
Abstract
This study was based on an analysis of an existing database compiled from 475 medical records of people living with HIV/AIDS admitted to an acute-care hospital in New York City in 2004. The characteristics of patients with HIV infection that received physical therapy were determined. Differences between patients with HIV infection that did and did not receive physical therapy, as well as predictors of receipt of physical therapy, were identified. The physical therapy subgroup (n = 69) had a mean age of 48.3 years, consisted of more men than women, and was predominately black, with public health insurance. Admissions were commonly due to non-AIDS-defining illness as the primary diagnoses, accompanied by several comorbidities. Admissions often presented with functional deficits, incurred a prolonged length of stay, and required assistance at discharge. Differences existed between the physical therapy subgroup and the non-physical therapy subgroup (n = 406). Predictors of receipt of physical therapy were functional status on admission and length of stay.
In 2009, there were an estimated 784 701 people living with HIV infection and 476 732 people living with AIDS in the United States, of which, New York was the state with the highest prevalence. 1 There were 49 367 people living with HIV and 78 017 people living with AIDS in New York, of which, approximately 75% resided in New York City. 2 According to the New York City Department of Health and Mental Hygiene, 3 New York City was and continues to be “the epicenter of the HIV/AIDS epidemic in the United States.”
Since 1996, highly active antiretroviral therapy (HAART) significantly reduced mortality associated with AIDS in the United States. 4 Between 2000 and 2009, death rates for AIDS decreased and prevalence rates for AIDS increased. 5 Once thought of as a terminal illness, HIV infection is increasingly regarded as a chronic disease.6,7 As such, there is a high prevalence of disability among people living with HIV/AIDS (PLWHA).8–10 Although only a minority of rehabilitation professionals work with PLWHA, 11 the rehabilitation professional community has the potential to play a greater role in addressing HIV/AIDS disability. 12
The role of rehabilitation in the management of HIV/AIDS disability prior to and at the beginning of the HAART era has been thoroughly described, yet little is known regarding the role of rehabilitation in the management of HIV/AIDS disability in the HAART era.
Physical rehabilitation services include, but are not limited to, physical, occupational, and speech-language therapies. In the HAART era, research pertaining to physical therapy and HIV/AIDS is sparse and narrow in scope, investigating efficacy13–22 or knowledge.11,23,24
Studies examining efficacy of physical therapy intervention in patients with HIV infection are mainly limited to specific techniques in small patient subpopulations13–16 or case reports.17–19 In addition, Hilburn et al 20 developed and evaluated a gross motor screening test for infants with HIV infection in developing countries. Dawad and Jobson 21 explored the use of a community-based rehabilitation program as a model for HIV-related task-shifting programs in South Africa. Maharaj and Chetty 22 developed and evaluated a rehabilitation program of moderate intensity exercises with a home program for PLWHA on HAART.
Studies examining knowledge of physical therapists23,24 and rehabilitation professionals 11 about HIV/AIDS revealed a lack of knowledge or discrepancies between perceived and actual knowledge. Yet, in the pre-HAART era, HIV/AIDS education was shown to improve knowledge of physical therapy students25,26 and efforts have begun to determine the ideal HIV/AIDS rehabilitation curriculum.27,28 Solomon et al conducted an interprofessional problem-based learning course on rehabilitation issues in HIV that students reported increased their learning and rehabilitation perspective. 29
Educating physical therapy students and clinicians regarding their roles in addressing HIV/AIDS disability requires an understanding of patients with HIV infection that receive physical therapy. Other than case reports describing individual patients with HIV infection in acute inpatient rehabilitation,30,31 there have been no recent studies aimed at identifying patients with HIV infection that receive physical therapy. Exploring access to rehabilitation among PLWHA has been identified as a key research priority in the field of HIV/AIDS and rehabilitation. 32 The purpose of this study was to examine PLWHA that accessed physical therapy after admission to an acute-care hospital in a large academic medical center in New York City. The specific aims of this project were to (1) determine the demographic, diagnostic, and hospitalization characteristics of patients with HIV infection that received physical therapy; (2) determine the impairments and functional limitations of patients with HIV infection that received physical therapy; (3) identify differences between patients with HIV infection that did and did not receive physical therapy; (4) identify predictors of receipt of physical therapy for patients with HIV infection.
