
Abstract
Cholesterol crystal embolism (CCE) is an underdiagnosed systemic condition that often leads to acute kidney injury (AKI) with poor kidney prognosis. Herein, we report a case of dialysis-dependent AKI due to spontaneous CCE with early kidney recovery. A 76-year-old man with hypertension, diabetes mellitus type 2, chronic hepatitis B virus, adrenal insufficiency and gout presented with fatigue, polyarthritis, oliguria, and elevated serum creatinine. Imaging revealed an infrarenal abdominal aortic aneurysm with diffuse atherosclerosis, and laboratory findings showed markedly elevated D-dimer without eosinophilia or autoantibodies. Despite supportive measures, kidney function deteriorated rapidly, necessitating urgent initiation of intermittent hemodialysis on 4 occasions during the first week. Kidney biopsy confirmed cholesterol clefts within medium-sized arteries, establishing the diagnosis of CCE. The patient was treated with corticosteroids, high-dose statins, aspirin, and supportive therapy. Remarkably, kidney function improved, allowing discontinuation of dialysis by the end of the first week, and he was discharged on day 22 with significant recovery of kidney function. In conclusion, CCE-related AKI is rare and typically associated with poor outcomes, yet this case demonstrates that early recognition, timely kidney biopsy, and prompt initiation of corticosteroids and high-dose statins may enable full kidney recovery.
Introduction
Cholesterol embolism, also called cholesterol crystal embolism (CCE) or atheroembolism, is a systemic condition caused by the release of cholesterol crystals originating from atherosclerotic plaques in major arteries such as the aorta and iliac vessels. 1 These crystals migrate distally and obstruct small- to medium-sized arterioles, leading to localized ischemia and a pronounced inflammatory reaction. 2 The kidneys, skin, gastrointestinal tract, and central nervous system are most commonly affected. 1
Cholesterol embolism often develops following thrombolytic therapy, arterial interventions, or major vascular surgeries involving the aorta or heart, and has historically been considered an iatrogenic condition. 3 However, spontaneous cholesterol embolism, occurring in the absence of recent vascular manipulation, is increasingly recognized, especially in patients with widespread atherosclerosis and other risk factors such as hypertension, smoking, diabetes, and advanced age. 1
The true incidence of cholesterol embolism is likely underestimated due to underdiagnosis and nonspecific clinical presentations. 2 Autopsy studies report an incidence of cholesterol emboli in 2.4% of unselected patients. 4 In patients undergoing angiographic procedures, about 0.38% develop clinically significant cholesterol embolism, confirmed either by histological findings or by the presence of characteristic skin manifestations together with specific blood test results. 5 Spontaneous cases are rarer but carry significant morbidity due to delayed diagnosis and multiorgan involvement. 1
Clinical presentation is highly variable and depends on the organs affected. 1 Common signs include acute or subacute kidney injury, livedo reticularis, blue or purple toes, retinal Hollenhorst plaques, and systemic inflammation with eosinophilia. 1 Diagnosis is often challenging and may be delayed due to nonspecific manifestations. 2 Tissue biopsy remains the gold standard, demonstrating cholesterol clefts within occluded small vessels. 1
Herein, we report a rare case of spontaneous CCE presenting with dependent acute kidney injury (AKI-D), highlighting the importance of early nephrology-focused evaluation in guiding management.
Case Report
A 76-year-old Vietnamese man with a history of hypertension (HTN), diabetes mellitus type 2, chronic hepatitis B virus (HBV) infection, adrenal insufficiency, and gout was admitted to the internal medicine department with a 4-day history of fatigue, polyarthritis, and oliguria. Over the past month, he had developed progressive pain and swelling in the small joints of both hands and feet. He reported no fever, rash, chest pain, dyspnea, abdominal pain, hematuria, or skin discoloration such as livedo reticularis or digital ischemia. He denied any history of smoking, alcohol consumption, or intravenous drug use. No family history of kidney, cardiovascular, or autoimmune disorders was reported. At home, he had been taking telmisartan, rosuvastatin, clopidogrel, allopurinol, prednisolone, diacerein, silymarin, esomeprazole, and vitamin B supplements for the management of comorbidities, without the use of any over-the-counter or herbal medications.
