
Abstract
Inhalation of methanol vapor is a rare but potentially life-threatening occupational hazard, particularly in environments with inadequate ventilation and safety controls. We report the case of an 18-year-old male shrimp processing worker who developed acute respiratory failure following accidental inhalation of methanol vapors mislabeled as kerosene. The patient presented with severe dyspnea, hypoxemia, metabolic acidosis, and radiographic findings of diffuse pulmonary infiltrates. He required mechanical ventilation, corticosteroids, antibiotics, and intensive supportive care. Bronchoscopy revealed erythematous bronchial mucosa with hemorrhagic stippling and was followed by bronchoalveolar lavage (BAL). Based on imaging findings, therapeutic segmental pulmonary lavage (TSPL) was performed, targeting the most affected lower lobe segments. The procedure involved instillation and aspiration of small saline aliquots to remove inflammatory debris. Following TSPL, the patient exhibited marked clinical improvement, with normalization of inflammatory markers and successful extubation within 48 hours. This case illustrates the potential value of TSPL as an adjunctive therapy in methanol-induced chemical pneumonitis. Unlike standard BAL, TSPL enables targeted clearance of toxic exudates from specific lung segments, potentially accelerating recovery in patients with localized airway injury. Given the rarity of inhalational methanol poisoning and the absence of established respiratory interventions beyond supportive care, TSPL may offer a novel approach to managing severe pulmonary complications. This experience highlights the need for heightened clinical awareness of inhalational toxic exposures and further research into therapeutic lavage techniques. Our findings suggest that TSPL could be considered in selected cases of toxic inhalation injury when conventional measures fail to produce timely improvement.
Keywords
Introduction
Methanol, commonly known as wood alcohol, is a volatile and toxic chemical widely utilized in industrial applications, such as cleaning agents, antifreeze, solvents, and fuels. 1 Its accessibility in workplace environments, particularly in industries handling hydrocarbons, renders it a significant occupational hazard. 2 Despite its relatively infrequent occurrence, methanol intoxication is associated with high morbidity and mortality due to its toxic metabolites, primarily formate, which cause severe metabolic acidosis and tissue-specific damage, including respiratory compromise, optic neuropathy, and neurological impairments. 3
Occupational exposure to methanol through inhalation is rare but poses substantial health risks, particularly in industrial settings where ventilation and safety protocols may be insufficient. 4 In shrimp processing plants and similar workplaces, workers may encounter methanol or hydrocarbon vapors during routine operations, often without proper protective equipment. Exposures to methanol have been documented in several industries, such as those involving carburetor cleaners, industrial cleaning, and cosmetic products, highlighting the risks associated with inadequate regulation and oversight. 5 In addition, cases of large-scale methanol poisoning have been reported in countries such as Iran and Libya due to the use of contaminated industrial alcohol, emphasizing the critical need for preventive measures in underregulated work environments. 6 In the United States, methanol exposure incidents are frequently linked to products such as windshield washer fluids and carburetor cleaners, further underscoring its widespread industrial use and potential for harm in occupational settings. 7
Inhalational methanol poisoning presents unique challenges due to its nonspecific symptoms, which can include headache, chest tightness, shortness of breath, and dizziness. These early manifestations often overlap with other toxic exposures, complicating diagnosis and delaying timely intervention. Prolonged exposure increases the risk of severe respiratory complications, such as chemical pneumonitis, acute respiratory distress syndrome (ARDS), and airway injury. 8
The management of methanol poisoning typically involves supportive measures, including the correction of metabolic acidosis with bicarbonate and the administration of antidotes such as fomepizole or ethanol to inhibit further metabolism to toxic intermediates. In severe cases, hemodialysis is used to facilitate the clearance of methanol and formate. 9 For patients presenting with respiratory complications, additional interventions such as mechanical ventilation, corticosteroids, and antibiotics are frequently employed to address airway inflammation and secondary infections. 10
We present the case of an 18-year-old shrimp processing worker who developed acute respiratory failure following accidental inhalation of methanol vapors and achieved a successful recovery after treatment with therapeutic segmental pulmonary lavage (TSPL).