Methods
An analysis was conducted of an existing deidentified database that had been created retrospectively for a utilization review for a clinical department at the medical center. Data collection was monitored for accuracy. Compilation of the database was done for nonresearch purposes in accordance with applicable laws and regulations, including the Health Insurance Portability and Accountability Act of 1996.
The database was compiled from medical records of adult (≥18 year old) patients admitted during the time period from January 1, 2004 to June 30, 2004 who were known to be HIV positive during admission. If a patient incurred greater than one admission during the time period, each admission was treated as a separate data-entry point. If a patient received a doctor’s order for physical therapy, a physical therapy initial evaluation, and was not discharged from physical therapy upon initial evaluation, the admission was assigned to the physical therapy subgroup; all other patient admissions were assigned to the nonphysical therapy subgroup. Patient admissions were excluded if the admission was for research purposes or if the medical record was missing, in use, or incomplete. Analyzed data included demographic information (age, sex, race, and primary insurance), diagnoses (primary, comorbidities), and hospitalization characteristics (functional status on admission, length of stay, and discharge disposition). Impairments and functional limitations were specified for the physical therapy subgroup only.
Age was recorded in years and categorized by quintiles. Sex was recorded as male or female. Race was recorded as white, black, Hispanic, or other. Primary insurance was recorded as Medicaid, Medicare, or private/self-pay.
Each patient admission had 1 admission diagnosis and anywhere from 1 to 24 discharge diagnoses. The first discharge diagnosis that was not HIV infection or AIDS was operationally defined as the primary diagnosis. Each primary diagnosis was classified using 2 schemes (1) as a non-AIDS-defining illness (non-ADI) or an ADI based on the US Centers for Disease Control and Prevention (CDC) category C 33 and (2) as a type of health or health-related condition using the International Classification of Disease, Ninth Revision, Clinical Modification (ICD-9-CM)-based classification groups. 34 All remaining discharge diagnoses were classified using the ICD-9-based classification groups. 35 The presence of comorbidities was determined for each patient admission by recording the total number of discharge diagnoses (excluding HIV infection, AIDS, and the primary diagnosis) and the occurrence of discharge diagnoses (excluding HIV infection, AIDS, and the primary diagnosis) in each of the ICD-9-based classification groups. 34 If a patient admission had one or more than one discharge diagnosis within a specified classification group, it was recorded as one or more. If a patient admission had no discharge diagnoses within a specified classification group, it was recorded as none.
Functional status on admission was determined by nursing assessment. Functional status on bed mobility, transfers, and ambulation was categorized as independent, requires assistance, or not assessed/missing. Data from the 3 functional status on admission measures were combined into a functional status on admission summary measure indicating independence with all assessed functional tasks, required assistance with any of the 3 functional tasks, or not assessed/missing on all 3 functional tasks. Length of stay was recorded as the total number of days of care (counting the date of admission but not the date of discharge) and categorized by quartiles. Discharge disposition was categorized as home, home with health care services, inpatient setting (acute rehabilitation, skilled nursing facility), or other (homeless or temporary housing, institutional setting, left against medical advice, died during admission, or missing).
The presence of impairments and functional limitations was determined by physical therapy initial evaluation. Each patient admission in the physical therapy subgroup could have one or more impairment or functional limitation. The total number of impairments and functional limitations was recorded. Identified impairments and functional limitations were categorized as decreased strength, decreased range of motion, decreased endurance, decreased balance, pain, decreased bed mobility, decreased transfer status, decreased ambulation status, decreased ability to negotiate stairs, decreased function/mobility, decreased aeration/cough efficacy/mobilization of secretions, or other.
