
Abstract
Background:
Falls is a common geriatric syndrome that has not been well characterized in HIV-infected populations.
Methods:
We retrospectively reviewed our database and identified patients who fell over the last 12 months.
Results:
Thirty-two patients were identified (incidence rate of 16 × 1000 patients per year). Twenty-five percent were female and 75% male. Sixty-seven percent were African American with 33% Caucasians. Average age was 48.19, number of years with HIV infection on average was 9.38 years, mean CD4 count 347.2 cell/mm3, mean HIV viral load was 31 379 copies/mL. The average number of medications was 8.7 with a mean of 3.48 comorbidities. The mean vitamin D level was 27.20. Sixty-two percent of patients were compliant with antiretroviral therapy. Univariate and multivariate analysis showed that number of medications (< .005 medications; P < .005), more than 3 comorbidities (P < .005), and noncompliance (P < .001) were related to falls in this population.
Conclusion:
Falls is a common geriatric syndrome. Associated risk factors in our cohort included number of medications, more than 3 comorbidities, and noncompliance. Larger studies are needed to properly characterize this geriatric syndrome in HIV-infected patients. As HIV-infected populations age, a shift into a more comprehensive geriatrics care including fall risk evaluation may be needed.
Introduction
Antiretroviral therapy (ART) has changed survival in HIV-infected populations. Greater improvements in outcomes and a higher prevalence of non-AIDS-defining complications developed as a result of ART. As HIV-infected patients age, higher prevalence of geriatric syndromes and geriatric conditions is expected. Approximately 30% of people over 65 years tend to fall each year, and up to 50% of these falls are recurrent. Falls result in increased morbidity, hospital costs, and worse mortality outcomes for elderly patients1–7
Fall is a common geriatric syndrome that has not been well characterized in HIV-infected populations until recently. Fall risk increases as patients’ age, and non HIV-infected populations have been related to the presence of multiple comorbidities, polypharmacy, and functional impairment. 8
Some reports have showed the multiplicity of comorbid conditions affecting HIV-infected patients. 9 Inadequate functional performance including poor lower limb muscle performance has been reported in HIV positive patients. 10 Equally interesting is the impact of nutrition on functional performance and risk of falls. This relationship has been clearly established in the case of poor nutritional status and the development of sarcopenia. 8 Therefore, based on the above-mentioned factors, HIV-infected populations may be at a higher risk of falls. Moreover, hearing and visual problems have been directly correlated to falls in senior populations. The role of these 2 factors in HIV-infected patients has not been established. 11
One recent study has evaluated fall risks between HIV and non-HIV infected populations. This study mentions the fact that the fall risk of middle aged (45-55 years) HIV-positive individuals is similar to non-HIV infected patients >65 years. 9 This finding coupled with interesting reports indicating a “premature aging” in HIV-infected individuals may pose this population at a higher risk of complications associated with falls, including fractures, recurrent hospitalizations, and potentially decreased quality of life. 9
This article reports the experience of an academic, urban HIV clinic and explores the incidence and risk factors associated with falls in HIV-positive patients.
Methods
We retrospectively reviewed our database and identified patients who fell over the last 12 months. Our HIV clinic has a total of 2000 registered patients. Demographic, clinical, and laboratory information was abstracted. Institutional review board approval from the Louisiana State University Health Sciences Center in New Orleans was obtained. Demographic information included age, gender, ethnic background, years with HIV infection, comorbidities, number of medications, number of comorbidities, and compliance with ART. Laboratory information included CD4 counts, HIV viral loads, and vitamin D levels.
Fall was defined as a situation where patients landed in the ground without accidental intervention. Ratios and percentages were analyzed. Univariate and multivariate analyses were performed.
Results
A total of 32 patients were identified (incidence rate of 16 × 1000 patients per year). Of all the patients, 25% were female and 75% were male, while 67% were African American with 33% Caucasians. Average age was 48.19 years; number of years with HIV infection in average was 9.38 years, mean CD4 count was 347.2 cell/mm3, and mean HIV viral load was 31 379 copies/mL. The whole group had an average number of medications of 8.7, including antiretroviral (ARV) medications, with a mean of 3.48 comorbidities. The mean vitamin D level was 27.20. Of all the patients, 62% were compliant with ART. Subsequently, for further analysis, the total number of patients was stratified into young (<50 years of age) and senior (>50 years of age). Table 1 depicts the information of demographics in this population.
Characteristics of HIV-Infected Patients with Falls.
