
Abstract
Nevirapine (NVP) was the first nonnucleoside reverse transcriptase inhibitor (NNRTI) approved for the treatment of HIV infection. NVP can provide safe and efficacious viral suppression for treatment-naive patients and for virologically controlled patients “switching” from other NNRTI or protease inhibitor–based regimens. Formulations allowing once-daily dosing of antiretrovirals can significantly improve regimen adherence, which is important for maintaining virologic control, especially for NNRTI-based regimens with low barriers for genetic resistance. Randomized and controlled clinical trials have established the clinical noninferiority of a new, extended-release formulation (XR) of NVP, in both treatment-naive (VERxVE) and treatment-experienced patients (TRANxITION), where patients already stable on the immediate-release formulation of NVP were safely transitioned directly to NVP XR. As a potentially more convenient once-daily option, NVP XR may improve adherence and reduce the risk of mutant viruses, attendant virologic failure, and the spread of drug resistance.
Keywords
As a class of antiretrovirals (ARVs), nonnucleoside reverse transcriptase inhibitors (NNRTIs) are widely used agents for first regimens and in later “switching” strategies for the treatment of HIV infection. When switching ARV regimens, staying within the NNRTI class is a logical goal to preserve future treatment options or to avoid adverse events (AEs) associated with other ARV classes. 1 Patient adherence is important in maintaining virologic control, especially with NNRTI-based regimens that generally have low genetic barriers to the development of virologic resistance. Overall, once-daily (QD) regimens have been shown to improve patient adherence. 2 Most of the first-line NNRTI-based regimens can now be given QD.
Nevirapine (NVP) is a first-generation NNRTI, with over 1 million patient years of experience and well-established efficacy and safety profiles. 3 As shown by Gathe et al in the VERxVE study, 4 the QD, 400-mg extended-release (XR) formulation of NVP-XR was found to be well tolerated, with efficacy comparable with that of twice-daily (BID) NVP 200 mg reported in treatment-naive individuals. Of additional interest for those who treat HIV disease may be the results from TRANxITION, a study in patients (N = 443) who were stable on the original, BID immediate-release formulation of NVP-IR and then switched to the XR formulation. Results from 24 weeks of follow-up have recently been published 5 and 48-week results were presented at the 10th International Congress on Drug Therapy in HIV Infection. 6
The TRANxITION study examined the efficacy and safety of switching virologically suppressed patients from NVP-IR 200 mg BID to NVP-XR 400 mg QD. 5 HIV-1-infected adults with undetectable viral loads were enrolled, with all patients having received NVP-IR previously for at least 18 weeks—the majority had been receiving NVP-IR for at least 1 year—along with a fixed-dose nucleoside reverse transcriptase inhibitor (NRTI) combination of QD abacavir/lamivudine (ABC/3TC), QD tenofovir/emtricitabine (TDF/FTC), or BID zidovudine/lamivudine. 5 Patients were randomized 2:1 to switch to open-label, QD NVP-XR (n = 295) or continue BID NVP-IR (n = 148). All 443 patients who were randomized and received at least 1 dose of study drug were included in the analysis. 5 Patients were followed for 48 weeks (Table 1).
Disposition of Patients in TRANxITION at 48 Weeks.
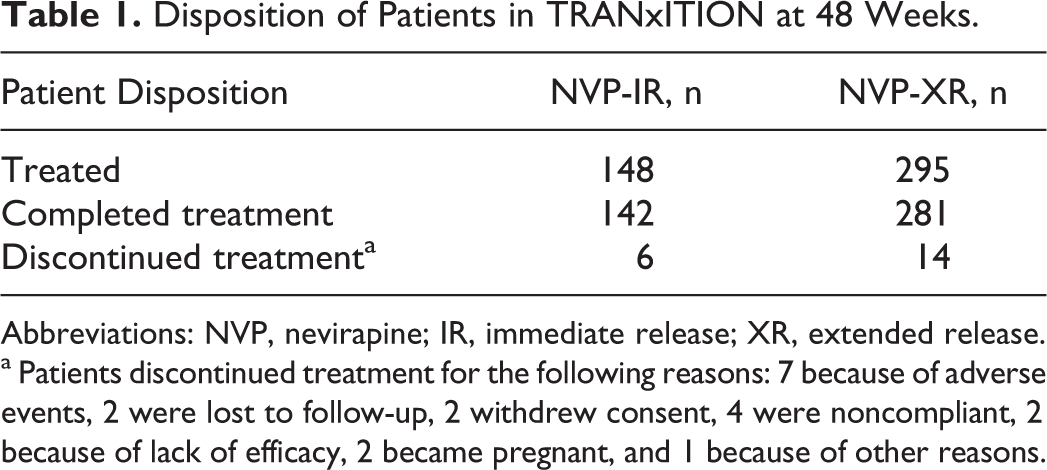
Abbreviations: NVP, nevirapine; IR, immediate release; XR, extended release.