Statistical analysis was conducted using PASW Statistics 18 (SPSS Inc, Chicago, Illinois) statistical software. To describe the total sample, physical therapy subgroup, and nonphysical therapy subgroup, descriptive statistics were performed. Categorical data are reported as frequencies and percentages. Continuous data are reported as means ± standard deviations (SDs). To identify the differences between the physical therapy subgroup and nonphysical therapy subgroup, chi-square tests or t tests were performed. To identify the predictors of receipt of physical therapy, a full-entry multivariable logistic regression analysis was performed. Because of insufficient sample size, several variables were transformed into dichotomous variables (age: <40 years or ≥40 years, race: non-black or black, primary insurance: Medicaid or private/self-pay/Medicare, length of stay: <8 days or ≥8 days) for the logistic regression analysis. Of all, 11.4% of the patient admissions had not assessed/missing functional status on admission summary data; however, these patient admissions were retained for the logistic regression analysis by creating the not assessed/missing category. There were no other patient admissions with any missing data. Discharge diagnoses classified using the ICD-9-based classification groups
25
were not compared between the physical therapy and nonphysical therapy subgroups because of the large number of diagnostic categories and the small number of patient admissions within some of the diagnostic categories. A P value of
Results
A total of 475 patient admissions were included in the database. Of the 475 admissions, 134 received a doctor’s order for physical therapy, and 104 of those admissions actually received a physical therapy initial evaluation. There were 69 admissions during which the patient was not discharged from physical therapy upon initial evaluation, representing 14.5% of the total number of patient admissions, comprising the physical therapy subgroup. The remaining 406 admissions, representing 85.5% of the total number of patient admissions, comprised the nonphysical therapy subgroup.
Characteristics of the Physical Therapy Subgroup
Table 1 presents the demographic characteristics of the total sample, physical therapy subgroup, and nonphysical therapy subgroup. The physical therapy subgroup had a mean (standard deviation [SD]) age of 48.3 (10.3) years, with a range from 28 to 78 years. In all, 56.5% (39 of 69) of patient admissions were men and 43.5% (30 of 69) were women. The majority of patient admissions were black (65.2%; 45 of 69). In all, 60.9% (42 of 69) of patient admissions had Medicaid and 27.5% (19 of 69) had Medicare as their primary health insurance.
Sample Demographic Characteristics.

aMean ± standard deviation.
bIn chi-square test, 1 (10%) cell had an expected count less than 5.
Table 2 presents the diagnoses of the total sample, physical therapy subgroup, and nonphysical therapy subgroup. Based on the CDC category C, 33 the physical therapy subgroup’s primary diagnosis was a non-ADI for 73.9% (51 of 69) of patient admissions and an ADI for 26.1% (18 of 69) of patient admissions. Pneumonia (27.8%; 5 of 18) and pneumonia due to Pneumocystis carinii (22.2%; 4 of 18) accounted for half of the ADIs. Based on the ICD-9-based classification groups, 34 the most common primary diagnoses were classified as infectious and parasitic diseases (23.2%; 16 of 69). However, 25.0% (4 of 16) of the infectious and parasitic diseases were diseases of the respiratory system (14.5%; 10 of 69; eg, pneumonia due to P carinii), making diseases of the respiratory system the most common primary diagnoses. Other common primary diagnoses were classified as diseases of the nervous system and sense organs (7.2%; 5 of 69), diseases of the circulatory system (7.2%; 5 of 69), and injury and poisoning (7.2%; 5 of 69).
Sample Primary Diagnoses.

Abbreviations: ADI, AIDS-defining illness; CDC, US Centers for Disease Control and Prevention.
Table 3 presents the comorbidities of the total sample, physical therapy subgroup, and nonphysical therapy subgroup. The physical therapy subgroup had a mean (SD) total number of comorbidities of 8.28 (4.09), with a range from 1 to 19. Based on the ICD-9-based classification groups, 34 the most common comorbidities were classified as infectious and parasitic diseases (63.8%, 44 of 69). In all, 2.3% (43 of 69) of patient admissions incurred one or more diagnosis in the endocrine, nutritional and metabolic diseases, and immunity disorders classification group and 56.5% (39 of 69) of patient admissions incurred one or more diagnosis in the mental disorders classification group.
Sample Comorbidities.

Abbreviations: ICD-9, International Classification of Disease, Ninth Revision.
aMean ± standard deviation.
bNumber (percentage) of patient admissions with one or more than one discharge diagnosis within a specified classification group.
Table 4 presents the hospitalization characteristics of the total sample, physical therapy subgroup, and nonphysical therapy subgroup. On nursing assessment of the physical therapy subgroup, 27.5% (19 of 69) of the patient admissions required assistance with bed mobility, 42.0% (29 of 69) of the patient admissions required assistance with transfers, and 46.4% (32 of 69) of the patient admissions required assistance with ambulation. The mean (SD) length of stay for patient admissions was 16.54 (11.4) days, with a range from 2 to 55 days. Patient admissions were discharged to home (33.3%; 23 of 69), home with health care services (13.9%; 10 of 69), an inpatient facility (37.7%; 26 of 69), or other (15.5%; 10 of 69).
