
Abstract
Sarcoidosis is a systemic disease where extrapulmonary presentation of the disease often goes unrecognized as it overlaps with many disease manifestations. End-stage renal disease (ESRD) can be complicated by hypercalcemia and encephalopathy, both potential signs of sarcoidosis. These numerous extrapulmonary presentations may delay timely diagnosis and treatment. In this case report, a 53-year-old male with ESRD was admitted following an unresponsive episode during routine hemodialysis, later found to have sarcoidosis. Initial presentation notable for hypothermia, tachycardia, leukocytosis, and metabolic derangements. Bronchoalveolar lavage cultures subsequently grew methicillin-sensitive staphylococcus aureus, successfully treated with cefazolin. However, the patient remained encephalopathic and hypercalcemic. Further workup showed nonparathyroid hormone-mediated hypercalcemia with a normal 25-OH vitamin D and elevated 1,25-OH vitamin D, concerning for sarcoidosis, malignancy, or tuberculosis. Additional computed tomography imaging and endobronchial ultrasound-guided biopsy illustrated enlarged lymph nodes with splenomegaly and nonnecrotizing granulomas, respectively, confirming the diagnosis of sarcoidosis. He was started on methylprednisolone, pantoprazole, and trimethoprim/sulfamethoxazole for pneumocystis jirovecii pneumonia prophylaxis; serum calcium levels started to drop, and his mentation improved. While his encephalopathy was initially presumed secondary to his ESRD and infection, further workup revealed sarcoidosis. Untreated sarcoidosis has significant health complications including lung fibrosis, pulmonary hypertension, heart arrhythmias, and neurological deficits. This case highlights the importance of maintaining a broad differential in the setting of critically ill patients as clinical presentations can be multifactorial. Furthermore, patients with a complex medical history such as ESRD on hemodialysis can make concluding sarcoidosis as a diagnosis more difficult.
Introduction
Sarcoidosis is a complex autoimmune multisystem disease characterized by the formation of nonnecrotizing granulomas in various organs, often leading to masked symptoms that delays timely diagnosis and treatment.1,2 While sarcoidosis is more common in women aged 30 to 50 of African and Scandinavian descent, it can affect people of all ethnic backgrounds and all ages.1-3 Over 90% of sarcoidosis cases present with intrathoracic involvement seen with symmetrical bilateral hilar adenopathy and interstitial infiltrates4,5; however, extrapulmonary manifestations should not be overlooked. The skin, eyes, liver, spleen, heart, lymph nodes, central nervous system, kidneys, salivary glands, and musculoskeletal system are potential sites of primary sarcoidosis presentation.1,6 Specifically, renal involvement can rarely present as isolated hypercalcemia.
In patients with end-stage renal disease (ESRD) on long-term hemodialysis, chronic hypocalcemia can occur leading to a secondary hyperparathyroidism with elevated parathyroid hormone (PTH). This, often in the setting of calcium-based binders, can be further complicated and lead to autonomous PTH secretion or tertiary hyperparathyroidism, causing hypercalcemia. 7 Metabolic changes due to chronic kidney disease including hypercalcemia and uremia can lead to neurological changes and encephalopathy.8,9 The retention of uremic solutes secondary to poor kidney function leads to electrolyte and hormonal imbalances causing uremic encephalopathy 8 ; hypercalcemia can be a catalyst for neurotoxic cascades causing neuropsychiatric dysfunction.10,11 In patients with ESRD, sarcoidosis is an often missed diagnosis as hypercalcemia workup may not be thoroughly completed. 12 Encephalopathy further complicates this picture as sarcoidosis can affect the nervous system but is also seen as a complication of ESRD. 13
Sarcoidosis may be present in concurrence with other disease processes; however, with its numerous systemic presentations, it is difficult to identify the root cause of symptoms, delaying, or misdiagnosing the etiology. There is no standardized criteria for diagnosis aside from 3 broad parameters: the clinical or radiological presentation, nonnecrotizing granulomas on tissue biopsies, and the exclusion of alternative diagnoses. 14 This case highlights a complex presentation of a 53-year-old male with ESRD who presented following an unresponsive episode during routine hemodialysis, later found to have hypercalcemia secondary to sarcoidosis.
