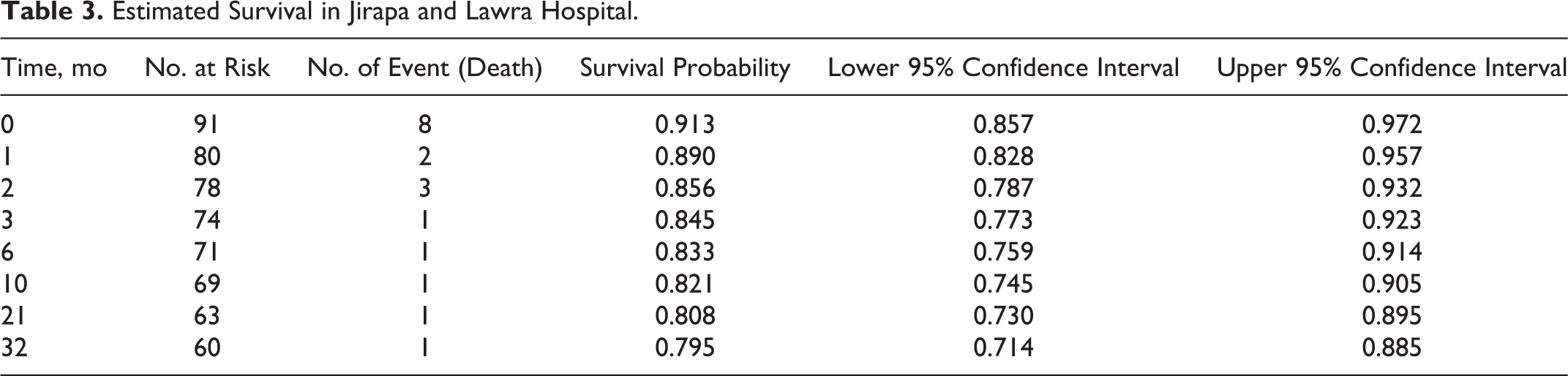
The median follow-up time was 36 months (range, 0-36 months). A total of 18 (19.8%) clients were reported dead. About 44.4% of the deaths occurred before the first month after the initiation of treatment. The remaining clients were censored for different reasons: 7 (7.7%) were lost to follow-up, 8 (8.8%) got transferred to other facilities, and 58 (63.7%) were alive at the end of the 36-month follow-up period. Estimated survival is shown in Table 3.
Estimated Survival in Jirapa and Lawra Hospital.
Graphical estimation of the overall Kaplan-Meier survival function showed that most of the deaths occurred in the earlier months of ART initiation, and it declined in the later months of follow-up. Separate graphs of the estimates of the Kaplan-Meier survival functions, for different factors, were also constructed in order to assess whether there is a difference in survival experience between different groups of individuals (see Figures 1 and 2).

Kaplan-Meier survival curves of client’s event (death).

Kaplan-Meier survival curve by facility.
A prognostic model based on the WHO clinical staging and hemoglobin level is predictive of mortality in this study. In the 36 months of follow-up, survival probability was significantly different between the groups with and without CTX. A statistically significant difference in survival probability was observed among WHO clinical stages, ranging from 0.96 for clinical stage I to 0.67 for clinical stage III, in the 36-month period. It is realized that clients in WHO stage I and II have higher survival probability. The hemoglobin level of clients before initiating ART was also considered during the study. About 16.5% of the clients had normal hemoglobin level, 38.5% mild anemia, 33% moderate anemia, and 12.1% severe anemia (see Figures 3 and 4).

Kaplan-Meier survival curves by cotrimoxazole initiation.

Kaplan-Meier survival curves by the World Health Organization clinical stage.
It is uncertain whether the association between anemia and mortality is causal or whether anemia is rather a marker of progressive HIV disease. It is known that the incidence of anemia increases with the progression of HIV infection (see Figure 5). 5
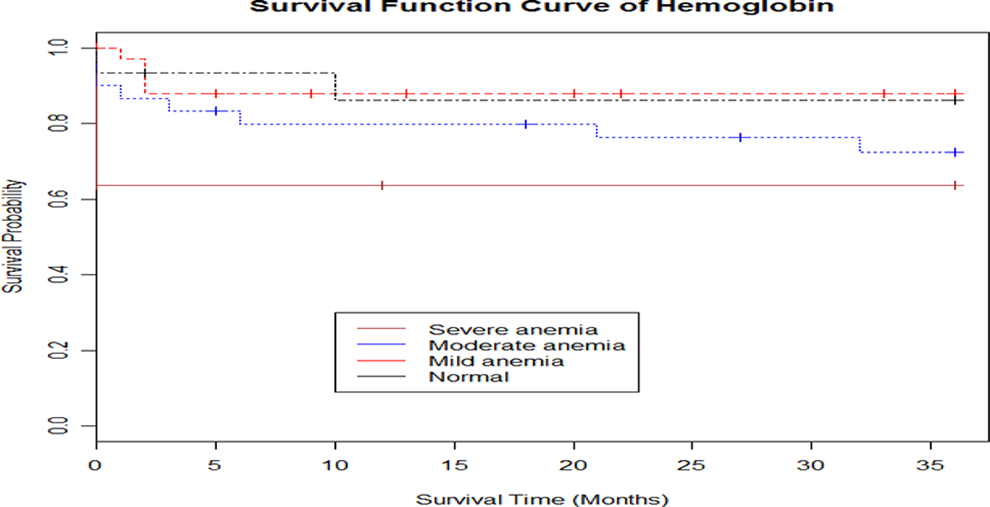
Kaplan-Meier survival curves according to baseline hemoglobin. Normal: >12 g/dL (>13 g/dL for men); mild anemia: 10 to 11.9 g/dL (10-12.9 g/dL for men); moderate anemia: 8 to 9.9 g/dL; severe anemia: <8 g/dL.
Cox Proportional Hazards Model
Table 4 presents the univariable models along with the necessary statistics. In a multivariable analysis, the variables WHO stage I/II, hemoglobin level at a cutoff point of ≥12 g/dL for women and ≥13 for men, clinical stage III/IV, and CTX initiation (at or before treatment initiation) were significantly associated with 36 months of survival. The hazard ratio (HR) of mortality for comparing WHO clinical stage of stage III/IV, which is one of the criteria for ART initiation, had almost 5 times higher risk of mortality than WHO stage I/II. Clients with severe anemia had 6 times higher risk of dying during the first year on ART than those with a normal hemoglobin level. The hazard rate of mortality reduces as the hemoglobin level increases. After ART initiation, the hemoglobin laboratory test should be performed on a regular basis as it would allow a more targeted search for OIs and closer follow-up in high-risk clients, thus reducing high mortality. We lacked viral load tests, which is an established predictor of morbidity and mortality in clients on ART (see Figure 6).