a Patients discontinued treatment for the following reasons: 7 because of adverse events, 2 were lost to follow-up, 2 withdrew consent, 4 were noncompliant, 2 because of lack of efficacy, 2 became pregnant, and 1 because of other reasons.
At baseline, 6% of the patients had HIV-1 RNA copies ≥50 copies/mL, but viral load was undetectable in most patients (280 [94.9%] of 295 patients randomized to the NVP-XR arm and 136 [91.9%] of 148 to the NVP-IR arm). 5 After 24 weeks, virologic suppression continued with both NVP-XR and NVP-IR (276 [93.6%] of 295 and 137 [92.6%] of 148 patients, respectively). 5 Noninferiority of the new formulation was assessed by comparing the lower bound of the 95% confidence interval (CI) for the difference in proportions of virologic response in the 2 treatment arms (NVP-XR minus NVP-IR) with a noninferiority margin of −10%. After adjustment for background therapy, the difference was 1.0% (95% CI: −4.3%-6.0%), indicating NVP-XR was noninferior to NVP-IR. 5 The proportion of patients experiencing division of AIDS (DAIDS) grade 3 or 4 events was similar in the NVP-XR and NVP-IR arms (3.7% vs 4.1%, respectively), although the number of patients reporting any AEs—whether or not defined as possibly drug-related by the treating physician—was greater in the NVP-XR than in the NVP-IR arm, perhaps because of the open-label study design. 5
The rates of AEs for 6 system organ classes that were greater in patients receiving NVP-XR at 24 weeks were followed up at 48 weeks (Table 2). Note that the analysis of the differences in the rates of AEs was limited to AEs considered mild or moderate at 24 weeks because of the very low number of serious AEs in any category. At 48 weeks, virologic response was achieved in 262 of 295 patients treated with NVP-XR and 131 of 148 patients treated with NVP-IR (88.8% vs 88.5%, 0.3% difference; 95% CI: −6.1-6.7). 6 Again, NVP-XR was noninferior to NVP-IR treatment, and this outcome was further supported by consistent results from time to loss of virologic response and snapshot analyses, as defined by the US Food and Drug Administration (FDA).
Adverse Events, by Selected System Organ Class and Intensity at 48 Weeks.a, 6

Abbreviations: NVP, nevirapine; IR, immediate release; XR, extended release; AE, adverse event; GI, gastrointestinal.
a The rate of adverse events (AEs) for 6 system organ classes (SOCs) that demonstrated higher rates in patients receiving NVP-XR at 24 weeks were followed at 48 weeks. These 6 groups do not include all patients with AEs, but highlight the SOC groupings with different AE rates. Note these differences were limited to mild and moderate AEs.
Both IR and XR formulations were well tolerated, with a good overall safety profile; the rate of AEs was lower than that usually seen in treatment-naive patients, 5 as might be expected given that patients had been receiving NVP-IR for a longer period of time (the majority at least 1 year). During the 48-week follow-up, the number of patients experiencing any AE was higher with NVP-XR than with NVP-IR, although the difference between the groups was lower than that seen at week 24. The rates of serious AEs were similar between the 2 treatment arms, 8.1% and 10.2% in the NVP-IR and NVP-XR groups, respectively.
