
Abstract
We conducted a study to investigate HIV and hepatitis delta virus (HDV) coinfection among patients with chronic hepatitis B virus (HBV) infection and the triple infection’s (HIV/HBV/HDV) clinical implications in India, an intermediate HBV endemic region, with an estimated HIV-positive population of 2.5 million. A total of 450 patients (men: 270; women: 180) with chronic HBV infections and 135 healthy volunteers were screened for HIV and HDV. The incidence of the triple infection was low (4 [0.8%]) compared with dual infections of HIV-1/HBV (7 [1.5%]) and HBV/HDV (22[4.8%]). Among 21- to 40-year-olds, HBV/HDV coinfection (45.8%) and HBV/HDV/HIV-1 triple infection was predominant (75%). Among 11 patients coinfected with HIV-1/HBV, 4 (36%) were tri-infected and were also associated with chronic hepatitis and cirrhosis. The HDV coinfection was higher among patients coinfected with HBV/HIV-1, despite the declining trend in HDV infection among HIV-negative patients, as previously reported. Thus, it is important to assess the impact of HIV, chronic HBV, and HDV tri-infection in India.
Keywords
Introduction
There is a high degree of epidemiologic similarity among hepatitis B virus (HBV), hepatitis delta virus (HDV), and HIV. Specifically, these viruses share high-risk groups, routes of transmission, and certain clinical manifestations, such as increased liver-related morbidity. 1,2 India’s status as an intermediate region of HBV infection indicates 2% to 4% of HBV in the general population and an even higher percentage within the HIV-infected population. 3,4 With this in mind, HDV requires a helper function provided exclusively by HBV. 5 Studies suggest that the majority of HDV infections are acquired through parenteral and sexual routes, 6 –8 which are also important routes for HIV transmission. India, with a whopping 2.5 million cases of HIV infection, has the unfortunate distinction of harboring the third highest number of HIV-positive patients in the world. Because of the culmination of the aforementioned dynamics, we conducted a study to investigate HIV and HDV coinfection among patients with chronic HBV (CHBV) infection, in India.
It has been estimated that ∼5% of the HBV carriers are also coinfected with HDV, resulting in ∼15 million people infected with HDV worldwide. 9 Clinical studies assessing the impact of HDV infection on patients coinfected with HBV–HIV were limited and yielded inconsistent results before the introduction of highly active antiretroviral therapy (HAART). 10 –13 Some reports suggest that in patients with CHBV infection, HDV coinfection may suppress HBV replication, with subsequent clearance of hepatitis B surface antigen (HBsAg) 14 –16 by inhibiting the host DNA-dependent RNA polymerase involved in HBV transcription. 17,18 Others argue that HIV infection might worsen chronic liver damage caused by HDV, 6,10 and that HIV patients with long-term HDV infection were more likely to develop cirrhosis than were patients with HBV infection alone. 19 To the same end, HDV/HBV/HIV tri-infection may lead to exacerbation and rapid progression of chronic liver disease, hepatic failure, and death. 6,8 Still other studies conclude that the course of long-term HDV infection was not influenced by concomitant HIV infection. 11 –13 The interaction of HBV with HDV coinfection was shown to significantly suppress HBV replication that might ameliorate the damage incurred as a result of HBV infection. 19 Because of the confounding literature on the impact of HDV infection on patients with HBV–HIV coinfection (prior to HAART), we investigated the HBV DNA in blood samples and liver cirrhosis in the setting of HBV/HDV/HIV tri-infection.
Materials and Methods
Between 2003 and 2005, patients with liver complications were referred from various gastroenterology departments to the National Reference Center for Viral Hepatitis, Department of Microbiology, Dr ALM PGIBMS, University of Madras, Chennai, Tamil Nadu, India. All patients were interviewed on the basis of a predesigned questionnaire regarding blood transfusion history, surgery/dental/gynecological procedures, exposure to syringes and needles, ear piercing, and behavioral information, such as intravenous drug abuse, sexual promiscuity, tattooing, and so on. None of the patients had a history of hemodialysis or organ transplantation.