Sample Hospitalization Characteristics.

aMean ± standard deviation.
bIn chi-square test, 1 cell (12.5%) had an expected count less than 5.
Impairments and Functional Limitations of the Physical Therapy Subgroup
Table 5 presents the impairments and functional limitations of the physical therapy subgroup. On physical therapy initial evaluation, the mean (SD) total number of impairments and functional limitations for patient admissions was 2.2, with a range from 1 to 5. The majority of patient admissions presented with decreased ambulation status (50.7%; 35 of 69). Other common impairments and functional limitations included decreased function/mobility (40.6%; 28 of 69), decreased strength (31.9%; 22 of 69), decreased endurance (24.6%; 17 of 69), decreased transfer status (20.3%; 14 of 69), and pain (13.0%; 9 of 69).
Impairments and Functional Limitations of the Physical Therapy Subgroup.
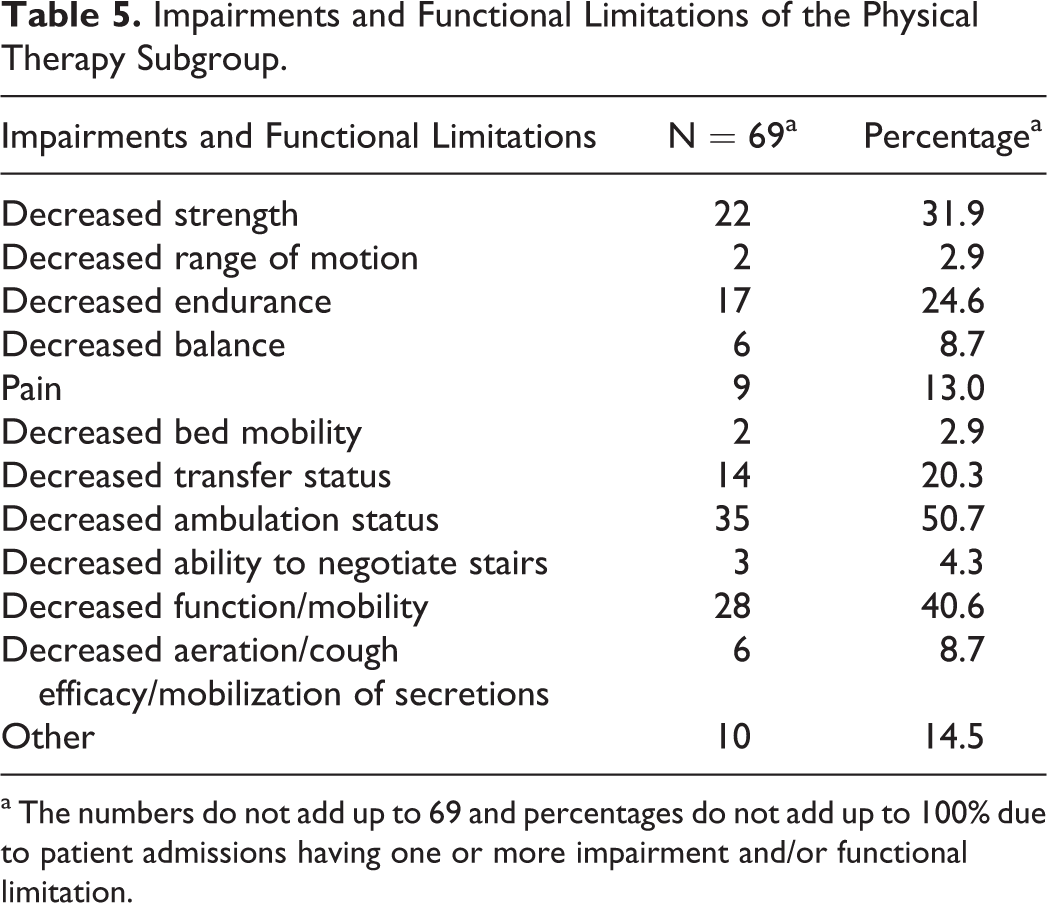
aThe numbers do not add up to 69 and percentages do not add up to 100% due to patient admissions having one or more impairment and/or functional limitation.