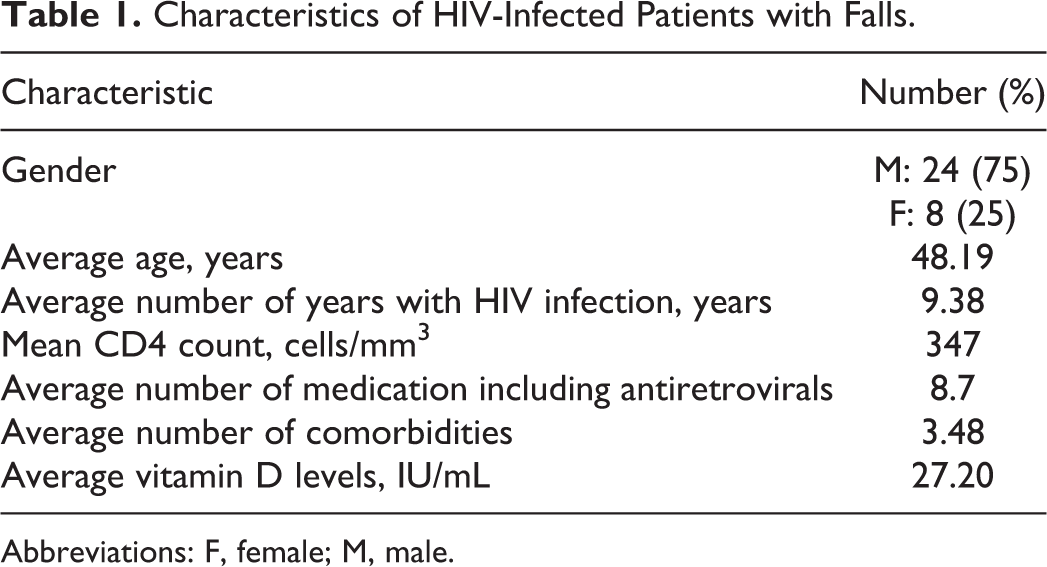
Abbreviations: F, female; M, male.
Approximately, 55% of patients were >50 years and categorized as senior patients. This group had an average age of 54.8 years. The mean CD4 count was 384 cells/mm3 with a mean HIV viral load of 1 132 588 copies/mL. The average number of year with HIV infection in this subgroup was 9.18 years, with an average of 10 medications per patient. Their average number of comorbidities was 3.75, and 67% of this group was compliant with their medications. Interestingly, the mean vitamin D level was 27.04 units/mL. Table 2 summarizes the information of this group.
Patients of >50 Years of Age Group.

Abbreviations: F, female; M, male.
The young group (<50 years) had an average of 40 years of age, an average of 9.6 years with HIV infection, CD4 count of 316 cells/mm3, and HIV polymerase chain reaction (PCR) RNA viral load of 58 434 copies/mL. The average number of medications was 6.8, including ARVs, and they had a mean of 3.78 comorbidities. Interestingly, their vitamin D level was higher compared to the senior group (27.15 units/mL). Table 3 shows information about this group.
Patients of <50 Years of Age Group.
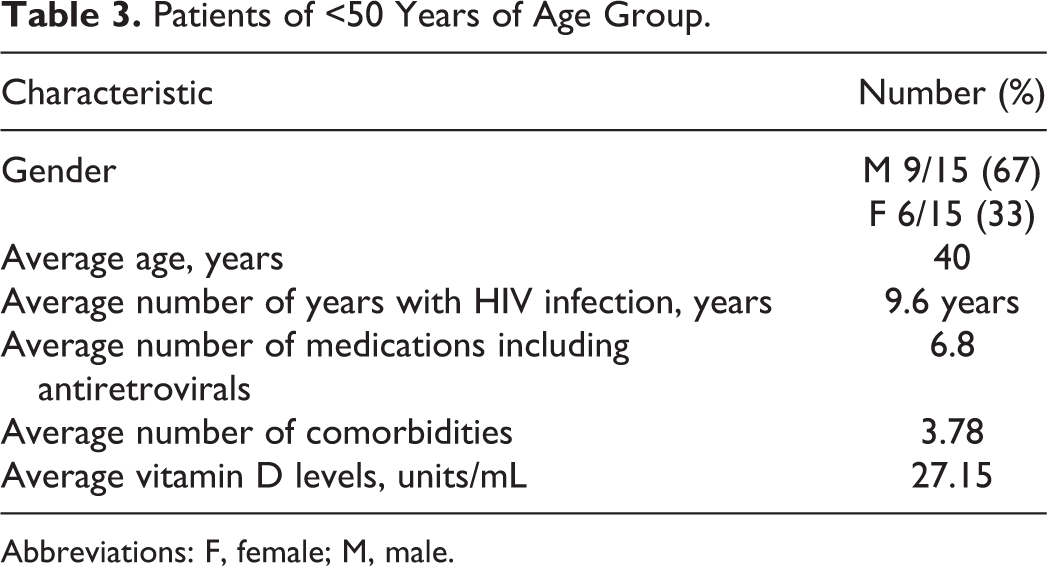
Abbreviations: F, female; M, male.
