
Abstract
Background:
With transmission of HIV occurring mainly through heterosexual contact, it is paramount to identify serodiscordant couples and implement preventive strategies that will protect the negative partner. The burden of serodiscordance and its predictors in Ethiopia is not clearly understood due to the dearth of data.
Objective:
To assess the prevalence and predictors of HIV serodiscordance among couples tested in Jimma University Specialized Hospital (JUSH) Voluntary Counseling and Testing (VCT) center.
Methods:
The study employed a case–control study design conducted at VCT center of JUSH in all registered serodiscordant couples and seroconcordant couples that were selected from the registered clients in the period from 2003 to 2010. A pretested structured questionnaire was used for data collection using medical chart abstraction. Data were entered, cleaned, and coded using Statistical Package of Social Sciences (SPSS) version 16.
Results:
The prevalence of serodiscordance in the study population was found to be 8.4%. Male and female discordants accounted for 5.8% (137) and 2.6% (62), respectively. Rare use of condom (adjusted odds ratio [AOR] = 7.2; 95% confidence interval [CI] = 1.59-32.54) and active tuberculosis (TB) at enrollment (AOR= 17.7; 95% CI = 2.3-139.2) were significantly found to be the predictors of serodiscordance.
Conclusion:
The prevalence of serodiscordance in the study area was found to be low, but it contributes to a clinically significant population that mandates implementation of preventive strategy. Sero-positive individuals who use condoms rarely should be encouraged to have their partners tested, and the association between active TB and serodiscordance underscores the need for further study.
Keywords
Introduction
In 2009, there were an estimated 33.3 million (31.4-35.3 million) people living with HIV and 2.6 million (2.3-2.8 million) people who became newly infected with HIV worldwide. 1 In sub-Saharan Africa, where the majority of new HIV infections continue to occur, an estimated 1.8 million (1.6-2.0 million) people became infected in 2009. 1 Sub-Saharan Africa continues to have the largest number of people living with HIV, many of whom are in HIV-discordant relationships. 2 Recent study suggests that a large proportion of new HIV infections in countries with mature epidemics occur within discordant partnerships, making discordance a major contributor to the spread of HIV in Africa. 2 In East Africa, 40% to 50% of the married or cohabitating HIV-infected persons are in an HIV-discordant partnership. 3
Evidence suggests that HIV-negative partners in discordant relationships are at high risk of HIV infection. 2 Early studies on HIV incidence rates among discordant couples were generally small, with limitations, but reported overall HIV incidence rates of 8.3% per year. 4 However, more recent data have shown that HIV-negative partners in discordant relationships may have HIV incidence rates of 10% to 20% per year, approximately 10- to 100-fold higher than relationships where both the partners are HIV negative. 5 Thus, identifying such a group of the population will have a great impact in designing a preventive measure and tackling the HIV/AIDS pandemic. 2
In sub-Saharan Africa, there is evidence that the rates of discordance range from 3% to 20% in the general population, and higher rates of 20% to 35% were found in studies of those presenting to Voluntary Counseling and Testing (VCT) services. 6 In sub-Saharan Africa, approximately 1 of 2 HIV-1-infected persons living as a couple have a serodiscordant partner. Recent data suggest that a large proportion of new HIV-1 infections in mature epidemics occur within discordant couples, making discordance a major contributor to the spread of HIV/AIDS in Africa. 7 About less than 10% of HIV sero-positive individuals know their partners’ status, and only about 20% of the HIV discordant couples know that they are living in a discordant relationship in East Africa. 8
HIV transmission in couples has been associated with the ignorance of self or partner’s HIV status 8 and with limited understanding that HIV discordance can exist within couples. 9 Although the explanation of serodiscordance is not completely understood, some biological factors that may influence HIV transmission rates in discordant partnerships may include sex, pregnancy, coinfection with other sexually transmitted diseases (STDs), male circumcision, and virologic, genetic, and immunologic factors. 2 So far, there are few studies conducted on predictors of serodiscordants. Since there is no study that has been carried out on the prevalence of serodiscordance and associated factors in Ethiopia, this study will serve as the baseline data for further studies in this area of interest and most importantly the high prevalence of HIV/AIDS in Ethiopia. Hence, identifying such a group of this population will help in designing a new preventive strategy for HIV/AIDS regionally and at the country level, which can be accomplished by voluntary counseling and treatment. Subsequently, identifying immunological and clinical factors for discordance could help in predicting the seroconversion possibility among discordant partners and implementing preventive measures among serodiscordants, which will reduce the seroconversion rate in unaffected patients, thus significantly helping in tackling the HIV/AIDS epidemic in general. So the objective of this study is to assess the prevalence and predictors of HIV serodiscordance in couples registered at VCT center in the southwest of Ethiopia.