Cumulative hazard function curve of by World Health Organization clinical staging.
Hazard Ratios of Mortality According to Baseline Variables in HIV-Infected Patients Starting ART.

Abbreviations: ART, antiretroviral therapy; CI, confidence interval; HR, hazard ratio; WHO, World Health Organization.
Discussion
The cohort study was made up of a 36-month follow-up period after treatment initiation, of which most of the deaths (44.4%) occurred before the first month after initiation of treatment. The survival probability at the end of the follow-up period (36th month) was .79.5 (CI: 0.714-0.885). The causes of death were not investigated. Late access to ART services, stigma related to HIV, and limited availability of HIV HTC services in most areas in the past might have played a role in delayed diagnosis, thereby leading to mortality. Lack of proper screening of latent OI might as well have increased the mortality rate. In this study, 7.7% were lost to follow-up and were not traced. It could probably be explained by the fact that most of the lost cases in our context had been dead but were not reported due to poor patient tracing and reporting mechanisms.
Most studies established CD4 count as a predictor of mortality; 98% of the clients, overall, started ART with counts less than or equal to 350 cells/mm3. As indicated in a study at Korle-Bu Teaching Hospital, Ghana, Renner et al stated that a targeted approach based on predictors of CD4 count recovery can be a viable and cost-effective way of monitoring HAART in HIV-infected children in resource-limited settings. 6 In this study, it was also found that the probability of death continued to decrease with higher baseline CD4 counts. Clients who were in WHO clinical stage III/IV had a higher risk of mortality than those in stage I/II (HR of 3.93). In the absence of a CD4 reagent, the client should always be examined well to make use of his or her WHO clinical staging for early access to ART.
In one study, Owiredu et al concluded that HAART has the capability of reducing the incidence of anemia and lymphopenia, which are associated with disease progression and death in HIV-infected patients. 7 The hemoglobin of clients before they were initiated on ART was also considered during the study. Of the clients, 16.5% had a normal hemoglobin level and 38.5% had mild anemia, 33% had moderate anemia, and 12.1% had severe anemia. Hemoglobin value at baseline with a cutoff of ≥12 g/dL for women (and ≥13 for men) was strongly associated with mortality with HR of 3.87 (95% CI: 0.71-21.19) for severe anemia, 2.11 (95% CI: 0.45-9.93) for moderate anemia, and 0.88 (95% CI: 0.16-4.82) for mild anemia.
Conclusion
The Kaplan-Meier results showed that the general median estimated survival time of patients after HAART initiation is 36 months. The mortality rate was very high in the earlier months of ART initiation and tended to stabilize later. About 44.4% of the deaths occurred before the first month of ART initiation. The results of the multivariable Cox proportional hazards model showed that WHO clinical stage III/IV and severe anemia were indicative of a higher risk of mortality. Mortality was low, with the majority of deaths occurring within 3 months of starting ART. Anemia and WHO staging were independent predictors of mortality.
Clients on ART should have more frequent (2 weeks) contacts with ART centers during the early phase (3 months) of treatment in order to prevent the many deaths that occur during the early weeks of ART. The factors that cause increased rate of mortality in the early stages of ART initiation need to be explored. WHO clinical stage, very low CD4 count, and hemoglobin level are indicators of the progression of the disease. Identification and treatment of OI may reduce the risk of mortality. Attempts should be made to input information on the investigation of the causes of deaths in the NACP Adult and Pediatric database. Mechanisms should be developed at each ART center to trace clients lost to follow-up. All HIV positive clients should be given ART treatment regardless of the CD4 count level or WHO clinical staging.
The limitation of this study is funding. Time is another limitation factor as we would prefer to study the survival of adults on ART in the Upper West Region of Ghana.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.