Case Presentation
An 18-year-old male presented to the emergency department following the accidental inhalation of a substance labeled as kerosene while working at a shrimp processing plant. The exposure occurred when the patient opened a bottle labeled as “kerosene,” commonly used for cleaning equipment in the facility. However, the bottle was confirmed to contain methanol, leading to the rapid release of toxic vapors in a poorly ventilated environment.
The patient exhibited signs of acute respiratory failure, including the use of accessory muscles, intercostal retractions, and generalized wheezing. Initial vital signs showed a respiratory rate of 44 breaths per minute, a heart rate of 151 beats per minute, and a peripheral oxygen saturation (SpO2) of 80%. Arterial blood gas analysis revealed metabolic acidosis (pH 7.26, HCO₃⁻ 16 mmol/L) with partial respiratory compensation (PaCO₂ 28 mmHg, PaO₂ 55 mmHg).
The patient reported additional symptoms of dizziness, chest tightness, and dyspnea immediately following the exposure. His clinical condition necessitated intubation and transfer to the intensive care unit (ICU). A chest radiograph revealed diffuse “cotton-like” infiltrates throughout the lung fields. In the ICU, the patient was placed on invasive mechanical ventilation in intermittent positive-pressure ventilation mode with AutoFlow (Dräger Evita 4; Drägerwerk AG & Co. KGaA, Lübeck, Germany). Sedation was maintained with propofol (1 mg/kg/h), and analgesia was achieved with fentanyl (0.5 mcg/kg/h). Vasopressor support was not required.