Methods
Study Setting and Context
The study was conducted at VCT center of Jimma University Specialized Hospital (JUSH) from October 1, 2010 to October 25, 2010. Jimma University Specialized Hospital is one of the teaching hospitals in the country located in Jimma town, Oromia region. The hospital serves as a referral hospital for southwestern Ethiopia including Jimma zone, which has a total population of 2 495 795 according to figures from the Central Statistical Agency in 2007. 10 The hospital is staffed with 1 general practitioner, 4 nurses, and a pharmacist who have trained in VCT service and management of people living with HIV.
Study Design and Participants
The study employed a case–control study design. The study patients were couples registered at the VCT center of JUSH and were tested for HIV. The inclusion criteria for the study were those older than 18 years, who reported to be married or to be a cohabiting couple whose couple serostatus is known and documented, and who have a complete medical chart. All 199 samples of serodiscordant couples registered at the VCT center of JUSH who fulfilled the inclusion criteria were included as cases, and equal numbers of seroconcordant couples were selected from the 658 registered seroconcordant couples; they served as the control group and were selected using a lottery method, making the total sample size 398. A 1:1 ratio was used to select for the control and the same number of HIV-positive concordant couples.
Data Collection Procedures and the Extracted Variables
The registration documents of the hospital contain basic information including patient’s age, sex, and address. Data were extracted from the registration book of the hospital using a structured data sheet specially designed for this study. Data extraction was made by nurse/health officers working at the VCT clinic of the hospital. To ensure quality of the data the following measures were taken: (1) a 1-day training was given for data collectors before the start of data collection, (2) the overall activities of data extraction were monitored by the principal investigator, and there was strict supervision during data collection, (3) all completed data sheets were examined by the principal investigator for completeness during data collection, and (4) consistencies of the collected data were checked during the analysis.
Measurement
Data on sociodemographic variables, baseline clinical characteristics like the World Health Organization (WHO) stage, and baseline CD4 count, past history of tuberculosis (TB) and TB treatment during VCT service, and risk behaviors like substance abuse, condom use, and couple status (discordant or concordant) were collected by a structured questionnaire and also through using a chart abstraction/review tool. The following operational definitions were used in this study.
Discordant couple is a couple where one partner is HIV positive, while the other is HIV negative. Couples were either married people or people cohabiting but not formally married, as reported by one of the couples and recorded on the charts.
Condom use was categorized as: (1) never or not asked: never have used a condom or not asked; (2) rarely: do use a condom whenever the patient thinks that the partner is a high-risk partner; (3) sometimes: use of condom for prevention of pregnancy; (4) mostly: use of condom unless forgets; (5) always: use of condom during every sexual intercourse.
Statistical Analysis
The quantitative data extracted from the registration book were checked for completeness and consistency by the principal investigator. Data entry and analyses were carried out using SPSS version 16.0 for Windows (SPSS, Chicago, Illinois). Descriptive statistics and bivariate analysis were performed. Multivariable analysis using a forward logistic regression model was used to identify independent predictors of serodiscordance. A P < .05 was considered to be statistically significant.