Case Report
A 53-year-old male with past medical history of hypertension, diabetes mellitus II, schizophrenia, and ESRD on hemodialysis presented to the emergency department via emergency medical services after becoming unresponsive after 1 hour of routine hemodialysis treatment. Initial electrocardiogram (ECG) during dialysis treatment was reported to be concerning for ST elevation myocardial infarction; he received nitroglycerin in route with no improvement. On initial physical exam, he had forced neck rotation to the left, slow rhythmic contractions of right upper extremity, and gaze deviation to the left with occasional slow vertical nystagmus, initially concerning for seizure. Vital signs were notable for hypothermia at 34.5 °C, hypotensive at 97/73 mmHg, tachycardia to the 107 beats/minute, and an oxygen saturation of 100%. Initial labs showed leukocytosis of 18.4 thous/mm3, hyponatremia of 135 mEq/L, hypokalemia of 3.0 mEq/L, hypercalcemia of 11.6 mg/dL after correcting for albumin, hyperphosphatemia of 11.2 mg/dL, and lactic acidosis of 2.4 mmol/L. Repeat ECG showed sinus tachycardia with no evidence of ST elevation or depression. Chest X-ray showed bilateral airspace opacities concerning for fluid overload and pulmonary edema. He received intravenous (IV) midazolam and naloxone with resolution of physical exam findings except for left gaze deviation. Code stroke was activated; however computed tomography (CT) of the head without contrast showed no acute intracranial process. He was subsequently intubated due to inability to protect airway; blood cultures were obtained followed by empiric antibiotics initiation; and mean arterial pressure was maintained above 65 with norepinephrine due to continued hypotensive state. He was admitted to the medical intensive care unit for management of airway protection and shock.
Inpatient workup included electroencephalogram showing diffuse encephalopathy, no seizures, or epileptic activity, echocardiography showing reduced left ventricular ejection fraction of 40% to 45%, and magnetic resonance imaging of the brain showing acute right greater than left bifrontal punctate infarctions without hemorrhage. Blood cultures subsequently came back negative, and empiric antibiotics were discontinued; however, bronchoalveolar lavage grew methicillin-sensitive staphylococcus aureus for which he completed a 7-day course of cefazolin. He continued to receive his routine hemodialysis during his inpatient stay.
Despite his antibiotic treatment and routine hemodialysis, he remained hypercalcemic and encephalopathic. Laboratory workup showed the hypercalcemia of 12.3 mg/dL was non PTH-mediated (PTH of 15.5 pg/mL), with normal 25-OH vitamin D of 27.7 ng/mL and elevated 1,25-OH vitamin D >200 pg/mL, concerning for possible sarcoidosis, malignancy, or tuberculosis. CT chest showed enlarged mediastinal and hilar lymph nodes concerning for lymphoproliferative process (Figure 1). CT abdomen/pelvis showed abdominal lymphadenopathy with borderline splenomegaly and nonobstructing left renal stones, also suggesting a lymphoproliferative process (Figure 2). QuantiFERON tuberculosis screening came back negative; angiotensin-converting enzyme (ACE) elevated at 201 U/L with a normal reference range of 16 to 85 U/L. Serum protein electrophoresis showed polyclonal hypergammaglobulinemia in the setting of hypoalbuminemia, consistent with chronic inflammation. Endobronchial ultrasound-guided biopsy revealed nonnecrotizing granulomas. Subsequent rheumatological and infectious workup including human immunodeficiency virus, antinuclear antibody, anti-double stranded DNA, anti-smith, anti-Sjogren syndrome type A/type B, anti-ribonucleoprotein (RNP), anti-topoisomerase 1, anti-centromere, and anti-U1 RNP were all negative. Given negative infectious and overlapping disease processes workup, he was diagnosed with sarcoidosis and started on methylprednisolone, pantoprazole, and trimethoprim/sulfamethoxazole for pneumocystis jirovecii pneumonia prophylaxis. His serum calcium levels started to drop after starting the glucocorticoid and mentation improved.