Initial laboratory results showed leukocytosis (18,500 cells/mm³) with neutrophilia (92%), an elevated C-reactive protein (CRP) level of 131 mg/L, thrombocytopenia (77 × 10⁹/L), and no significant liver function abnormalities. The patient was started on methylprednisolone, hydrocortisone, and triple antibiotic therapy (ceftriaxone, levofloxacin, and vancomycin).
On the second day, his leukocyte count decreased to 12.5 × 10⁹/L, with neutrophils at 62%, and platelets at 81.4 × 10⁹/L. Chest computed tomography (CT) revealed bilateral “cotton-like” opacities (Figure 1). Liver function tests remained normal. Viral serologies were negative, and methanol metabolites were detected in blood (55 mg/dL) and urine (95 mg/L; Table 1).
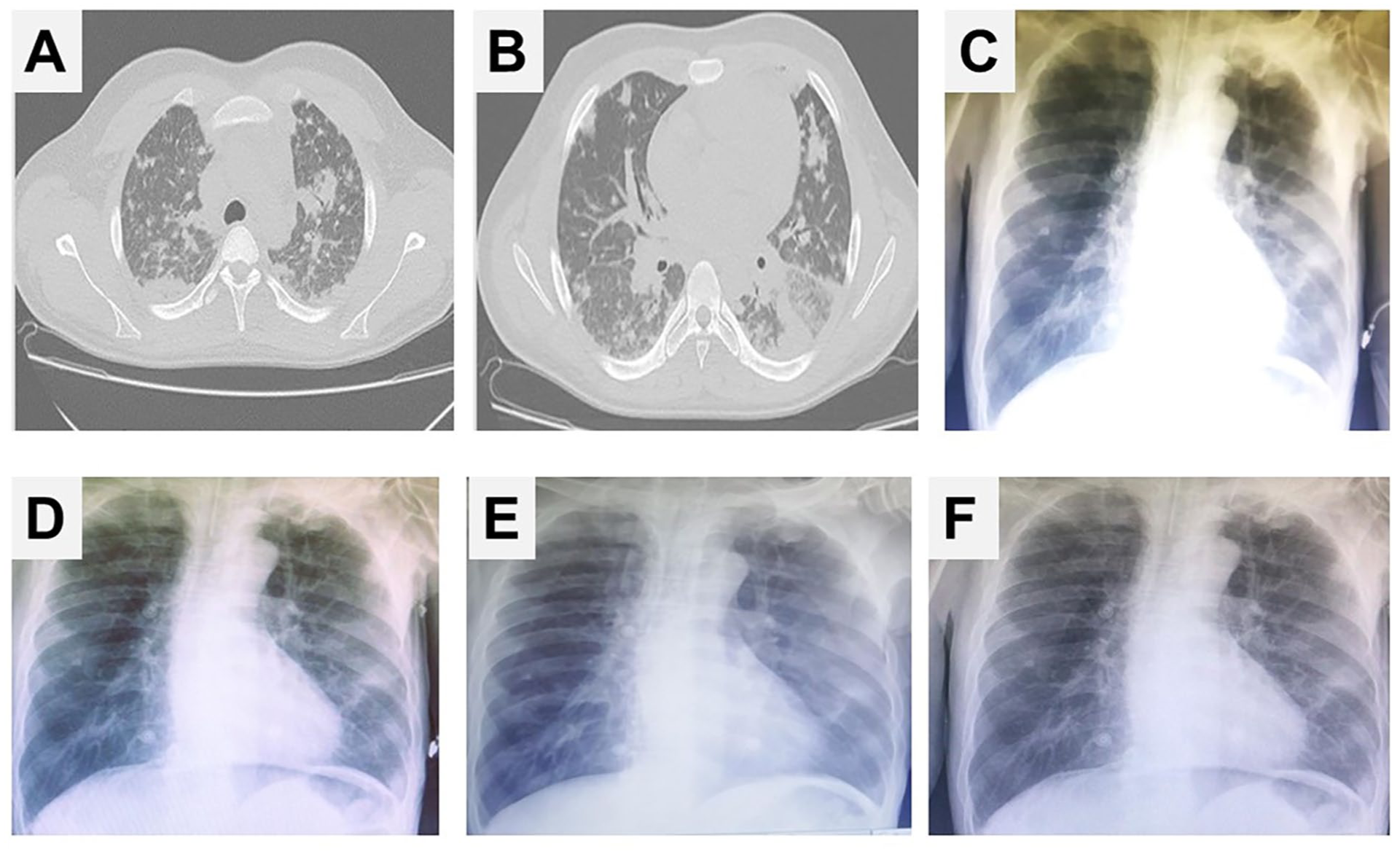
Radiological evolution of methanol-induced lung injury and response to TSPL. (A) and (B) Axial chest CT images obtained at admission, prior to TSPL, demonstrate bilateral ground-glass opacities and consolidations with a characteristic “cotton-wool” appearance, predominantly affecting the lower lobes. These findings are consistent with chemical pneumonitis secondary to methanol inhalation. (C) Chest radiograph taken at admission (pre-TSPL) reveals bilateral basal infiltrates with blurring of the diaphragmatic and cardiac borders. (D-F) Sequential chest radiographs obtained on Days 2, 3, and 4, respectively, show progressive radiographic improvement following TSPL, including partial resolution of opacities and improved lung aeration. These changes closely correlate with the patient’s rapid clinical recovery.
Chronological Summary of Clinical Parameters, Laboratory Findings, Imaging Results, and Therapeutic Interventions in a Patient With Methanol Inhalation-Induced Lung Injury Treated With TSPL.