On admission, vital signs were stable: blood pressure 140/80 mmHg, heart rate 78 beats/minute, and temperature 37°C. Physical examination revealed bilateral pitting edema of the lower extremities and swollen, tender, and erythematous small joints of both hands and feet. No skin discoloration, livedo reticularis, or digital ischemia was observed. Laboratory findings are summarized in Table 1. Blood and urine cultures, urine protein-to-creatinine ratio, and anti-glomerular basement membrane and proteinase 3-antineutrophil cytoplasmic antibody (PR3-ANCA) testing were not performed. All other immunologic assays were negative. A serum-free light chain assay was not separately performed.
Laboratory Findings.

Abbreviations: µL, microliter; µmol/L, micromole per liter; ALP, alkaline phosphatase; ALT, alanine aminotransferase; AMA, anti-mitochondrial antibody; ANA, antinuclear antibody; Anti-HBe, antibody to hepatitis B e antigen; aPTT, activated partial thromboplastin time; ASO, anti-streptolysin O; AST, aspartate aminotransferase; Cl−, chloride; CRP, C-reactive protein; dsDNA, double-stranded DNA; g/L, gram per liter; Hb, hemoglobin; HBeAg, hepatitis B e antigen; HBsAg, hepatitis B surface antigen; HBV, hepatitis B virus; HCT, hematocrit; HDL, high-density lipoprotein; INR, international normalized ratio; K+, potassium; LDH, lactate dehydrogenase; LDL, low-density lipoprotein; LKM-1, liver-kidney microsomal antibody type 1; mmol/L, millimole per liter; MPO, myeloperoxidase; Na+, sodium; PLT, platelet; PT, prothrombin time; RBC, red blood cell; RF, rheumatoid factor; SG, specific gravity; SMA, smooth muscle antibody; WBC, white blood cell.
Doppler ultrasound of the lower extremities revealed scattered atherosclerotic plaques without thrombosis. Abdominal ultrasound showed an infrarenal abdominal aortic aneurysm with extensive wall calcification and severe atherosclerosis. The patient was transferred to the nephrology unit with a provisional diagnosis of acute tubular necrosis, later revised to cholesterol embolism syndrome (CES) based on clinical suspicion and predisposing factors, including advanced age, diffuse atherosclerosis, and multiple comorbidities. Although the patient had advanced atherosclerosis and presented with acute kidney injury (AKI), the absence of peripheral eosinophilia, livedo reticularis, and a recent vascular procedure made the diagnosis of CES challenging. Initial consideration included acute tubular necrosis and vasculitis, requiring a kidney biopsy for definitive diagnosis.
Prior to the initiation of CCE-specific therapy, the patient received intravenous methylprednisolone 40 mg daily, along with supportive medications including proton pump inhibitors, sucralfate, paracetamol, and tramadol. Chronic medications for comorbid conditions included clopidogrel, low-dose rosuvastatin, amlodipine, vildagliptin/insulin, magnesium and vitamin B supplements, and entecavir for chronic hepatitis B.
On the second hospital day, kidney function worsened significantly (creatinine 519 µmol/L and urea 28.9 mmol/L), accompanied by progressive oliguria, prompting urgent initiation of hemodialysis. The patient underwent 4 sessions of intermittent hemodialysis on hospital days 2, 4, 6, and 7.
Further investigations revealed no immunologic or autoimmune abnormalities. The eosinophil count was not elevated (0.2 × 109/L), and complement levels (C3 and C4) were within normal limits. D-dimer was markedly elevated (>15 000 ng/mL), and the lipid profile showed dyslipidemia consistent with underlying atherosclerosis (Table 1). Viral serology confirmed chronic inactive HBV infection. A kidney biopsy (Figures 1 and 2) performed on hospital day 8 contained 12 glomeruli, of which 3 were globally sclerosed, and the remaining appeared normal. Chronic interstitial inflammation was noted, accompanied by tubular atrophy and interstitial fibrosis involving approximately 30% of the cortical area. Focal acute tubular necrosis with granular casts was observed in some tubules. Medium-sized arteries and arterioles showed cholesterol clefts within the lumen, associated with intimal thickening and severe atherosclerosis. Masson’s Trichrome stain demonstrated concentric intimal fibrosis and collagen deposition consistent with hyperplastic arteriolosclerosis. On immunofluorescence, a weak IgA stain was recorded in the mesangium, otherwise unremarkable. Electron microscopy was not available.

Kidney biopsy (Trichrome × 400). Light microscopy shows concentric intimal fibrosis and collagen deposition consistent with hyperplastic arteriolosclerosis.