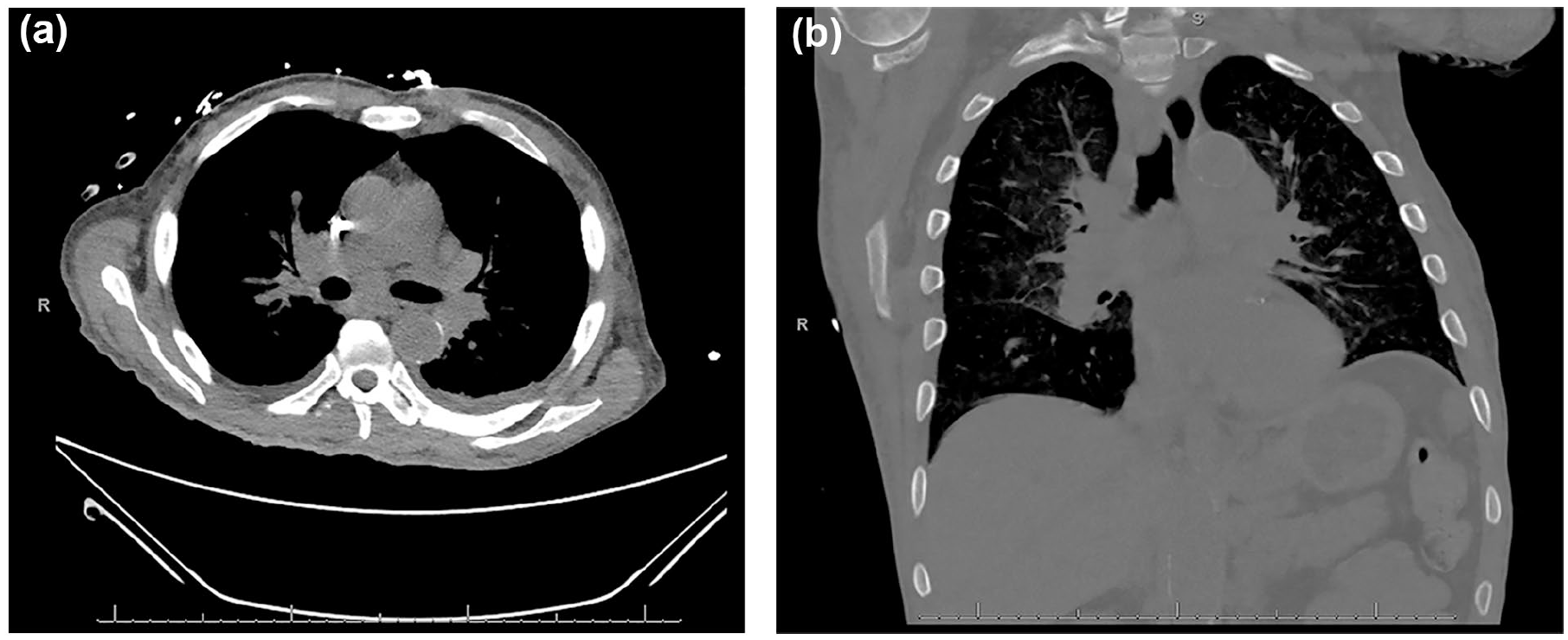
CT chest showed enlarged mediastinal and hilar lymph nodes concerning for lymphoproliferative process, both in axial (a) and coronal (b) slices. CT, computed tomography.
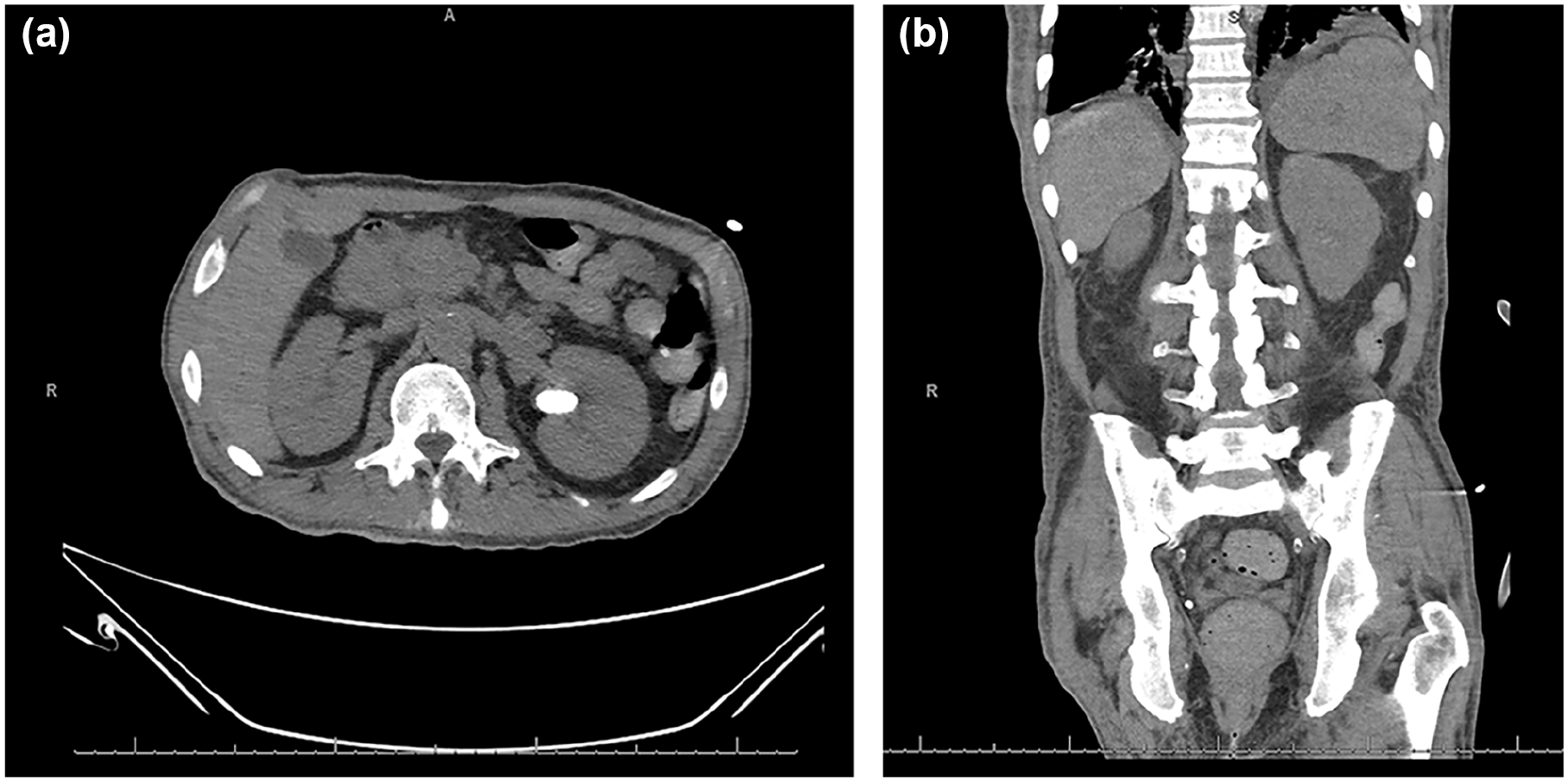
CT abdomen/pelvis showed abdominal lymphadenopathy, most notably in the upper abdomen and retroperitoneum in axial (a) and borderline splenomegaly in coronal (b). CT, computed tomography.
Discussion
Sarcoidosis often presents with nonspecific symptoms that widely overlaps with many other conditions. Our patient had bilateral mediastinal/hilar lymphadenopathy, nonthoracic lymphadenopathy, hypercalcemia with normal PTH, increased 1,25-OH vitamin D, and normal 25-OH vitamin D, elevated ACE levels, splenomegaly, and nonnecrotizing granulomas on biopsy, all suggestive of sarcoidosis diagnosis. Sarcoidosis is known as “the great mimicker” as it often imitates other conditions, including infections, neuropsychiatric symptoms, and hypercalcemia, all symptoms that our patient had initially obscuring our focus to a concurrent or underlying diagnosis of sarcoidosis. 15 Sarcoidosis requires timely diagnosis to prevent significant complications, such as lung fibrosis, pulmonary hypertension, heart arrhythmias, and neurological deficits, including seizures and encephalopathy. 16
Renal sarcoidosis is a rare form of sarcoidosis presenting with granulomatous inflammation of the renal parenchyma, known as granulomatous interstitial nephritis, and hypercalcemia-related disorders.17,18 Elevated 1,25-OH vitamin D is the main cause of hypercalcemia in sarcoidosis as it is overproduced by the activated lymphocytes and macrophages in the nonnecrotizing granulomas.19,20 This results in downregulation of PTH as seen in our patient with elevated calcium but normal PTH. The hypercalcemia and likely subsequent hypercalciuria can be treated medically with prednisone, 15 to 25 mg/day, which reduces the overproduction of 1,25-OH vitamin D, decreasing overall calcium levels. 19 Hypercalcemia can also lead to neuropsychiatric symptoms, another symptom of our patient.9,11