Ethical Considerations
Ethical clearance was obtained from the ethical review committee of Jimma University College of Public Health and Medical Sciences. An official letter was obtained from the Department of Internal Medicine and was given to the responsible body at the VCT center. Information obtained from the records was kept confidential by not recording the participant’s name and the unique VCT code number on the questionnaires; instead new code numbers were given by the principal investigator and later after data entry, the code numbers were permanently destroyed.
Results
Of the 2370 couples registered at VCT center of JUSH during the period 2003 to 2010, a total of 199 serodiscordants were found, and their data were analyzed in comparison with 199 seroconcordants.
In our study, 199 (8.4%) couples were found to live in serodiscordant relationships of a total of 2370 cohabiting couples who seek VCT service, thereby the prevalence of serodiscordance in the study area is 137 (5.8%) male discordants and 62 (2.6%) female discordants (Table 1). Among the 199 patients in a serodiscordant relationship, 137 (68.8%) were HIV-positive women while 62 (31.2%) were HIV-positive men.
Prevalence of Serodiscordance at VCT Center, JUSH, from 2003 to 2010.
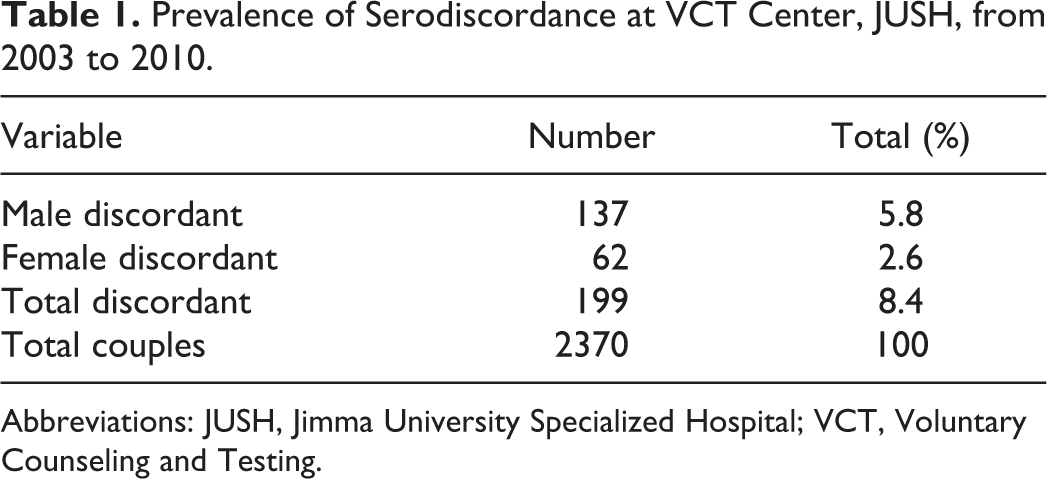
Abbreviations: JUSH, Jimma University Specialized Hospital; VCT, Voluntary Counseling and Testing.
Sociodemographic Variables and Couple Serostatus
The mean age of the discordant and concordant patients was 31.9 years (standard deviation [SD] = 8.5 years) and 31.4 years (SD = 8.1 years), respectively. Thirty three (45.8%) in the age group 18 to 24 years, 159 (50.6%) of those in age group 25 to 49 years, and 7 (58.3%) of those belonging to the age group of 50 years or older had a sero-negative partner. Regarding the level of education and couple serostatus, the majority (27 [55.1%]) had tertiary education and a sero-negative partner, while 78 (53.4%) had secondary education and a sero-positive partner. Concerning religion, 116 (51.1%), 57 (49.1%), and 26 (53.1%) of orthodox Christians, Muslims, and protestants, respectively, were in the discordant relationship. There was no association between sociodemographic variables and the couple’s serostatus (Table 2).
Sociodemographic Characteristics of Serodiscordants and Seroconcordants at VCT Center, JUSH, from 2003 to 2010.