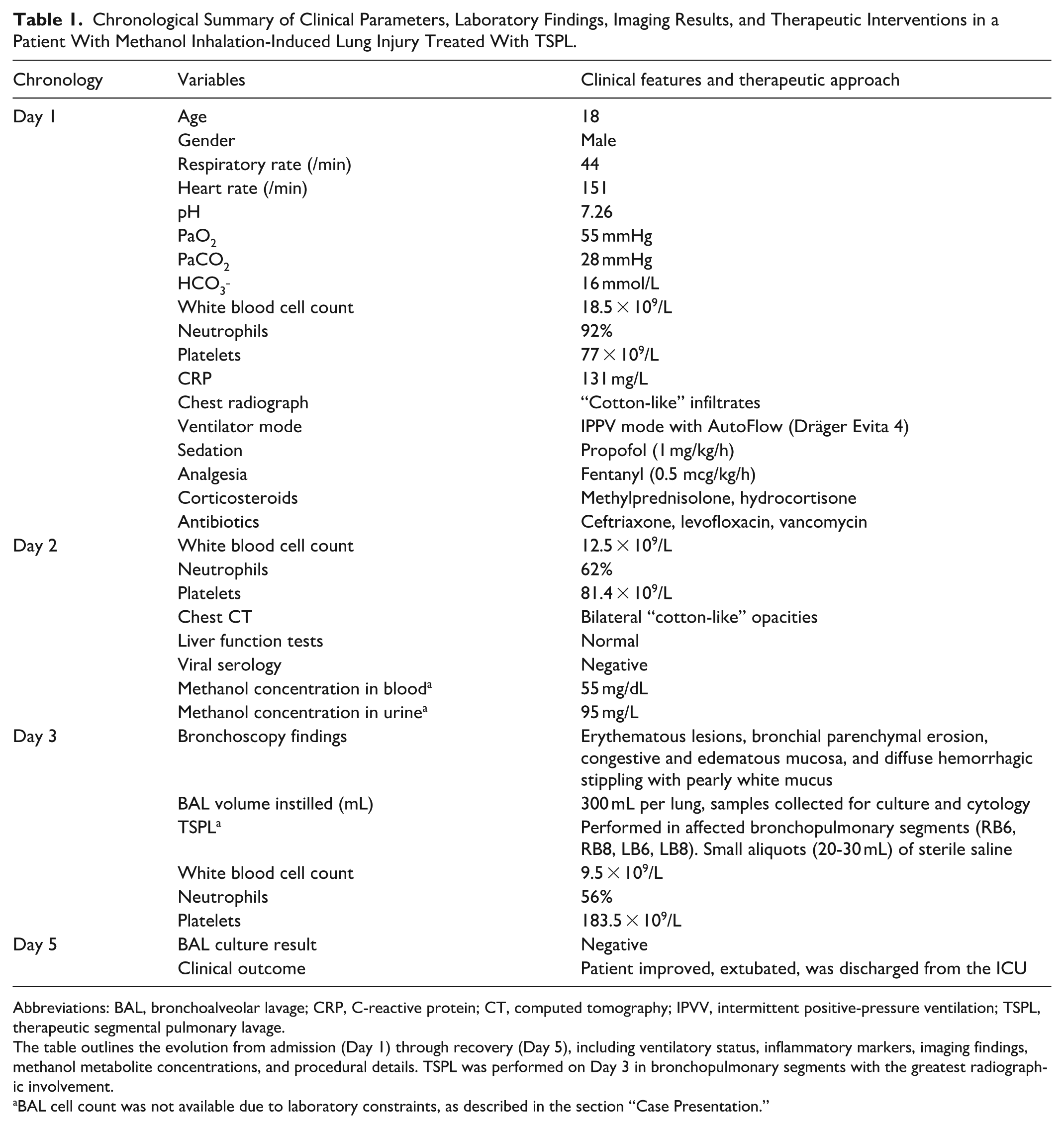
Abbreviations: BAL, bronchoalveolar lavage; CRP, C-reactive protein; CT, computed tomography; IPVV, intermittent positive-pressure ventilation; TSPL, therapeutic segmental pulmonary lavage.
The table outlines the evolution from admission (Day 1) through recovery (Day 5), including ventilatory status, inflammatory markers, imaging findings, methanol metabolite concentrations, and procedural details. TSPL was performed on Day 3 in bronchopulmonary segments with the greatest radiographic involvement.