Differences between the Physical Therapy Subgroup and the Nonphysical Therapy Subgroup
There were several differences in demographic characteristics, diagnoses, and hospitalization characteristics between the physical therapy subgroup and the nonphysical therapy subgroup. The last columns of Tables 1–4 present the results (P values) of the chi-square tests and t tests.
Differing demographic characteristics between the physical therapy subgroup and nonphysical therapy subgroup included age and race (Table 1). The mean (SD) age of the physical therapy subgroup was older than that of the nonphysical therapy subgroup (48.3 years vs 44.92 years, P= .009). The racial profile of the physical therapy subgroup had a larger percentage of black patient admissions (65.2% vs 48.8%) and a smaller percentage of other race patient admissions (7.2% vs 18.5%) than that of the nonphysical therapy group (P = .036).
The physical therapy subgroup and the nonphysical therapy subgroup had similar percentages of patient admissions with a primary diagnosis of an ADI (26.1% vs 20.0%, P = .264; Table 2). However, the physical therapy subgroup had a larger percentage of patient admissions with a primary diagnosis of an infectious and parasitic disease (23.2% vs 11.8%), disease of the nervous system and sense organs (7.2% vs 1.5%), disease of the skin and subcutaneous tissue (5.8% vs 1.7%), and disease of the musculoskeletal system and connective tissue (5.8% vs 0.7%), in comparison with the nonphysical therapy subgroup (Table 2). The physical therapy subgroup had a smaller percentage of patient admissions with a primary diagnosis of a mental disorder (2.9% vs 14.8%), disease of the respiratory system (14.5% vs 23.4%), and disease of the digestive system (4.3% vs 9.1%), in comparison with the nonphysical therapy subgroup (Table 2). The mean (SD) total number of comorbidities in the physical therapy subgroup was more than that of the nonphysical therapy subgroup (8.28 vs 5.39, P = .000; Table 3). The physical therapy subgroup had a larger percentage of patient admissions with one or more diagnoses in 13 of the 18 ICD-9-based classification groups, 34 in comparison with the nonphysical therapy subgroup (Table 3).
Differing hospitalization characteristics between the physical therapy subgroup and the nonphysical therapy subgroup included all functional status on admission measures, length of stay, and discharge disposition (Table 4). The physical therapy subgroup in comparison with the nonphysical therapy group had a smaller percentage of patient admissions independent and a larger percentage of patient admissions require assistance on all 4 functional status measures bed mobility (62.3% vs 77.8%, 27.5% vs 9.6%, P = .000), transfers (47.8% vs 75.4%, 42.0% vs 11.8%, P = .000), ambulation (42.0% vs 72.9%, 46.4% vs 13.8%, P = .000), and summary (43.5% vs 73.6%, 47.8% vs 14.5%, P = .000). The mean (SD) length of stay of the physical therapy subgroup was longer than that of the nonphysical therapy subgroup (16.54 days vs 6.11 days, P= .000). The physical therapy subgroup in comparison with the nonphysical therapy subgroup, had a larger percentage of patient admissions discharged home with health care services (14.5% vs 6.9%) and to an inpatient facility (37.7% vs 6.7%) and a smaller percentage of patient admissions discharged home (33.3% vs 63.8%; P = .000).
Predictors of Receipt of Physical Therapy
Table 6 presents the results of the multivariable logistic regression analysis. The Hosmer-Lemeshow test was not significant (P = .599), indicating that the logistic regression model adequately fit the data. Factors identified as predictors of receipt of physical therapy were functional status on admission and length of stay (odds ratios (OR) significantly greater than 1.00). Relative to being independent with all assessed functional tasks, requiring assistance with any of the 3 functional tasks increased the odds of receiving physical therapy roughly 4-fold (OR = 4.34). Relative to a length of stay <8 days, a length of stay
Determinants of Receipt of Physical Therapy.

Abbreviation: CI, confidence interval.