Abbreviations: CI, confidence interval; JUSH, Jimma University Specialized Hospital; OR, odds ratio; VCT, Voluntary Counseling and Testing.
Clinical and Immunological Characteristics and Couple’s Serostatus
A total of 16 patients were found to have persistent generalized lymphadenopathy (PGL) of which 13 (81.2%) were serodiscordants, while only 3 (18.8%) were seroconcordants and HIV-positive individuals with PGL were 4 times more likely to have a negative partner than those without a history of PGL (COR = 4.56; 95% CI = 1.28-16.28). Of the 16 patients having active TB at enrollment, 15 (93.8%) were serodiscordants and 1 (6.2%) was a seroconcordant, and HIV-positive individuals with active TB at enrollment were 16 times more likely to have a negative partner than those with no active TB at enrollment (crude odds ratio [COR] = 16.14; 95% CI = 2.11-123.41).
Of the 136 patients having a history of past TB treatment, 58 (42.6%) were serodiscordants and 78 (57.4%) were seroconcordants, and HIV-positive individuals with past TB treatment were less likely to have negative partners (COR = 0.64; 95% CI: 0.42-0.96). Of the 129 patients with a past herpes zoster infection, 50 (38.8%) were serodiscordants, while 79 (61.2%) were seroconcordants, and HIV-positive individuals with a past herpes zoster infection were less likely to have a negative partner (COR = 0.51; 95% CI: 0.33-0.78). Of the 35 patients with oral candidiasis at enrollment, 16 (31.5%) were serodiscordants and 29 (64.4%) were seroconcordants, and HIV-positive individuals with oral candidiasis were less likely to have a negative partner (COR = 0.51, 95% CI = 0.26-0.97). Regarding the WHO clinical stage of the HIV-positive patient and the serostatus of the other partner, 32 (69.6%) of the participants are with WHO stage I HIV and 125 (50.2%) participants are with WHO stage IV HIV in serodiscordant and concordant relationships, respectively. There was an association between the WHO clinical stage of the HIV-positive patient and the serostatus of the other partner in a couple. Patients with WHO stages II to IV were more likely to have a sero-positive partner (COR [95% CI] = 2.71 [1.08-6.72], 3.47 [1.56-7.67], and 2.3 [1.17-4.52], respectively) as compared with those with WHO stage I.
Regarding CD4 count at enrollment, 62 (47%) of those having CD4 count <100 cells/mm3 and 11 (57.8%) of those having more than 500 cells/mm3 were in serodiscordant relationships. The mean CD4 count was found to be 183.3 cells/mm3 (SD = 166.8) and 179.9 cells/mm3 (SD = 166.8) for serodiscordants and concordants, respectively. There was no association between CD4 count of HIV-positive patients and the serostatus of the other partner of the couple (Table 3).
Clinical and Immunological Characteristics of Discordants versus Concordants in VCT Center, JUSH, from 2003 to 2010.

Abbreviations: CI, confidence interval; JUSH, Jimma University Specialized Hospital; PGT, persistent generalized lymphadenopathy; OR, odds ratio; TB, tuberculosis; VCT, Voluntary Counseling and Testing; WHO, World Health Organization.
Regarding condom use behavior of HIV-positive patients and the serostatus of the other partner of the couple, the majority (2 [66.7%]) of those who used condoms mostly or always had a sero-negative partner when compared with those who used condoms rarely (2 [12.5%]) and sometimes (5 [27.8%]). Those who used condoms sometimes or rarely were more likely to have a concordant positive partner, COR (95% CI) = 7.77 (1.74-34.71) and 2.88 (1-8.27), respectively. Among 199 serodiscordants compared with 199 seroconcordants for functional status at enrollment, 126 (53.6%), 63 (45%), and 10 (43.5%) of the working, ambulating, and bedridden, respectively, were in the serodiscordant relationship. The functional status of the HIV-positive patient has no association with the serostatus of the other partner of the couple (Tables 1 and 4).
