
Abstract
Goals of universal “test and treat” will never be fully realized if testing acceptance remains low, including rural areas, where HIV is increasingly recognized. We surveyed 250 randomly selected households from a rural Ethiopian town (Arba Minch) and surrounding villages about HIV testing experience, knowledge, and attitudes. Of the 558 adults, 45% were never HIV tested. Those never tested for HIV were more likely to be (P < .05) ≥45 years, rural villagers, and unaware of the benefits of antiretroviral therapy treatment and that persons with HIV can appear healthy; they were more likely to believe HIV-infected persons would be stigmatized and unsupported by their communities. Of those never tested, 70% were interested in HIV testing if offered. Despite recommendations that all persons be HIV tested, almost half of the adult residents in this rural community were never tested. Programs to increase HIV testing must include measures to address stigma/discrimination and knowledge deficits including benefits of early diagnosis and treatment.
Introduction
From a largely urban problem, HIV is increasingly being recognized in rural areas. Although seroprevalence may be higher in cities, the majority of persons in sub-Saharan Africa (SSA; 63%) still live in rural areas. 1 Of the estimated 1.2 million people living with HIV (PLWH) in Ethiopia (where 83% of the population is rural), over 450 000 (38%) PLWH live in rural areas. 2 Compared to those in urban areas, rural populations may have lower HIV knowledge and awareness levels as well as particular difficulty accessing HIV testing and care programs. 3 –7 Although HIV incidence rates may be stabilizing or even decreasing in urban areas in SSA, rates in many rural areas are continuing to increase. Available data from Ethiopia suggest that HIV prevalence may be increasing in small market towns compared to larger cities, of great concern since such towns can serve as bridging sites for urban to rural spread of HIV. 8
Lack of knowledge of serostatus by PLWH is a major obstacle to the goal of universal access to treatment and prevention, including the rural areas. Although provider-initiated HIV testing is one strategy to improve HIV testing, 9 many clinical settings in generalized epidemics are not routinely offering testing, 10 and patients who are asymptomatic may not present to health care facilities. As treatment guidelines are increasingly recommending earlier initiation of antiretroviral therapy (ART) to prevent morbidity and mortality, 11,12 and with current evidence of the advantage of “test and treat” to prevent HIV transmission, 13,14 HIV testing offered in community settings remains critically important, especially to reach those in earlier stages of HIV infection. Strategies used to help promote HIV testing in such settings include community mobilization, home-based testing, mobile voluntary counseling and testing services, and mass testing campaigns. 15 –17 However, increasing access to HIV testing, although essential, will not be successful unless increased access is accompanied by increased acceptance of testing. If certain knowledge gaps or negative attitudes are associated with failure to receive HIV tests, programs designed to improve testing rates must address these needs.
In preparation for a community support program for PLWH in rural southern Ethiopia, we conducted an HIV knowledge and attitude survey among randomly selected households, focusing on neighborhoods and villages from which a larger number of PLWH had been reported. 18 As part of this survey, we asked whether respondents had been tested for HIV, desired to receive an HIV test, and knew where HIV testing could be obtained. We report responses to these questions and the relationship of having ever been tested for HIV with specific knowledge gaps and negative attitudes toward PLWH, and discuss how these barriers can be addressed.
Methods
Study Setting
This survey was conducted among residents of the rural southern Ethiopian town of Arba Minch as well as surrounding villages, where most people support themselves through farming; details have been previously described. 18 As of February 2010, 2886 patients enrolled in HIV care at Arba Minch Hospital, the main zonal referral hospital, and 1849 started on ART, 19 indicating the significant presence of HIV in this community.
Participants for this survey were selected based upon their kebele of residence. In Ethiopia, kebeles are small units of administration, representing villages or neighborhoods, which provide many basic municipal services and to which every resident of Ethiopia belongs. In all, 4 kebeles were selected from neighborhoods within Arba Minch town and 6 kebeles from villages outside the town. 18 The main criterion for kebele selection was prior knowledge based on information from HIV clinics and local PLWH associations that there were significant numbers of PLWH living in that kebele. From each kebele, we identified a list of all households (mean number of households = 532 in town kebeles and 704 in village kebeles), and 25 households were randomly selected. Trained interviewers visited each selected household and asked whether they could privately interview all adult (≥18 years) household members. Of the 638 adult residents meeting inclusion criteria in identified households, 47 (7%) were unavailable (eg, moved away for school/work); of the remainder, 95% agreed for the interview.
