
Abstract
Vulvitis circumscripta plasmacellularis or Zoon vulvitis is a rare benign condition that affects the vulva chronically. We herein report a case of Zoon vulvitis in a 52-year-old HIV-infected patient with an uncommon ulcerovegetating lesion diagnosed by histopathlogic findings. The patient was treated with clobetasol propionate ointment and oral corticosteroid. Zoon vulvitisis is a rare vulvar disorder that offers a challenging diagnose and therapy. The patient was appropriately treated and remains disease free.
Introduction
In the 1950s, Zoon described a chronic inflammation of the glans penis or inner surface of the foreskin which was named balanitis chronica circumscripta plasmacellularis. 1 Vulvitis circumscripta plasmacellularis, also called Zoon vulvitis, is a rare benign condition that affects the vulva chronically. Zoon vulvitis pathophysiology remains unknown.
Zoon considered the presence of a plasmacellular infiltrate a mandatory criterion for a proper diagnosis. 1 Diagnosis of Zoon vulvitis has become a challenge because of its resemblance to other infectious and neoplastic disease. Being clinically similar to malignancies, the best method of diagnosis is a biopsy. 2 The therapeutic response may vary and may be prolonged for years, with some cases of recurrence. We herein describe a very atypical, exuberant case of ulcerative Zoon vulvitis in an HIV-infected woman.
Case Report
A 52-year-old mulatto woman, married, artisan, HIV-positive for about 3 years, residing in the city of Vila Velha-Espirito Santo, Brazil, was referred by her infectologist to the gynecology service of a private clinic because of “the presence of an extensive, itchy wound in the genitals” that had been present for 6 months.
She had previously undergone an incisional biopsy that histopathology described as a nonspecific chronic inflammatory process. She was prescribed, after biopsy, the use of azithromycin, topical steroids, ciprofloxacin, and oral acyclovir for 10 days, which did not provide any clinical improvement of the lesion.
During anamnesis, the patient declared having 2 children, and a steady exclusive partner who tested sero-negative for HIV, with no possibility of intercourse because of genital lesions. She denied any previous pathologies and history of neoplasia or cervical pathology or autoimmune disease in the family. She also denied the use of illicit drugs, smoking, and alcohol.
Regarding her clinical follow-up for HIV infection, she reported to be undergoing highly active antiretroviral therapy (HAART) since early diagnosis that occurred 3 years before (zidovudine [ZDV], lamivudine [3TC], and lopinavir/ritonavir [LPV/r]) when she presented with Herpes zoster, community-acquired pneumonia, and lymphocyte count of 260 CD4 cells/mm3. She still keeps the same regimen in force.
We observed, during gynecological examination, the presence of a granulomatous, vulvar ulcer with elevated borders and with necrotic background, associated with abundant exudate involving a large part of the right labia majora and lower left vaginal wall (Figure 1A). The patient also had painless itching associated with the lesions.

A, Vulvar ulcer with elevated borders and with necrotic background associated with abundant exudate. B, Vulva with lesion regression.
The sample collected and stained with Giemsa and Gram stains did not indicate donovanosis and/or other bacterial infections; however, a therapeutic trial with doxycycline 200 mg/d was performed, with the lesion progressing with severe exacerbation. At the same time, a new biopsy was performed which showed a histopathologic image compatible with the dense plasma cell inflammatory infiltrate with focal atrophy and erosion of the epidermis suggestive of Zoon vulvitis (Figure 2).