Social and Behavioral Characteristics of Discordants versus Concordants in the VCT Center, JUSH, from 2003 to 2010.

Abbreviations: CI, confidence interval; JUSH, Jimma University Specialized Hospital; OR, odds ratio; VCT, Voluntary Counseling and Testing.
Predictors of Serodiscordance
Comparing the 199 serodiscordants to 199 seroconcordants for predictors of serodiscordance after binary logistic regression by adjusting confounding factors, HIV-positive individuals who used condoms rarely were 7 times more likely to have a negative partner than those who never used condoms (AOR = 7.2; 95% CI = (1.59-32.54), and HIV-positive individuals with active TB at enrollment were 17 times more likely to have a negative partner than with no history of active TB at enrollment (AOR = 17.7; 95% CI =2.25-139.18; Table 5).
Predictors of Serodiscordance in VCT Center, JUSH, from 2003 to 2010.

Abbreviations: CI, confidence interval; JUSH, Jimma University Specialized Hospital; PGT, persistent generalized lymphadenopathy; OR, odds ratio; TB, tuberculosis; VCT, Voluntary Counseling and Testing; WHO, World Health Organization.
Discussion
This study is a hospital-based study that limits generalization of the findings to the HIV-infected population; otherwise, it revealed the prevalence and predictors of serosdiscordance in the VCT center of JUSH. This study has included all discordant patients during the period 2003 to 2010 to examine the prevalence and predictors of serodiscordance in discordant and concordant couples in the context of the global pattern.
The prevalence of serodiscordance in the study area was found to be 8.4% compared with the figures from other studies, including the Rwandan study that showed a prevalence of 12% of discordance in couples presenting for VCT service. 11 About 107 patients (38.7%) belonged to a serodiscordant couple. 12 In fact, it is also found to be much lower from the data that estimates a serodiscordance prevalence rate of 20% to 30% in sub-Saharan African countries. 13 The possible explanation could be the regional difference in serodiscordance rates that is observed all over the world. 6 In addition, the study has revealed that the majority in serodiscordant relationships are sero-positive women, which is consistent with the fact that women have a higher risk of acquiring HIV infection compared with men. 14 Compared with men, women were significantly less likely to be serodiscordant (were HIV-positive concordant; odds ratio [OR]: 1.19; 95% CI: 1.02-1.38). 12 Unlike our study participants in Uganda, the study population comprised 293 HIV-discordant couples, among whom the male partner was HIV infected in 192 (65.5%) and the female partner was HIV infected in 101 (34.5%) of the couples. 15 In Kenya AIDS Indicator Survey 2007, an overall 9.6% (95% CI: 8.3-10.9) of the couples were affected by HIV; 3.8% (95% CI: 3.0-4.5) were concordantly infected, and 5.8% were discordantly infected (95% CI: 4.7-6.8). 16 Of the 3408 HIV-1-serodiscordant couples enrolled, 67% of the HIV-1-infected partners were women. 17 The proportion of discordant couples with an HIV-positive man is almost the same as that of discordant couples with an HIV-positive woman. 18
One explanation for discordance may be that partners may not have been primarily susceptible to HIV acquisition. 12 Indeed, regarding the risk of HIV transmission in heterosexual intercourse, both infectiousness of the infected partner and susceptibility of the uninfected partner are critical. 19
Until recently, most of the studies following up HIV-negative or HIV-serodiscordant couples in countries with generalized HIV epidemics tended to show that women were at especially high risk of HIV infection from within their regular partnership, presumably due to their higher biological susceptibility and the infidelity of the men. 20 These data were reinforced by individual representations: women feared being infected by their spouse/regular partner, whereas men feared HIV infection from “outside” partners. 21 So, prevention efforts need to be focused to address this matter with respect to point of care and patient management. Understanding of HIV discordance, even among health care providers, is limited, and common misconceptions may undermine the risk reduction efforts. 22