Surveys were verbally conducted in Amharic and included questions about previous HIV testing history, interest in receiving an HIV test, and knowing where HIV testing could be obtained. Other survey items included demographic characteristics, knowledge questions about HIV transmission and treatment, and asking about agreement with certain negative or positive attitudes toward PLWH. We evaluated the association between self-report of ever receiving an HIV test and demographic characteristics, responses to 14 knowledge questions, and responses to 9 statements about attitudes toward PLWH.
This study was approved by the institutional review boards of University of Hawassa and University of Minnesota. Participants provided informed consent. The project was presented to kebele leaders who provided their support.
Results
Study Participants
Of the 558 participants reporting their HIV testing history, 53% were female, 65% were from rural villages, and 35% were from town neighborhoods. The median age was 30 years (interquartile range [IQR] = 22, 45), 62% were married, and 32% were single (remainder were widowed or separated). In terms of education, 49% either never attended school or attended some primary school but had not completed it.
HIV Testing History
A total of 306 (55%) respondents reported being tested for HIV at least once, including 238 (43%) tested within the previous 16 months. Of those tested, 17 (6%) reported a positive result. Although 411 (74%) knew where HIV testing was available if they wanted it, 26% did not. Of those never tested for HIV, 70% indicated that they would be interested in receiving an HIV test if offered one.
A history of HIV testing was reported by 56% of the males and 54% of the females (P > .10); 55% of those ≤21 years of age, 65% of those 22 to 44 years, and 36% of those ≥45 years (P < .001); 70% of those who had finished at least primary school versus 40% who had not (P < .001); and 75% of those living in Arba Minch town neighborhoods versus 44% from rural villages (P < .001).
Knowledge Associated with HIV Testing
Those never tested for HIV were less likely to know that someone with HIV can appear healthy, that treatment helps prolong the life of PLWH, that condoms are protective, and that there are ways to reduce mother-to-child HIV transmission; they were more likely to believe in casual contact transmission (Table 1). When asked whether they felt they had enough information about HIV/AIDS, 54% said “no.” Testing was reported by 70% of those who felt they had enough information about HIV/AIDS versus 43% of those who felt they did not (P < .001).
History of Ever Receiving an HIV Test by Responses to Knowledge Questions, Community Residents of Kebeles, Arba Minch, Ethiopia.

Abbreviation: DK, don't know.
HIV Stigma Associated with HIV Testing
Those never tested for HIV were more likely to agree with attitudes of blame or shame toward PLWH and believe PLWH would be distanced or stigmatized by their communities (Table 2). Those who agreed that communities should respond to PLWH with compassion and support were more likely to have been HIV tested. HIV testing was reported by 61% of those who personally knew a PLWH, compared to 45% of those who did not (P < .001).
Discussion
Universal voluntary HIV testing and immediate ART have been suggested to have a major effect on severe generalized HIV epidemics, including in SSA. 20,21 Contingent on the success of such strategies is the widespread acceptance of HIV testing, especially in earlier stages of HIV infection. In our community survey of randomly sampled households in rural Ethiopia, almost half (45%) of the respondents were never tested for HIV, including 56% of those from rural villages. Given that small towns are becoming “hot spots” for HIV in Ethiopia, with potential further spread to rural settings, 8,22 it is essential to develop programs targeted to such communities.
Ethiopia’s strategic HIV/AIDS plan has as a priority enhanced uptake of HIV counseling and testing, including in community-based settings. 22 From 2005 to 2008, the number of Ethiopians tested for HIV each year increased 10-fold. 23 Despite this impressive progress, gaps in HIV testing remain. In addition to those never tested, many Ethiopian PLWH who learn their status and enter care do so only after developing advanced HIV disease with low CD4 counts. 24,25
In addition to lower testing rates in rural villages, we also identified lower testing in those ≥45 years of age. Our results are consistent with other studies from SSA that older persons are less likely to accept HIV testing. 26 –28 HIV in older adults, including in SSA, is being increasingly recognized, 29 stressing the need to ensure that older adults are adequately accessed by HIV counseling and testing programs.