Throughout the study, the proportion of patients experiencing DAIDS grade 3 or 4 events was similar between the NVP-XR and NVP-IR arms (6.4% vs 6.1%, respectively). However, mild and moderate AEs were somewhat higher in the NVP-XR arm (Table 2). Between 24 and 48 weeks of treatment, no NVP-related incidents of hepatic injury or rash were observed. Also, liver transaminase elevation was seen in 4 patients taking NVP-XR (1 patient had hepatitis C infection and discontinued participation and 3 patients continued in the study; Tables 1 and 2). 6
Once-daily NVP-XR (400 mg) was approved by the FDA in March 2011, 3 and its availability expands the number of QD options in the NNRTI class. Although the results from VERxVE trial showed the relative safety and efficacy of this agent in treatment-naive patients, 4 data from TRANxITION support the switch from NVP-IR to NVP-XR in treatment-experienced patients who are virologically suppressed taking NVP-IR. 6 Indeed, for these patients, the improved dosing regimen may make the reformulated agent more convenient and compatible with other QD regimen components, such as recommended fixed-dose combinations of NRTIs.
Patients who started treatment regimens with a higher pill burden or more frequent dosing requirements may be good candidates for regimen simplification, as recommended by the 2012 US Department of Health and Human Services (DHHS) HIV Treatment Guidelines. 1 Evidence from studies of simplified regimens suggests that adherence is likely to be improved with these regimens. A meta-analysis of 11 randomized, controlled trials comparing QD and BID ARV regimens reported that adherence improved with QD regimens, without compromising efficacy. 2 Improving adherence levels is a particularly important issue for patients receiving ARVs, because nonadherence can lead to treatment failure, selection of mutant viruses (especially among patients receiving a regimen other than a boosted protease inhibitor), and spread of drug resistance. The benefits of simplified regimens have also been demonstrated in disadvantaged HIV-infected populations such as the homeless and marginally housed. 7
According to the current prescribing guidelines, adults already established on a regimen of NVP-IR (200 mg BID) can be switched to NVP-XR (400 mg QD) with no half-dose, lead-in period. Per the product label, the lead-in period is required only for those starting therapy with NVP de novo. 3 Those patients should initiate therapy with a single 200-mg tablet of NVP-IR QD for the first 14 days, followed by a 400-mg tablet of NVP-XR QD. If a patient experiences a rash during the 14-day lead-in period with NVP-IR, this formulation can be continued up to 28 days, based on clinical evaluation of the severity, and NVP-XR should not be started until the rash has resolved. However, if dosing is interrupted for more than 7 days for any reason, the patient should restart therapy with the 14-day lead-in dosing of NVP-IR 200 mg/d. 3
The DHHS HIV Treatment Guidelines 1 also recommend that the patients should be monitored after switching treatment regimens, advising that the patients should be evaluated 2 to 6 weeks after treatment simplification in order to assess tolerance and for appropriate clinical monitoring (eg, HIV vial loads and liver function tests). Cholesterol subsets and triglycerides should be assessed (fasting) within 3 months of the change in therapy. If there are no specific complaints, laboratory abnormalities, or viral rebound at 3 months, the patient may return to regularly scheduled clinical and laboratory monitoring. 1
In conclusion, by providing a potentially more convenient QD option for patients, NVP-XR may improve adherence over the long term, thereby reducing the risk of virologic failure, selection of mutant viruses, and the spread of drug resistance. Clinical studies have demonstrated safety and efficacy in combination with standard NRTI regimen components, including QD, fixed-dose combinations such as TDF/FTC or ABC/3TC. 4 - 6
Footnotes
Acknowledgments
The authors were fully responsible for all content and editorial decisions, were involved at all stages of manuscript development, and have approved the final version of this brief communication that reflects the authors’ interpretation and conclusions. Medical writing assistance, supported financially by Boehringer Ingelheim, was provided by Linda Merkel and Geraldine Thompson of Envision Scientific Solutions, during the preparation of this manuscript. Boehringer Ingelheim was given the opportunity to check the data used in the manuscript for factual accuracy only.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: As a clinical trial investigator, Dr Ward receives research funding from Boehringer Ingelheim, the manufacturer of Viramune (nevirapine).