Discussion
The Institute of Medicine defines access to health care as “the timely use of personal health services.” 35 As PLWHA are living longer 36 and experiencing greater disability,8–10 accessing health care, in particular physical therapy, may significantly impact their quality of life. 22
This study examined PLWHA that accessed physical therapy after admission to an acute-care hospital. It is useful to begin with a discussion of the manner by which physical therapy was accessed.
In this study, 28.2% (134 of 475) of the total patient admissions received a doctor’s order for physical therapy. Although this referral rate is similar to the 22.4% of patient admissions (all diagnoses) to acute-care hospitals in North Carolina that received physical therapy, 37 it seems low given the prevalence of impairments in PLWHA.8–10 In a sample of persons living with HIV in British Columbia, 8 91.5% reported at least 1 impairment, 80.6% reported at least 1 activity limitation, and 93.2% reported at least some level of participation restriction. In samples of patients with HIV infection in Brazil, 91% were found to have some degree of functional impairment 9 and 85% reported impaired physical activity. 10
Of the 134 patient admissions that received a doctor’s order for physical therapy, 77.6% (104 of 134) did receive and 22.4% (30 of 134) did not receive a physical therapy initial evaluation. There are several potential reasons for patient admissions not having received a physical therapy initial evaluation, including but not limited to the patient being medically unstable, prioritized less during physical therapy triage, not available, or discharged. In addition, it is possible that some physical therapists have a bias against working with patients with HIV infection. In a sample of physical therapists in Nigeria, 23 22% reported that they were unwilling or unsure about working with patients with HIV infection. In a sample of rehabilitation professionals in Canada, 11 27% reported that they were unwilling and 46% were unsure about working with patients with HIV infection.
Of the 104 patient admissions that did receive a physical therapy initial evaluation, 66.3% (69 of 104) were not discharged from physical therapy upon initial evaluation and 33.7% (35 of 104) were discharged from physical therapy upon initial evaluation. Inappropriate referrals, either for patients who should have physical therapy delayed until a later date or who do not require physical therapy, result in an inefficient use of resources. A closer examination of the data collection forms from the 35 patient admissions that were discharged from physical therapy upon initial evaluation revealed 18 discharged with no reason recorded, 15 discharged because of “no need” for physical therapy, and 2 discharged because of discharge home on the same day of the physical therapy initial evaluation.
Ultimately, only 14.5% (69 of 475) of the total number of patient admissions received physical therapy. Identified predictors of receipt of physical therapy included functional status on admission and length of stay, both indicators of illness severity. Longer length of stay was also found to be associated with receipt of physical therapy in patients with stroke and joint replacement in acute-care hospitals in North Carolina. 37
Based on the prevalence of impairments in PLWHA8–10 and the rates of referrals to physical therapy, physical therapy initial evaluations, and receipt of physical therapy in patients with HIV infection in this study, it is possible that a number of patients with HIV infection that could have benefitted from receipt of physical therapy were unable to access physical therapy. The demographic, diagnostic, and hospitalization characteristics of the patient admissions that received physical therapy were determined and are discussed relative to other populations in the following paragraphs.
This study’s physical therapy subgroup had a mean age of 48.3 years, consisted of more men than women, and was predominately black, with public health insurance. In comparison to the nonphysical therapy subgroup, the physical therapy subgroup was older and had a different racial profile. However, multivariable logistic regression analysis revealed no demographic characteristics as predictors for receipt of physical therapy. In comparison to patients with HIV infection in the United States during the pre-HAART era, 38 this study’s physical therapy subgroup had a mean age of approximately 10 years older (48.3 years vs 38.5 years) and a higher frequency of women (43.5% vs 0.0%). These changes in demographic characteristics over time reflect improvements in life expectancy for PLWHA 36 and trends in mode of HIV transmission, 5 respectively.
In comparison with PLWHA in the surrounding neighborhood, 39 this study’s patient population had a higher frequency of persons greater than or equal to 40 years of age (81.2% vs 64.9%), women (43.5% vs 26.6%), and persons who identified themselves as black (65.2% vs 40.7%). In a multistate cohort of patients with HIV infection, 40 higher crude hospitalization rates were also found for persons greater than or equal to 40 years of age, women, and persons who identified themselves as black. In comparison with the national acute-care patient population (all diagnoses) that received physical therapy, 41 this study’s physical therapy subgroup had a higher frequency of men (56.5% vs 42.4%), persons less than 65 years of age (92.8% vs 34.5%), and persons with Medicaid as their primary insurance (60.9% vs 9.86%).