Our results suggest that programs to promote HIV testing and counseling need to address certain knowledge gaps. In our survey, those never tested were less likely to know that one can be HIV infected and still feel healthy without symptoms. Those never tested were also less likely to know that treatments such as ART prolong the life of PLWH. Programs to increase the uptake of HIV testing therefore need to inform participants in a culturally and educationally appropriate fashion about the natural history of HIV and benefits of early diagnosis and treatment. Other SSA studies have also found that ART availability and belief in its benefits can have a positive impact on willingness to be tested for HIV. 30,31
Although knowledge is essential, our results also suggest that failure to test for HIV was associated with the belief that PLWH would be rejected or distanced by their families or communities. Conversely, those who felt PLWH should be treated with community compassion and support were more likely to be tested. Failure to test for HIV because of feared or perceived stigma has been identified in other SSA studies. 26,32 –34 Programs to encourage universal HIV testing will therefore never be totally successful unless they also address community-based HIV stigma. Since in our survey mistaken beliefs in casual contact transmission were associated with failure to test, addressing such stigma-associated misperceptions is essential. A variety of other strategies to reduce stigma have been employed including community dialog (such as the Ethiopian community conversations program), integrating HIV testing with other health promotion interventions, involvement of religious and other opinion leaders, and inclusion of PLWH in implementing stigma reduction efforts. 8,35 –38 In our survey, those who personally knew a PLWH were more likely to have accepted HIV testing.
Several cautions must be considered in interpreting and generalizing our results. Some participants may have given responses they considered socially desirable, rather than how they actually felt; to minimize this potential bias, interviewers were trained to ask questions in a nonjudgmental fashion. Second, this survey was designed to assess responses in a rural Ethiopian community, and responses may differ in different geographic and demographic settings. However, as described above, our key findings are consistent with studies from many other SSA countries. Third, although we looked at individual knowledge and attitude as predictors of HIV testing, various structural factors may affect community testing rates such as accessibility of testing services and distance to clinics. However, even if strategies are promoted to reduce such structural barriers, the individual knowledge and attitude factors we identified are also important to address to help improve client acceptance. Finally, our primary outcome of analysis was being ever tested for HIV; in certain high-risk populations, repeat testing is advisable. 39
In summary, despite recommendations that all persons should be HIV tested, our study of rural kebeles in which there were many PLWH found that almost half of the adult residents were never tested. Outreach campaigns to improve testing must include both educational components and community HIV stigma and discrimination reduction efforts. Even if access to HIV testing is increased, unless uptake can be improved, the goal of universal test and treat will never be realized.
History of Ever Receiving an HIV Test by Agreement with Attitudes Toward PLWH, Community Residents of Kebeles, Arba Minch, Ethiopia.