Neurological sarcoidosis has been reported in only 5% to 10% of all patients with sarcoidosis with clinical manifestations including meningitis, cranial neuropathy, myelopathy, sellar disease, parenchymal disease, and encephalopathy.21,22 Encephalopathy often presents with nonspecific white matter lesions that may be small and focal or larger and diffuse.13,21 Our patient was discovered to have encephalopathy as well; however, it is unknown whether his chronic kidney disease secondary to his hypertension and diabetes mellitus II, sarcoidosis, or both were contributing to this manifestation. Immunosuppression is vital in the treatment of neurosarcoidosis to minimize neurologic injury. IV methylprednisolone is initially recommended for severely affected patients which can then be transitioned to oral prednisone with follow-up monitoring, 21 the treatment regimen our patient received.
Renal and neurological sarcoidosis can present with hypercalcemia-related disorders. While disordered of calcium metabolism can be appreciated in patients with known kidney disease; it is possible there is an underdiagnosis of sarcoidosis in patients with ESRD due to the overlapping symptomatology. We initially presumed the encephalopathy, and hypercalcemia was secondary to his ESRD diagnosis’; however, this case emphasizes the importance of maintaining a broad differential in the setting of critically ill patients, especially in patients with ESRD as clinical presentations can be multifactorial.
Footnotes
Acknowledgements
We would like to express our gratitude to the patient for granting us permission to share his case, which contributed to the learning experience of this report.
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent for Publication
Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Prior Presentation of Abstract Statement
Not previously presented.