A total of 450 patients with CHBV infection, including 279 asymptomatic patients, followed by 92 patients with chronic hepatitis, 47 patients with cirrhosis, and 32 patients with hepatocellular carcinoma, were analyzed for the study. During the same study period, 135 healthy volunteers were also analyzed. The following markers of HBV and HDV enzyme-linked immunosorbent assay (ELISA) kits: HBsAg, hepatitis B e antigen HBeAg/anti-HBe (Biorad Laboratories, Hercules, California), and anti-HDV Immunoglobulin M (DiaSorin, Italy) were detected using commercially available kits with known positive and negative controls. The HIV antibodies were detected by ELISA (HIV Microlisa; J. Mitra & Co, India), and reactive samples were subjected to 2 other rapid/simple tests (Comb AIDS-RS; RS; Span Diagnostics, India and HIV TRIDOT; J. Mitra & Co). The available biochemical, clinical, and liver histopathological data were correlated with the virological profile. The HBV DNA polymerase chain reaction (PCR) 20 was performed with appropriate positive and negative controls as described by Cheung. The sensitivities of our HBV DNA PCR assay reached 10 copies of HBV DNA per specimen, as determined by testing 10-fold serial dilutions of HBV DNA of known amounts.
Results
The retrospective demographic data of these patients showed that of the 450 patients, 270 (60%) were male patients and 180 (40%) were female patients, and the mean age was 32 years (95% confidence interval [CI] ± 3.5 years, range 8-67 years). The predominant mode of acquiring HIV infection was heterosexual contact (73%) followed by blood transfusion products/surgery, tattoo/ear piercing, and dental procedures/hospitalization (9%). Among patients with CHBV infection, tattoo/ear piercing was the predominant mode of transmission (45%) followed by dental procedures/hospitalization (22%), blood products/surgery (13%), heterosexual contact (11%), intravenous drug use (1%), and unknown (8%; Table 1).
Demographic Details of Patients Co-infected with Chronic HBV and HIV-1 (n = 450).
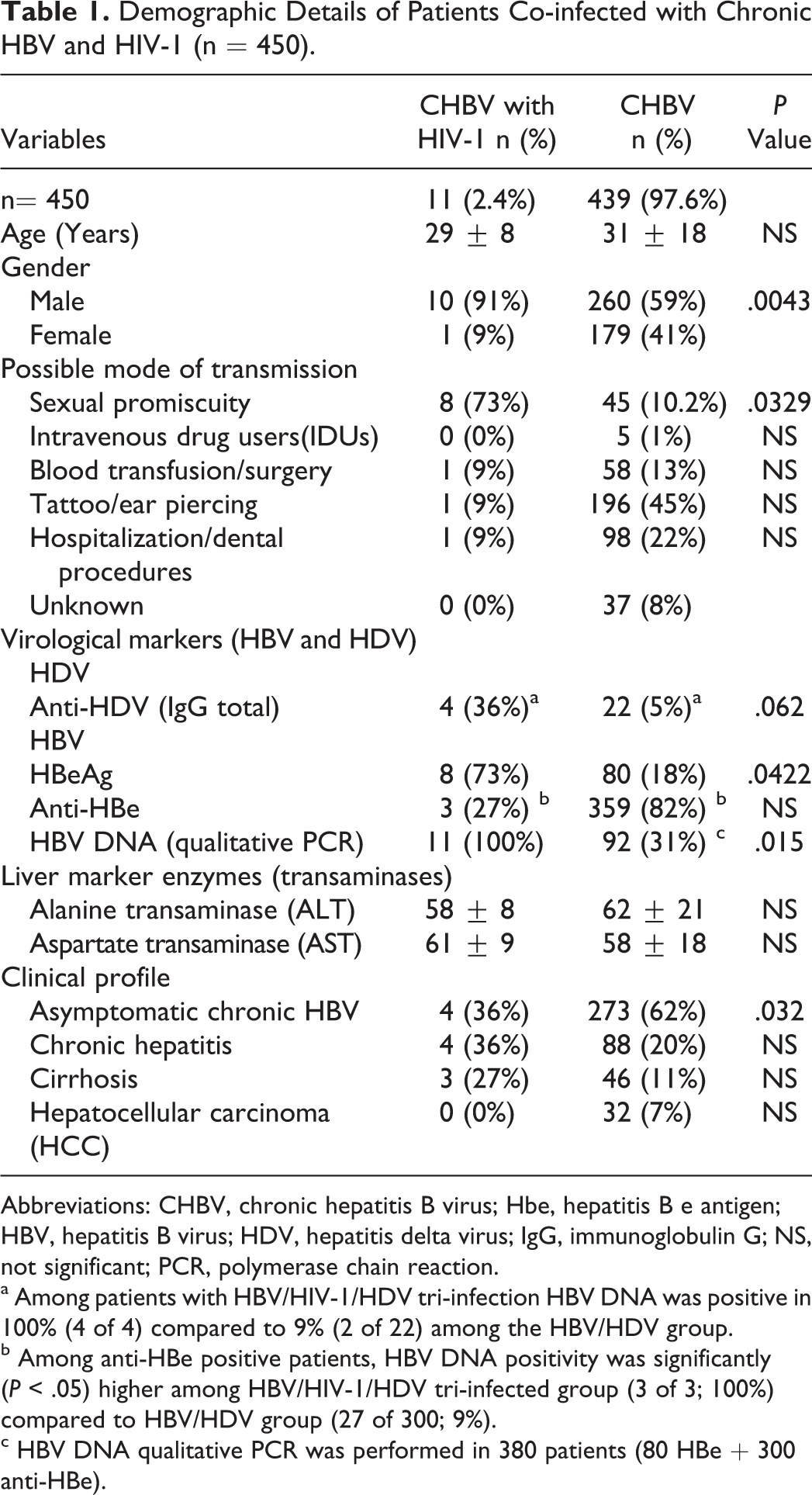
Abbreviations: CHBV, chronic hepatitis B virus; Hbe, hepatitis B e antigen; HBV, hepatitis B virus; HDV, hepatitis delta virus; IgG, immunoglobulin G; NS, not significant; PCR, polymerase chain reaction.
a Among patients with HBV/HIV-1/HDV tri-infection HBV DNA was positive in 100% (4 of 4) compared to 9% (2 of 22) among the HBV/HDV group.
b Among anti-HBe positive patients, HBV DNA positivity was significantly (P < .05) higher among HBV/HIV-1/HDV tri-infected group (3 of 3; 100%) compared to HBV/HDV group (27 of 300; 9%).
c HBV DNA qualitative PCR was performed in 380 patients (80 HBe + 300 anti-HBe).