In our study, HIV-positive individuals who rarely used condoms were 7 times more likely to have a negative partner than those who never used condoms, and this was found to be a predictor of serodiscordance. A review of the published studies on discordant couples in Sub-Saharan African countries, which was undertaken to ascertain factors that may explain high rates of HIV discordance and why some individuals remain uninfected despite repeated exposure to HIV, identified a number of correlates of transmission, including condom use. 23 Respondents who used condoms during their last sexual intercourse were significantly less likely to be serodiscordant (OR: 0.52; 95% CI: 0.28-0.96). 12 Transmission among couples has been reduced by 80% with effective interventions, including couple-specific counseling and testing and condom provision. 24 Less than 3% of the couples reported current condom use prior to VCT. In the year after VCT, >80% of reported acts of intercourse in discordant couples included condom use. 25 In fact, discordant couples who have received VCT and other interventions have lower seroconversion rates; however, incidence within these couples remains high, ranging from 3% to 8% annually 6 ; thus, different strategies have been undertaken and evaluated and found to have a sound impact. HIV counseling and testing (VCT) of couples with follow-up has resulted in sustained increases in reported condom use from 3% at baseline to 80% after VCT among discordant couples in Zambia. 26
The proportion of discordant couples using condoms increased from 4% to 57% after 1 year of follow-up. During follow-up, 2 of the 23 HIV-negative men and 6 of the 30 HIV-negative women seroconverted. Confidential HIV serotesting with counseling caused a large increase in condom use and was associated with a lower rate of new HIV infections. HIV testing is a promising intervention for preventing the spread of HIV in Africa. 24
Interestingly, the other predictor of serodiscordance, which is active TB at enrollment, contradicts the finding that patients with an active infection will have high viral load and hence highly likely to transmit the virus to their partner. 14 A cross-sectional study was performed to define predictors of HIV status and assess their differences by sex and geography in 2 study cohorts: 1351 heterosexual couples recruited from a VCT center in Lusaka, Zambia and 1458 women recruited from antenatal and pediatrics clinics in Kigali, Rwanda. Multivariable logistic regression modeling showed that history of TB (OR: 2.8-20.7) was strongly predictive of seropositivity. 27
Our findings make the issue of understanding discordance relative to active TB a little more difficult to understand and underscore the need for further study in this area.
In our study, interestingly, the clinical stage, such as WHO clinical stage, and immunological factors like CD4 count were found to have no association with serodiscordance, making the issue of discordance more difficult and suggesting the need for more studies in this area of interest.
In conclusion, the prevalence of serodiscordance in the VCT center of JUSH is found to be 8.4%, which is low compared with other studies. Using a condom rarely and active TB at enrollment are the predictors of serodiscordance (HIV-positive individuals who rarely use a condom and have active TB at enrollment are more likely to have a negative partner than those who never use condom and have no active TB at enrollment). Preventive strategies designed to prevent seroconversion of a negative partner in a serodiscordant relationship are recommended. Further studies are needed to see the prevalence in different regions of the country. Sero-positive individuals who rarely use a condom should increase the possibility that the patient can have negative partners; hence, such patients should be encouraged to have their partners get tested. However, the fact that active infection is permissive to HIV transmission and is against the association between active TB and serodiscordance in this study warrants the need for further study to ascertain this association.
Footnotes
Acknowledgments
The authors thank VCT center of Jimma University Specialized Hospital and staff for their cooperation.
Authors’ Note
EH, AY, and FA conceived and designed the study and collected data in the field, performed analysis, interpreted the data, and drafted the manuscript. FA assisted with the design, interpretation of data, and the critical review of the manuscript. KD and SB participated in analysis and interpretation of data, helped in drafting the manuscript, and critically reviewed the manuscript. All authors read and approved the final manuscript. All authors participated in critical appraisal and revision of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We are grateful to Jimma University for funding this project.