It has long been recognized that in their scope of practice, rehabilitation professionals work with patients who suffer from disability resulting from HIV/AIDS and patients who may coincidentally be HIV positive. 42 The majority of this study’s patient admissions, regardless of subgroup, were due to non-ADI primary diagnoses. This finding is consistent with the decrease in hospitalization rates due to ADIs in PLWHA in the United States between 1994 and 2005. 43 The most common primary diagnoses of this study’s patient admissions were diseases of the respiratory system. This finding is consistent with pneumonia being the most common primary diagnosis in patients with HIV infection in the United States between 2000 and 2006. 44 It is interesting to note that the primary diagnoses (non-ADI and ADI) of this study’s patient admissions were distributed among 15 of the 18 ICD-9-CM-based classification groups, 34 reflecting the “clinical” diversity of the patient population.
In comparison to this study’s nonphysical therapy subgroup, the physical therapy subgroup had a larger percentage of patient admissions with a primary diagnosis of a disease of the nervous system and sense organs, disease of the skin and subcutaneous tissue, and disease of the musculoskeletal system and connective tissue. These classification groups represent 3 of the 4 categories of conditions under which the American Physical Therapist Association has developed preferred physical therapist practice patterns. 45 The preferred physical therapist practice patterns, which describe the elements of patient management that are provided by physical therapists, are applicable to the management of HIV/AIDS disability.
Not only was the mean total number of comorbidities in the physical therapy subgroup significantly more than that of the nonphysical therapy subgroup, also the physical therapy subgroup had a larger percentage of patient admissions with one or more diagnosis in 13 of the 18 ICD-9-based classification groups. 34 These results highlight the greater illness severity in the physical therapy subgroup. The most common comorbidities in the physical therapy subgroup were classified as infectious and parasitic diseases, endocrine, nutritional, and metabolic diseases, and immunity and mental disorders. The endocrine, nutritional, and metabolic diseases and immunity disorders classification group includes diabetes mellitus and the manifestations of diabetes mellitus. 34 The incidence of diabetes mellitus increases in PLWHA with cumulative exposure to combination antiretroviral therapy. 46 Physical therapists play a role in the prevention and treatment of several manifestations of diabetes mellitus. The mental disorders classification group includes psychoses, personality disorders, and substance abuse. 34 There is a high prevalence of mental disorders 47 and co-occurring mental disorders 48 (ie, mood disorder and substance abuse disorder) in PLWHA. It is important that education pertaining to mental disorders and the unique challenges of working with patients with mental disorders be included in HIV/AIDS rehabilitation curricula.
The nursing admission assessments and the physical therapy initial evaluations were in close agreement, both finding functional limitations common among this study’s physical therapy subgroup. Based on the nursing admission assessments, the physical therapy subgroup had a smaller percentage of independent patient admissions and a larger percentage of patient admissions require assistance on all functional status on admission measures, in comparison with the nonphysical therapy subgroup. Based on the physical therapy’s initial evaluations, 50.7% had a decreased ambulation status, 40.6% had decreased function/mobility, and 20.3% had a decreased transfer status. It is likely that the common impairments, such as decreased strength, decreased endurance, and/or pain were contributing factors to the functional limitations. The identified impairments and functional limitations are not unique to patients with HIV infection. Their impairments can significantly impact quality of life and are within the scope of physical therapy practice.
In comparison with the samples of patients with HIV infection in Brazil,9,10 this study’s physical therapy subgroup had a higher prevalence of decreased ambulation status but a similar prevalence of decreased transfer status. This discrepancy between the patient populations’ ambulation status may be due to differences in functional assessments, study time periods, and/or health care between the 2 countries. Although the demographic and diagnostic characteristics of patients with HIV infection have changed in the United States since the pre-HAART era, the impairments and functional limitations have remained similar. Patients with HIV infection in the United States during the pre-HAART era commonly presented with functional deficits 38 and impaired mobility, generalized deconditioning, and pain. 49
The mean length of stay of this study’s physical therapy subgroup was more than 2.5 times longer than the mean length of stay of this study’s nonphysical therapy subgroup and more than 3.5 times longer than the mean length of stay of the national acute-care patient population (all diagnoses). 41 This study’s physical therapy subgroup was more than 3.5 times as likely to require assistance at discharge, in comparison with this study’s nonphysical therapy subgroup, and more than 2 times as likely to require assistance at discharge, in comparison with the national acute-care patient population (all diagnoses). 41 These differences reinforce other findings that suggested a greater severity of illness and prevalence of impairments and functional limitations among this study’s physical therapy subgroup.