Among the 135 healthy volunteers, 90 (66.6%) were men and 45 (33.3%) were women. The mean age of the study group was 28 years (95% CI ± 2.8 years, range 18-42 years).
Prevalence of Viral Coinfections
Overall, the prevalence of coinfection of HBV with HDV was 5.7% (26 of 450) and HBV with HIV was 2.4% (11 of 450). All the patients coinfected with HIV were confirmed as HIV-1 (Table 1). Among the HIV-positive patients, the rate of HDV tri-infection was 36% (4 of 11); all of the 4 patients were male. Among the control group, HBsAg positivity was observed in 2% (3 of 135), all of whom were HDV negative. None of our healthy participants was found to be positive for HIV1/HIV2.
The majority of the HIV-infected patients comprised the 21- to 40-year age group (71%) followed by the 41- to 60-year age group (29%). Mean age of the patients with HIV/HBV was 29 years (95% CI ± 2.8 years). The HBV/HDV coinfection was highest in the 21- to 40-year age group (45.8%), while HIV/HBV/HDV tri-infection was also predominant (75%) in the same age group (Table 1; Figure 1).
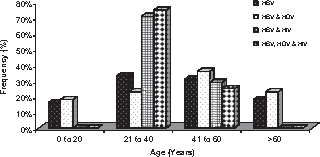
Age-related distribution of human immunodeficiency virus (HIV) and hepatitis delta virus (HDV) coinfection among patients with chronic hepatitis B virus (HBV) infection.
Although not significant, there was a trend showing a decrease in HDV in patients not infected with HIV but infected with CHBV (5%; 22 of 439). The serum aminotransferase was not significant in patients c-infected with HIV compared to CHBV alone (Table 1). Overall, coinfection of HDV and HIV among patients with CHBV was 0.88% (4 of 450).
HBV DNA Analysis
The HBeAg positivity was significantly higher among patients coinfected with HIV than patients with CHBV infection alone (73% versus 18%; P < .05), whereas the HBe seroconversion was higher in the patients with CHBV compared with patients with HIV coinfection (82% versus 27%, P < .05). The HBV DNA was found to be higher in patients coinfected with HIV having CHBV infection than patients uninfected with HIV (100% versus 31%, P < .05). Among the HIV/HBV/HDV (n = 4) tri-infected group, all 4 patients were HBV DNA positive, of which 3 (75%) patients had anti-HBe and 1 (25%) patient had HBe. The HBV DNA positivity was significantly higher (P < .05) in tri-infected (HIV/HBV/HDV) and coinfected (HIV/HBV) patients compared with the group not infected with HIV. Among patients not infected with HIV-1/HIV-2 but having CHBV infection and HDV infection (n = 22), none of the patients were HBV DNA positive in spite of HBe (2 of 22; 9%) and anti-HBe (20 of 22; 91%) positivity (Table 2).