BAL cell count was not available due to laboratory constraints, as described in the section “Case Presentation.”
Bronchoscopy was performed to evaluate the suspected respiratory complications, including the risk of chemical pneumonitis caused by methanol inhalation. Findings included erythematous lesions, bronchial parenchymal erosion, congestive and edematous mucosa, and diffuse hemorrhagic stippling with pearly white mucus (Figure 2). Bronchoalveolar lavage (BAL) was performed with 300 mL of saline per lung, and samples were collected for culture and cytology.

Bronchoscopic findings and TSPL. Bronchoscopic images show airway injury following methanol inhalation: (A, B) Erythematous and edematous bronchial mucosa with significant congestion, consistent with acute chemical irritation; (C, D) Diffuse hemorrhagic stippling with pearly white mucus, suggestive of focal bleeding, fibrin deposition, and early reparative changes. Given the severity of airway involvement, TSPL was performed with small aliquots (20-30 mL) of sterile saline instilled and aspirated in the right lower lobe segments (RB6: superior basal, RB8: anterior basal) and the left lower lobe segments (LB6: superior basal, LB8: anteromedial basal), facilitating clearance of inflammatory exudates and improving airway patency. TSPL, therapeutic segmental pulmonary lavage.
In addition to the standard BAL approach, TSPL was performed in the most affected bronchopulmonary segments. Based on the CT findings, which revealed extensive “cotton-like” infiltrates predominantly in the lower lobes, TSPL was focused on the right lower lobe segments (RB6: superior basal, and RB8: anterior basal) and the left lower lobe segments (LB6: superior basal, and LB8: anteromedial basa; Figure 2). Small aliquots (20-30 mL) of sterile saline were instilled into each of these segments and gently aspirated, achieving a retrieval rate of approximately 70% to 80% of the instilled volume. This technique aimed to remove the accumulated inflammatory exudates contributing to the patient’s respiratory compromise.
Following the lavage, the patient showed significant clinical improvement, enabling weaning from mechanical ventilation and extubation. Post-procedure laboratory findings revealed normalization of leukocyte counts (9.5 × 10⁹/L) with 56% neutrophils and improved platelet counts (183.5 × 10⁹/L). BAL cultures were negative. The patient was discharged from the ICU 48 hours after extubation.
Discussion
Methanol is widely used in industrial and household products, including cleaning agents, antifreeze, and solvents. While ingestion and dermal contact are the most common routes of poisoning, inhalational exposure remains exceptionally rare and presents unique diagnostic and therapeutic challenges. 1 These difficulties arise from the nonspecific nature of symptoms, which often leads to delayed diagnosis and management. The severity of methanol intoxication depends on the route, duration, and concentration of exposure. Ingestion typically leads to rapid systemic absorption, causing severe metabolic acidosis, optic neuropathy, and central nervous system depression. By contrast, inhalation exposure has a more insidious onset, often delaying medical intervention. Prolonged exposure can exacerbate complications such as lipoid pneumonitis, alveolar damage, increased transpulmonary pressure, and ARDS. 11 These complications highlight the importance of early clinical suspicion and prompt intervention in cases of inhalation toxicity.
In this case, the patient developed severe respiratory dysfunction following methanol vapor inhalation, necessitating mechanical ventilation and advanced diagnostic procedures. While standard management of methanol poisoning includes supportive care, correction of metabolic acidosis, and administration of fomepizole or ethanol to inhibit methanol metabolism, the presence of respiratory complications required additional therapeutic measures. Corticosteroids and antibiotics were used to manage airway inflammation and prevent secondary infections, but bronchoscopy with BAL proved pivotal to the patient’s recovery.