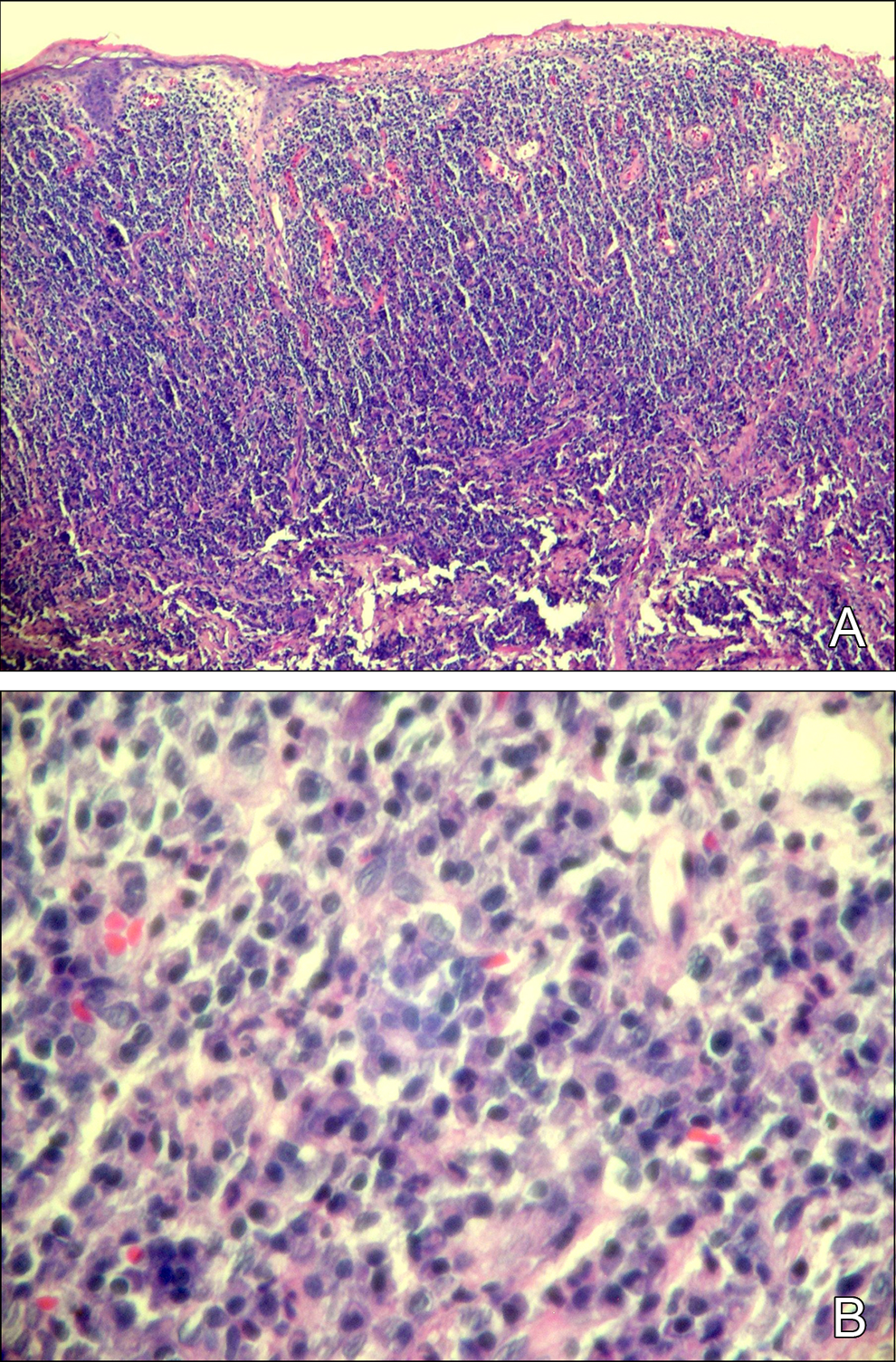
A, Intermediate power view dense plasmacytic inflammatory infiltrate with epidermal focal erosions and hypotrophy (hematoxylin and eosin [H&E] ×100). B, Lower power view of dense plasmacytic inflammatory infiltrate (H&E ×40).
The patient was treated with clobetasol propionate ointment 0.05% 3 times a day for 2 weeks with a discrete improvement at which point the patient was administered oral corticosteroid (betamethasone 6 mg/d) with decreasing dosage every 15 days for about 2 months with marked improvement in the lesion along with its disappearance in 21 days (Figure 1B). At this point, we returned to the ointment applied once a day for 3 more months. Now she is recovered and disease free, 18 months after diagnosis. Currently the patient is undergoing 1-year follow-up in gynecology, dermatology, and infectious diseases services.