HBV Markers Profile among Various Groups (n = 450).
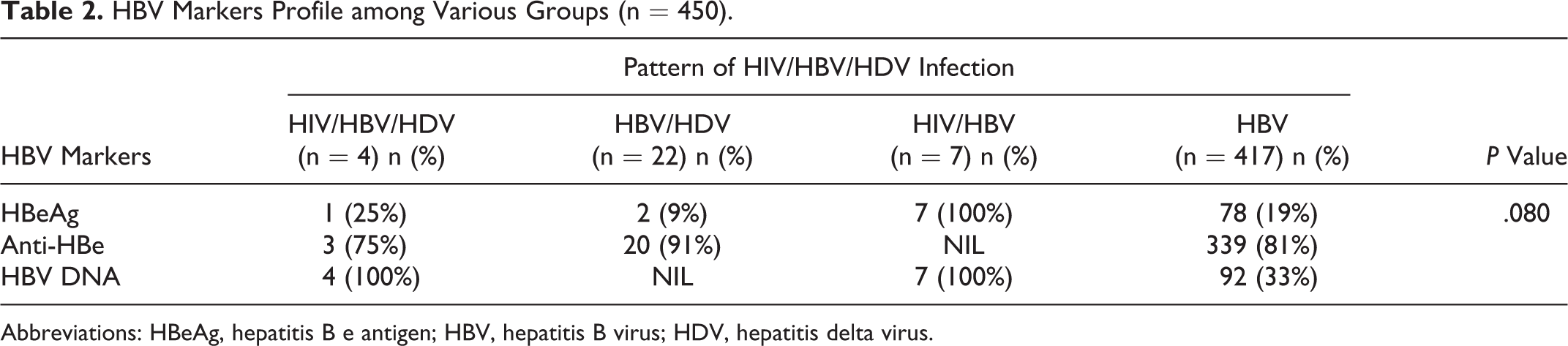
Abbreviations: HBeAg, hepatitis B e antigen; HBV, hepatitis B virus; HDV, hepatitis delta virus.
Clinical Implications
Among the 4 patients with HIV/HBV/HDV tri-infection, 3 (75%) patients were diagnosed as having chronic hepatitis with cirrhosis, and 1 patient was asymptomatic for CHBV infection. Of the 11 patients coinfected with HIV/HBV, 4 (34%) had asymptomatic CHBV infection. Conversely, in patients not infected with HIV having CHBV infection (n = 22), the majority of the HDV infection was asymptomatic (68%; 15 of 22), but the patients' viremic (HDV RNA) status was not analyzed.
Discussion
Our results demonstrate that the triple infection of HIV, HBV, and HDV is rare but may increase the risk of progression to chronic liver disease. Previous studies have estimated that 1.9% to 5% of HIV-infected patients are coinfected with both HBV and HDV, with tri-infection especially common among injection drug users. 21,22 Although our cohort included few injection drug users, we showed a higher prevalence of HDV infection (36%) among patients with HBV/HIV coinfection than that in the general population of Indian HBsAg carriers (2.7%-5%). 23,24 This directly counters a previous study where we demonstrated a declining phase of HDV among CHBV infection in this part of India. 25 Our current study shows that the maximum levels (>70%) of HIV/HBV coinfection and the HIV/HBV/HDV tri-infection occurred in the 21- to 40-year age group, which is the most common age group for HIV positivity as demonstrated in the Indian literature. 26 –28 The higher rate of HDV/HBV infection among our HIV-infected patients in India may be related to multiple sexual encounters, 7 since HBV infection is endemic and sexual contact is the major risk factor for HIV transmission 29 in this region.