Kidney biopsy (H&E × 400). Cholesterol clefts (arrow) are seen within the arterial lumen, accompanied by intimal hyperplasia and severe atherosclerosis. H&E, Hematoxylin and Eosin.
Following histologic confirmation of CES, the treatment regimen was adjusted accordingly. The clinical course during hospital are illustrated in Figure 3. Intravenous methylprednisolone 40 mg daily was continued and subsequently transitioned to oral prednisone. Rosuvastatin therapy was intensified, with the dose increased from 10 mg to 20 mg daily, and low-dose aspirin (81 mg/day) was initiated. Supportive measures, including glycemic control, blood pressure control, and nutritional supplementation, were continued, as were the patient’s chronic medications for comorbid conditions. Hemodialysis was discontinued at day 7 following clinical stabilization and improvement in kidney function (creatinine 291 µmol/L, urea 14.12 mmol/L), along with a progressive increase in urine output exceeding 1500 mL/day, which subsequently stabilized at approximately 2000 mL/day. The patient tolerated all medications well, with no adverse effects or intolerance reported during hospitalization or follow-up.
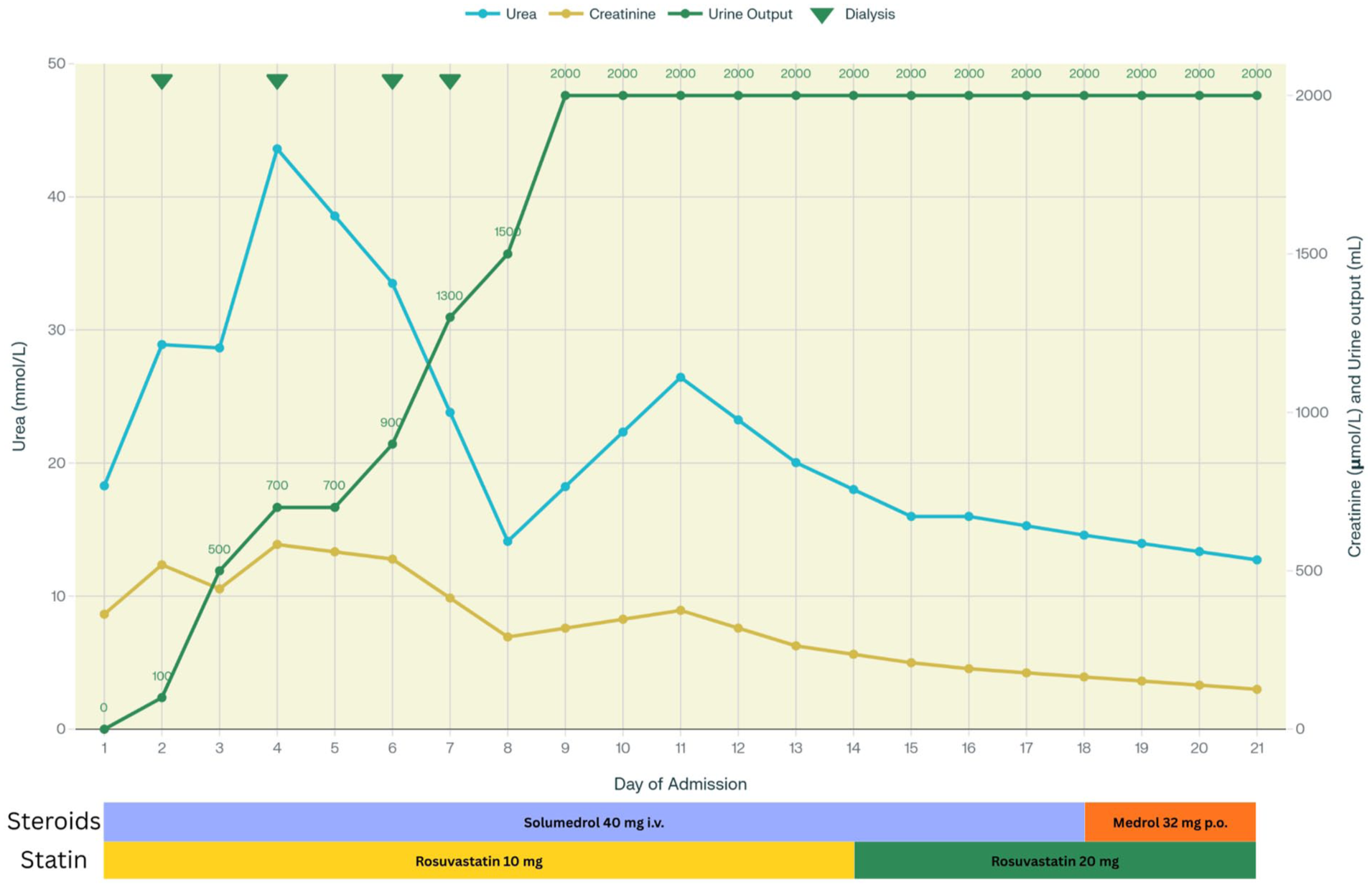
Clinical course during hospitalization. Trends of serum urea, creatinine, and urine output during admission. Green arrows indicate dialysis sessions. Timelines of corticosteroid (methylprednisolone—Solu-Medrol; Medrol) and statin (rosuvastatin) therapy are shown.