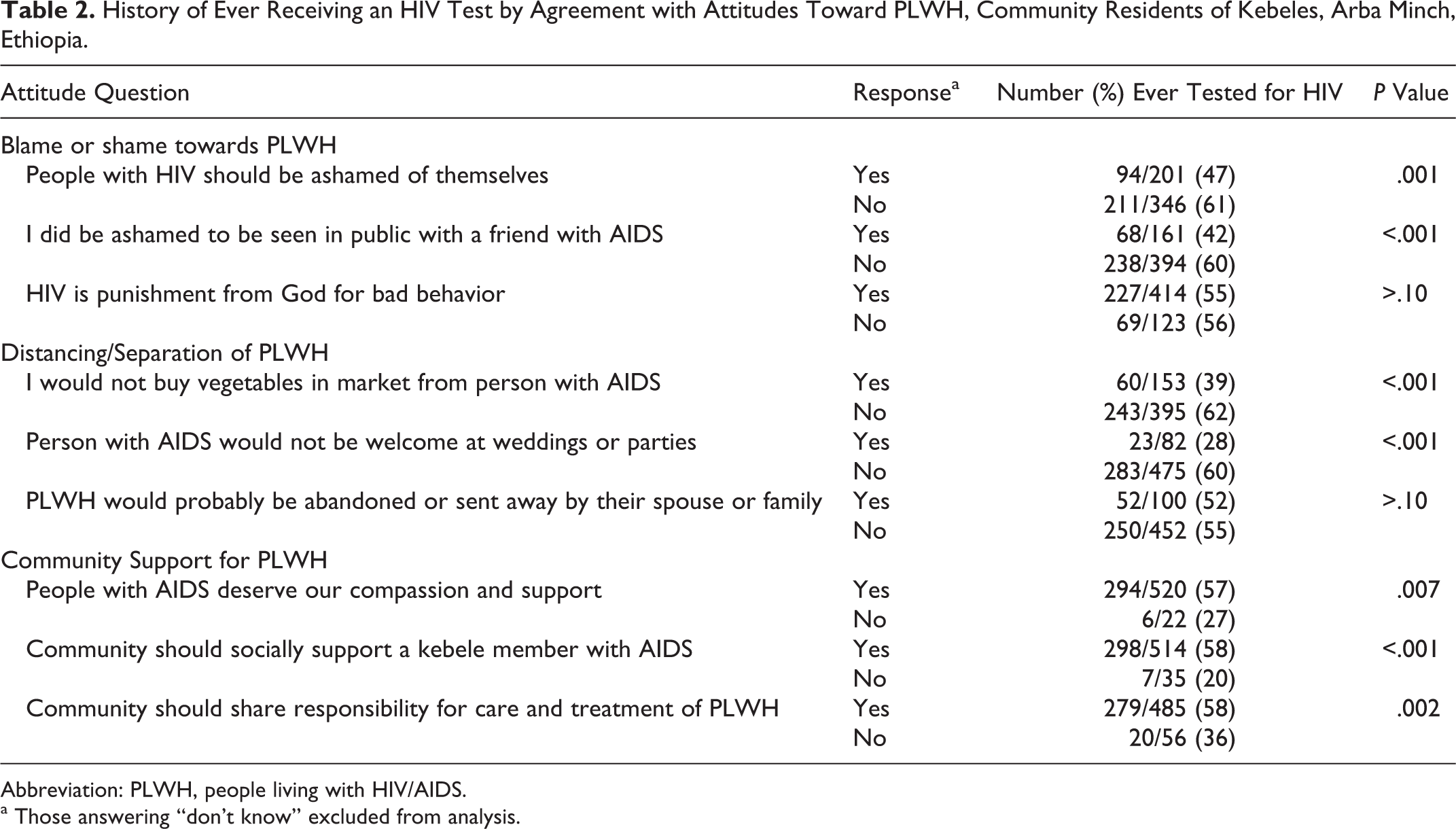
Abbreviation: PLWH, people living with HIV/AIDS.
a Those answering “don't know” excluded from analysis.
Footnotes
Acknowledgments
We wish to thank the following individuals and organizations who provided technical advice, support, or assistance: Dr Akram Eltom and the HIV/AIDS team from the World Health Organization's Country Office for Ethiopia; Meka Metekia and Kare Chawecha from the Regional Health Bureau, Southern Nations, Nationalities, and People's Regional State; the Gamo Gofa Zonal Department; Arba Minch Hospital; the Arba Minch zuria woreda health office; the Arba Minch town health office; the Arba Minch Health Center; and Gezie Aba from the Ethiopian Office of the National Alliance for State and Territorial AIDS Directors. We also wish to thank all data collectors and supervisors for their commitment and conscientious efforts in conducting these surveys. We thank Rose Hilk for her invaluable assistance with programming and data management and Alex Baker and Nick Meza for data entry. Finally, we wish to thank and extend our appreciation to the Arba Minch zuria woreda and Arba Minch town community at large for their important and generous participation as a study population.
Authors’ Note
Preliminary results from this study were presented at the 16th International Conference on AIDS and STIs in Africa in Addis Ababa, Ethiopia during December 2011.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) declared receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this project was provided by the World Health Organization's Country Office for Ethiopia and the University of Minnesota's Office for International Programs.