In the years following data collection, researchers have demonstrated an association between HIV infection and premature frailty.50–57 Frailty is defined by the presence of at least 3 of the following characteristics: weight loss, exhaustion, low physical activity, weakness, and slow walking time. 58 The prevalence of frailty in PLWHA ranges from 5% to 60%,50–57 depending on study population and/or methodology. In comparison with nonfrail PLWHA, frail PLWHA have greater impairments in physical performance, peak oxygen uptake, functional status, walking speed, balance, and muscle quality 57 ; have higher body mass index and fat mass 57 ; and are at an increased risk of falls. 59 Frail PLWHA have greater comorbidity, higher rates of nonelective hospitalization, and longer inpatient admissions. 52 Predictors of frailty in PLWHA include low CD4 count, longer duration of HIV infection, clinical AIDS, and increased age.50–51,53–56
By 2015, more than half of PLWHA in the United States will be
Limitations
The results of this study should be considered with an awareness of its limitations. The retrospective design allows for potential bias. It is possible that the examining clinicians (ie, physicians, nurses, physical therapists) misinterpreted the patient’s actual condition (ie, diagnoses, functional status, impairments, and functional limitations), data were inaccurately entered into the medical records, and/or data were inaccurately abstracted from the medical records. However, given the “clinical” diversity of the patient population, it is unlikely that the diagnoses were biased toward certain ICD-9-based classification groups. 34 In addition, the close agreement between the nursing admission assessments and the physical therapy initial evaluations pertaining to functional status indicates a high degree of accuracy. The external validity of this study’s results may be limited because of the study setting and time period, as all patient admissions occurred in an acute-care hospital in a large academic medical center in New York City during 2004. However, the majority of PLWHA in the United States reside in urban areas, 62 with New York City having the highest number of reported AIDS cases. 1 Furthermore, the clinical course of HIV/AIDS has not changed considerably since 2004, with the rate of hospitalizations stabilized and comorbidities continuing as the most common cause for admission. 63 Despite these limitations, this study represents a sample of PLWHA that accessed physical therapy after admission to an acute-care hospital in New York City and is a first attempt at describing this population during the HAART era.
Conclusion
Since Galantino and McReynolds 64 described PLWHA referred for outpatient physical therapy services in Texas during the pre-HAART era, there had been no studies aimed at describing patients with HIV infection that receive physical therapy. In this study, patient admissions with HIV infection that received physical therapy had a mean age of 48.3 years, consisted of more men than women, and were predominately black, with public health insurance. The majority of these patient admissions were due to non-ADI primary diagnoses, commonly classified as diseases of the respiratory system, and accompanied by roughly 8 comorbidities. These patient admissions most often presented with functional deficits, decreased strength, decreased endurance, and/or pain. These impairments and functional limitations likely contributed to the population’s prolonged length of stay and need for assistance at discharge. Predictors of receipt of physical therapy were functional status on admission and length of stay.
Further research should examine PLWHA that access physical therapy after admission to acute-care hospitals throughout New York and the United States. Prospective studies are needed to investigate PLWHA that receive and do not receive physical therapy, to determine their physical therapy needs and whether they are being met. Information regarding the physical therapy needs of PLWHA is of value to the education of students, clinicians, and patients. Ultimately, a better understanding of the role of physical therapists in the management of HIV/AIDS disability has the potential to improve the use of resources, effectiveness of interventions, and patient outcomes.
Footnotes
Acknowledgments
The authors gratefully acknowledge Sarah Cohen, DPT, Imee Harsuvanakit, DPT, and Candice Meng, DPT, for conducting data collection during the utilization review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This publication was supported by the National Center for Research Resources and the National Center for Advancing Translational Sciences, National Institutes for Health, through Grant Number UL1 RR024156. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.