He was discharged after 22 days of hospitalization with improved kidney function (creatinine 126 µmol/L, urea 12.73 mmol/L), and a final diagnosis of CES with recovering AKI, along with comorbidities. At discharge, the patient had partial recovery of kidney function. Long-term prognosis remains uncertain, and close outpatient follow-up with periodic kidney function monitoring, cardiovascular risk factor control, and outpatient surveillance was planned.
Literature Review
In this study, 12 cases of CCE or atheroembolic renal disease (AERD) were examined across 3 countries (Turkey, India, and Japan) between 2014 and 2024 (Table 2). The majority of patients were older males (ages 48-80) with common cardiovascular risk factors and comorbidities, including HTN, coronary artery disease (CAD), smoking, diabetes mellitus (DM), and prior endovascular intervention like revascularization. A notable trend was the spontaneous or procedure-related onset of kidney failure or critical limb ischemia secondary to CCE/AERD. Clinically, patients are most frequently presented with signs of target organ ischemia, especially kidney dysfunction (oliguria) and peripheral limbs (toe gangrene). Laboratory findings consistently revealed AKI (elevated creatinine and declined estimated glomerular filtration rate), and in some cases, eosinophilia or elevated Erythrocyte Sedimentation Rate. Imaging often showed increased kidney echogenicity and severe aortic atherosclerosis and calcification. Definitive diagnosis was established by biopsy in nearly all cases, with hallmark findings of cholesterol clefts within small arteries, glomerulosclerosis, and varying degrees of interstitial fibrosis and tubular atrophy. Most patients received statins as a core treatment. Additional therapies included steroids, hemodialysis, and aggressive blood pressure control. Outcomes were variable but severe in most cases: dialysis dependency or amputation. However, partial or full kidney recovery was noted in a few individuals, especially when early diagnosis and supportive care were initiated. Overall, these cases highlight the multisystem impact, diagnostic challenges, and generally poor prognosis of CCE/AERD, emphasizing the need for early recognition and individualized management strategies.
Summary of Reported Cases of CCE and AERD From the Literature.

Abbreviations: ABI, Ankle-Brachial Index; ACEi, Angiotensin-Converting Enzyme Inhibitor; AERD, Atheroembolic Renal Disease; AKI, Acute Kidney Injury; CABG, Coronary Artery Bypass Graft; CAD, Coronary Artery Disease; CCE, Cholesterol Crystal Embolism; CKD, Chronic Kidney Disease; CLTI, Chronic Limb-Threatening Ischemia; CT, Computed Tomography; DM, Diabetes Mellitus; EF, Ejection Fraction; ESR, Erythrocyte Sedimentation Rate; EVT, Endovascular Treatment; HCTZ, Hydrochlorothiazide; HTN, Hypertension; IF, Immunofluorescence; IFTA, Interstitial Fibrosis and Tubular Atrophy; IVUS, Intravascular Ultrasound; LDL, Low-Density Lipoprotein; MI, Myocardial Infarction; NOGA, Nonobstructive General Angioscopy; NSAIDs, Non-Steroidal Anti-Inflammatory Drugs; PTRA, Percutaneous Transluminal Renal Angioplasty; RCCE, Renal Cholesterol Crystal Embolism; RFTs, Renal Function Tests; SFA, Superficial Femoral Artery; SRAPs, Spontaneous Ruptured Aortic Plaques; WIfI, Wound, Ischemia, and Foot Infection Classification; Yrs, Years.