In multivariate analysis, polipharmacy (defined as more than 5 medications besides ARVs) was found to be significantly different between the senior and young groups. Further statistical analysis revealed that number of medications (>5 medications; P < .005), more than 3 comorbidities (P < .005), and noncompliance with medications (P < .001) were related to falls in the whole population.
Discussion
Fall is a very common geriatric syndrome, and its incidence increases with age. In case of HIV-infected patients, this is complicated by the presence of other factors including HIV virus, comorbidities, polypharmacy, and poor functional status. 8,9
Our study points out interesting facts. First, the prevalence of falls as expected is higher in the senior patient group compared to the young group. Second, the senior group uses more medications maybe due to a higher number of other factors but comorbidities. Interestingly, the number of comorbidities was higher for the young group. Third, there were no significant differences among variables such as CD4 count, HIV PCR viral load, and vitamin D levels between these 2 groups. Compliance with ARV appears to be higher in senior populations even though potential drug–drug interactions may happen as a result of multiple comorbidities in the senior population. This has been described previously. 12
Poor lower extremity function was not evaluated, since it was not included in the electronic information. This would have improved the analysis of correlation between lower extremity functionality and risk of falls. Other tests such as get up and go test were not part of the evaluation either since this is not a common test administered in the HIV setting. The correlation among these 2 variables and fall risk needs to be studied. We did not find any information on hearing or visual issues in this population. Therefore, correlations between these variables and risk fall could not be determined.
Frailty status has been linked to many increased morbidity and mortality in senior and HIV-infected patients. 13 Interestingly, even though the study was not designed to evaluate for frailty, patients who had falls and were included in the study did not appear to have signs of frailty (exhaustion, tiredness, slowness, muscle loss, and decreased strength). 13 Therefore, traditional fall risk factors other than frailty status should be sought and investigated in this population.
The issue of vitamin D deficiency and its role on muscle metabolism, etiology of muscle weakness, and increased risk of falls have been studied widely. 14 –18 In this study, the difference of vitamin D levels between young and senior groups did not appear significant (27.15 versus 27.04 units/mL). One of the factors for this apparent lack of statistical difference might be the small number of patients. Another possible explanation might be the lack of accurate information for all the patients in relation to vitamin D levels.
Polypharmacy is a widely known fall risk factor. 19,20 In our study, the number of medications was higher for senior patients, and this difference was significant when compared to the young group. Interestingly, the type of ART did not have a particular effect on fall risk. The type of medication used has also been related to fall risk. 19 In particular, certain families of drugs, such as benzodiazepines, antihypertensives, hypnotics, and among others, have been found to directly correlate with falls. 20 In our group, we did not find any significant differences among the type of medication and its particular fall risk, when these drugs were analyzed.
Noncompliance with medications is a particular problem among HIV-infected populations. 21 In our study, we found that noncompliance was directly correlated with fall risk. Possible explanations may be drug and substance abuse, which may put these patients to a higher risk of falls, mediation interactions, or side effects that prevented patients to continue taking their medications, possible immune system deterioration, which in turn may predispose patients to develop further complications including falls.
The role of CD4 count in risk fall has been evaluated. Studies showed no correlation between nadir CD4 count and fall risk. 8 Interestingly, in our study, both the senior and the young groups had relatively high CD4 counts; therefore, we could not find any correlations between this variable and falls in our population. Moreover, the role of HIV PCR viral load could not be established in our study since both the groups have relatively high-HIV PCR viral loads.
Limitations of this study include its retrospective nature, potential underreporting among providers, and the small size of patients in the study. Results found in the study may not be applicable to other populations.
Conclusion
Fall is a common geriatric syndrome. The associated statistically significant risk factors in our study included number of medications, more than 3 comorbidities, and noncompliance with medications. Larger studies are needed to properly characterize this geriatric syndrome in HIV-infected patients. As HIV-infected populations age, a shift into a more comprehensive geriatrics care including fall risk evaluation may be needed.
Footnotes
Authors’ Note
This manuscript has not appeared as a preliminary report or abstract.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.