A notable aspect of this case was the implementation of TSPL. While BAL is primarily employed for diagnostic purposes in pulmonary pathology, TSPL extends beyond sample collection by targeting specific bronchopulmonary segments affected by toxic injury. By instilling small aliquots of saline into the most severely involved lung segments, followed by controlled aspiration, TSPL may facilitate clearance of inflammatory debris and toxic residues, improving gas exchange and ventilation-perfusion balance. In this patient, incorporating TSPL as an adjunct to BAL likely enhanced exudate removal in the most affected bronchopulmonary segments, leading to accelerated clinical recovery.
Although spontaneous improvement following inhalational methanol exposure is possible, the marked and rapid improvement in oxygenation and radiologic findings observed immediately after TSPL—despite persistent hypoxemia under standard care—strongly supports a therapeutic effect of the lavage. This intervention appears to have contributed decisively to the resolution of pulmonary infiltrates and the patient’s timely extubation. Given the timing and magnitude of the recovery, we argue that TSPL played a critical role beyond supportive management alone.
The potential of segmental lavage techniques has been demonstrated in other pulmonary conditions, such as pulmonary alveolar proteinosis (PAP). 12 In cases of autoimmune PAP presenting with severe respiratory failure, segmental lung lavage under general anesthesia has been shown to significantly improve respiratory function and radiographic findings, even in non-lavaged lung areas. 13 Similarly, BAL with segmental targeting has been successfully utilized in PAP patients with profound hypoxemia, resulting in long-term remission and prevention of recurrence. 14 Furthermore, a report on post-COVID-19 PAP demonstrated that TSPL improved severe hypoxia and bilateral infiltrates after diagnostic BAL confirmed the presence of proteinaceous material in the alveoli.
In previous literature, BAL has been described in cases of iatrogenic methanol exposure, where a methanol-based cell preservation solution (Cytolyt) was inadvertently administered instead of saline. 15
The distinction between therapeutic benefit attributable to TSPL and spontaneous recovery is substantiated by convergent evidence from multiple sources in the literature. Cases of chemical pneumonitis have demonstrated dramatic clinical improvements following BAL, with documented reports of “dramatic improvements after BAL in patients with hydrocarbon pneumonitis.” 1 Similarly, in pesticide-induced chemical pneumonitis, therapeutic BAL has facilitated “rapid patient recovery with a favorable outcome,” indicating that active intervention positively modifies the natural disease trajectory. 16
Systematic evidence from exogenous lipoid pneumonia, a condition clinically analogous to our presentation, demonstrates that 96.7% of patients treated with therapeutic lung lavage experience clinical improvement, in contrast to limited spontaneous resolution observed in untreated cases. 17 The underlying pathophysiological mechanism supports this therapeutic attribution, as segmental lavage provides direct physical removal of accumulated toxic material, inflammatory mediators, and cellular debris from alveolar compartments, thereby interrupting the cycle of perpetual inflammatory damage characteristic of chemical pneumonitis. 18
The temporal pattern of improvement observed in our patient, specifically the rapid radiological and clinical resolution within 24 to 48 hours following TSPL, markedly exceeds the spontaneous recovery patterns typically reported in severe chemical pneumonitis, which generally requires weeks for resolution in cases achieving recovery without specific therapeutic intervention.19,20
Conclusion
This case highlights the rare but severe pulmonary toxicity that may result from occupational methanol vapor inhalation. In addition to standard supportive measures, the use of TSPL may represent a valuable adjunctive intervention in cases of localized airway injury and severe chemical pneumonitis. The patient’s rapid clinical and radiologic improvement following TSPL supports its potential therapeutic benefit in selected cases of toxic inhalant exposure. Further research is warranted to define its role and safety profile in similar contexts.
Footnotes
Acknowledgements
None.
ORCID iDs
Ethical Considerations
Ethical approval to report this case was obtained from Comité de Ética en Investigación en Seres Humanos del Hospital General de Babahoyo (Approval number: IESS-HG-BA-DTMC-2019-1231/CÓDIGO 004).
Consent to Participate
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.