Discussion
CES is a condition involving multiple organ systems, caused by cholesterol crystals lodging in small- to medium-sized arteries, and is most frequently seen in older adults with advanced atherosclerosis. 1 While commonly linked to iatrogenic triggers such as catheterization or surgery, spontaneous CES can occur without recent vascular intervention. 2 A 2018 study employing nonobstructive general angioscopy reported that 80.9% of individuals diagnosed with, or suspected to have, CAD had spontaneous rupture of aortic plaques. 8 This case exemplifies such a presentation in a patient with multiple cardiovascular risk factors, including advanced age, long-standing hypertension, type 2 DM, and an infrarenal abdominal aortic aneurysm with diffuse atherosclerosis. Interestingly, the baseline lipid profile was not markedly abnormal, underscoring that CCE may occur even in the absence of significant dyslipidemia.
Diagnosis is complicated as a wide range of conditions were carefully considered due to its variable and nonspecific clinical features. 2 In this case, subacute kidney injury, systemic inflammation, and absence of clear acute tubular necrosis triggers raised clinical suspicion. The absence of hematuria, proteinuria, or serologic markers (eg, ANCA, anti-dsDNA, and low complement) helped exclude immune-mediated vasculitis and glomerular diseases. Although peripheral eosinophilia and dermatologic signs were absent, markedly elevated D-dimer and imaging evidence of advanced atherosclerosis supported the consideration of CES.9-11 Diagnosis of cholesterol embolization syndrome can be confirmed with certainty only through biopsy. 2 Kidney biopsy is proved to be the gold standard for cholesterol embolization, revealing characteristic cholesterol clefts within occluded vessels. 1
No definitive or specific treatment exists for CES, and management remains largely supportive.1,12,13 Hemodialysis is indicated to manage complications of AKI, such as refractory fluid overload, hyperkalemia, oligoanuria, or severe kidney dysfunction. 1 Statins and aspirin enhance their therapeutic effects by modifying the morphology of cholesterol crystals, potentially reducing their harmful impact. 14 Statins have multiple effects beyond lipid-lowering, including anti-inflammatory, endothelial-protective, and antithrombotic actions. These effects are mediated by reducing tissue factor expression and enhancing thrombomodulin, leading to decreased thrombin generation and platelet activation.15,16 Statins are recommended for plaque stabilization and may improve outcomes, while corticosteroids have shown benefit in some cases, though evidence is mixed and largely based on case reports and small series.17,18
Biopsy-proven CCE generally carries a poor prognosis, with long-term studies showing that nearly one-third of patients progress to end-stage kidney disease requiring chronic dialysis and more than one-third die within 5 years. 9 A recent review further emphasized that severe or multisystem CCE can be associated with mortality rates as high as 60% to 80% within the first year, particularly in patients presenting with AKI-D. 14 Kidney recovery, though possible, is uncommon in this setting; in a cohort of 43 patients, only 28% were able to discontinue dialysis, and most recoveries occurred months after the initial event with a risk of late relapse. 19
In our case, several nephrology-specific decisions may have contributed to the favorable outcome. Hemodialysis was initiated promptly when indicated, and an early kidney biopsy secured the diagnosis and guided targeted management. High-dose intravenous methylprednisolone was started on the first day, when vasculitis had not yet been excluded, although pulse therapy was avoided given the patient’s advanced age and the absence of firm evidence. In addition, statin therapy, a mainstay in both cardiology and nephrology, was also begun promptly. Together, these timely interventions and a kidney-focused management strategy likely accounted for the unusually rapid recovery observed.
Because follow-up was limited to the hospitalization period, the long-term kidney prognosis remains uncertain.
Conclusion
Spontaneous cholesterol embolism is rare but should be considered in elderly patients with diffuse atherosclerosis who present with unexplained AKI, even in the absence of recent vascular intervention. Kidney biopsy remains essential for a definitive diagnosis, and management is mainly supportive, with statins recommended for secondary prevention. Although most dialysis-requiring cases progress to chronic dependence or poor outcomes, this patient’s unusually rapid recovery illustrates how early recognition, biopsy confirmation, and carefully tailored therapy can occasionally alter the expected clinical trajectory. Long-term prognosis, however, remains uncertain.
Footnotes
Author Note
Prior Presentation of Abstract Statement: Not applicable.
ORCID iDs
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series
Consent for Publication
Written informed consent was obtained from the patient for their anonymized information to be published in this article
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.