During diagnosis, Venereal Disease Research Laboratory screening tests were performed and repeated with 7 and 14 days of clinical follow-up, with negative results and normal blood count. At that time, the patient also presented with a lymphocyte count of 1153 CD4 cells/mm3 and an undetectable viral load, under the same regimen of HAART.
Discussion
In 1952, Johannes Jacobus Zoon, a German dermatologist, 1 diagnosed a chronic inflammation of the penis glans or its inner surface of the foreskin, resembling erythroplasia of Queyrat, but with an infiltrate of plasma cells present in the histological findings. 3 In 1955, Zoon described 2 cases with similar clinical and histological aspects in the vulva. 1 The affection of the vulva is a rare disorder with hemosiderin deposits often found, most likely caused by a reaction of the vulvar mucosa after injury, trauma, or general infection. 4 However, there have been no reports of malignant transformation of these lesions. 1
Zoon vulvitis may preferentially affect the age group between 26 and 70 years, without, however, affecting prepuberal women. 3 Our patient’s age is compatible with what is described in the medical literature.
In general, the lesions are asymptomatic and may remain unnoticed by the patient for some years. However, some patients may complain of itching, burning sensation, and dyspareunia, 1 perineal pain, increased sensitivity, 1 dysuria, 5 and scaling. 2 Our patient presented an extended lesion with mild burning sensation and pain symptoms, though with great discomfort due to the presence of genital lesions and associated pruritus.
Lesions often clinically present themselves as well-defined, non-infiltrated erythematous plaques that are bilateral and symmetrical, tending to confluence. The presence of hemosiderin deposits, telangiectasias, and purples give a red or dark aspect to the ecchymotic lesions. 3 Lesions may vary in color from yellow to orange with red dots known as cayenne pepper. 5 In less frequent cases, it can be erosive lesions or granulomatous as noted in this report. The lesions can be found in the small and large labia, clitoris, urethral meatus, posterior fourchette, and vaginal channel. 3,5 The patient in this study had extensive granulomatous lesion that occupied much of the large lip and right lower portion of the left vagina with abundant exudate.
Regarding its differential diagnosis, Zoon vulvitis may “resemble” Paget disease, pemphigus vulgaris, lichen planus, allergic contact dermatitis, syphilis, genital herpes, chancroid, lymphogranuloma venereum, infection with HIV, Crohn disease, systemic lupus erythematosus, Bechet disease, infection with Mycobacterium tuberculosis, 1 Queyrat erythroplasia, 3 and even intraepithelial vulvar neoplasia. 2 Thus the biopsy becomes essential for proper diagnosis, 1 as it has happened with our patient.
The histopathologic findings may point to atrophic epidermis, a decrease in keratinocyte both in number and in size, thinner epidermal layer having espondiose between the layer and the epidermal keratinocytes. It also presents dense lichenoid infiltrate with a predominance of plasma cells (more than 50%). Lymphocytes and mast cells may be also present. The vessels are dilated, facilitating extravasation of erythrocytes and deposition of hemossiderina. 1,5 The histopathological lesions of the patient in this study showed dense plasmacytic inflammatory infiltrate with focal atrophy and erosion of the epidermis confirming the diagnosis suggestive of Zoon vulvitis.
Various forms of treatment of Zoon vulvitis were proposed with different results. Symptoms may disappear, however, the injury may remain. 5 Therapeutic options include estrogen, corticosteroids (topical or systemic), antifungals, antibiotics, nerve block flow, fulguration, laser abrasion, cryotherapy, interferon, etretinate, and surgical excision. 1
Our patient received clobetasol propionate ointment as well as oral corticosteroid therapy with a remarkable response. In this context, the establishment of a proper clinical history and biopsy are essential to ensure appropriate treatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.