Our study found the majority (75%) of the tri-infected patients had chronic hepatitis with cirrhosis compared with 11% of the patients with HIV/HBV coinfection and 27% of the patients with HBV/HDV coinfection. The clinical manifestations of patients tri-infected with HDV/HIV/HBV remain unclear, although HIV infection appears to have marked influence on the natural history of HBV infection. Our data regarding possible clinical effects of HIV/HBV/HDV, although not statistically significant, certainly warrants more study, especially in conjunction with the increase in HDV infection among HIV-positive patients. The HBsAg carriers permit a continuous replication of HDV, which may play a role in the development of fulminant hepatitis and accelerate the progression of chronic liver damage, irrespective of the HIV status. 6,7,18,22,30 Some studies have shown the putative direct cytopathic effect of replicating HDV on hastening the liver fibrosis process, leading to a more rapid fibrosis and an accelerated progression toward decompensated cirrhosis. 31 –33 The HDV coinfection may lead to exacerbation and rapid progression of chronic liver disease and hepatic failure in patients with HBV/HIV coinfection. 6,8 Moreover, patients with long-term HDV infection were more likely to develop cirrhosis than patients with HBV infection alone. 19 This proposed dynamic, in combination with India’s status as an intermediate HBV-endemic region, suggests that more and more HDV superinfections are to be expected, as the AIDS epidemic expands in this part of the country. Such a profile would have important public health implications, as more chronic liver diseases would be expected.
Although HDV coinfection conferred virological benefit by suppression of HBV replication, this suppression is not the case in patients coinfected with HIV. 13 Our study, consistent with other reports, observed increased hepatotropic viral replication in HIV-infected patients.
Several reports in India have observed a change in HDV epidemiology toward a declining phase. Recently, we have confirmed the trend among patients with liver disease 25 ; yet, the HDV coinfection was higher in patients with CHBV infection who were also coinfected with HIV. It may prove difficult to predict whether HDV was acquired as a coinfection with HBV/HIV or as a superinfection in patients with existing chronic HBV/HIV coinfection. Treatment guidelines on HIV-HBV coinfection management outlined the importance of early treatment of chronic HBV;although efficient antiviral drugs are available to treat patients coinfected with HBV and HIV, 22 the treatment of HDV is still an unsolved issue.
In patients with HDV having HBV coinfection, a biphasic increase in serum aminotransferase activity has been commonly observed in the clinical setting, which may help to differentiate it from histologically indistinguishable acute HBV infection. However, since no large study has demonstrated the proportion of cases of HDV coinfection presenting with such a clinical manifestation, the accuracy of using this feature to diagnose HBV and HDV coinfection remains unproven. Although the clinical effects of HDV and HBV coinfection may range from mild to severe fulminant hepatitis, 34 complete clinical recovery from acute self-limiting disease with no chronic sequelae is usually the rule.
The triple infection (HIV/HBV/HDV) seems to have an effect on the natural history of HBV, which may have implications for hepatitis policies. Epidemiologic studies should be considered to monitor a possible increase in the spread of HDV among populations at risk of HIV and HBV infections. Prolonged survival of HIV-infected patients coinfected with HBV and HDV may become an important clinical concern due to increases in cirrhosis. Failing to include equal proportions of risk group populations in every category and HDV RNA not being carried out are the potential limitations of this study.
Although HBV is still the major cause of chronic liver disease followed by hepatitis C virus, the devastating (HIV, HBV, and HDV) tri-infection appears to be of significant and of epidemiologic importance in the light of high heterosexual transmission of HIV in India. In lieu of these observations, routine evaluation of HDV markers should be performed in all individuals coinfected with HBV/HIV for better prognosis and survival and to efficiently control by selecting the antiretroviral therapy regimen involving anti-HBV agents and manage the situation in this tropical region.
Footnotes
Acknowledgments
The authors thank the study participants and the assistance rendered by the gastroenterologists and pathologists in conducting the study.
Authors’ Note
SSa, VV, and SPT conceived and designed the study. SSa enrolled and interviewed the patients. VM and SSo managed and followed up the cases. SSa and VV used the diagnostic kits to detect HIV-1 and -2 and HDV infections. KGM and PB acquired, analyzed, and interpreted the data. KGM, PB, and GW helped in statistical analysis of the data. NK, DM, KMH, SS, and SPT critically revised the manuscript. All authors read and approved the final manuscript. SSa and SPT are guarantors of the article. The study was approved by the institutional ethics committee of the Dr ALM PG Institute of Basic Medical Sciences (Dr ALM PG IBMS), University of Madras, Chennai, Tamil Nadu, India.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Indian Council of Medical Research (ICMR), Government of India, New Delhi under the grant-in-aid program for the ‘Referral Centre for Chronic Hepatitis Serology and Molecular Virology’.