
Abstract
Xanthogranulomatous pyelonephritis (XGP) is a rare, severe form of chronic kidney infection that mimics renal malignancies, often leading to diagnostic challenges. We present the case of a 36-year-old woman with a 2-month history of progressive lower back pain, fever, and weight loss. Imaging revealed left renal enlargement with multiple low-attenuation areas and large staghorn calculi, suggestive of XGP. Middle-aged women are primarily affected by recurrent urinary tract infections and renal calculi, leading to extensive renal destruction. Characteristic “bear paw” sign on computed tomography suggests XGP; however, histopathological confirmation is required. Early recognition and intervention are essential to prevent irreversible renal damage. Our case highlights the need for clinical awareness and prompt evaluation to minimize disease burden and improve patient outcomes.
Introduction
Xanthogranulomatous pyelonephritis (XGP) is a rare, severe type of chronic kidney infection that often mimics renal malignancies, leading to challenges in early diagnosis and treatment. 1 First described by Schlagenhaufer in 1916, it accounts for 0.6% to 1% of pyelonephritis cases globally. 2 It primarily affects middle-aged and older women, commonly associated with chronic urinary tract infections (UTIs), renal calculi, and urinary obstruction. 2 The pathophysiology involves a prolonged inflammatory response leading to granulomatous infiltration, renal parenchymal destruction, and, in advanced cases, perinephric abscess formation or fistula development. 3
Clinically, XGP can resemble renal tumors, presenting nonspecific symptoms like flank pain, fever, anemia, a palpable flank mass, and recurrent urosepsis.4,5 Imaging modalities, particularly contrast-enhanced computed tomography (CT), play a crucial role in diagnosis by showing characteristic “bear paw” sign, caused by hypoattenuating areas of renal destruction, and help differentiating from renal malignancies. However, definitive diagnosis requires histopathological confirmation. 6
Treatment usually involves nephrectomy for advanced cases, with segmental excision for localized disease. Recurrence is rare, though postoperative complications like bacteriuria or hypertension may occur. 7 Early intervention is critical in preventing irreversible renal damage, making prompt diagnosis and management essential.
Case Presentation
A 36-year-old woman presented to the emergency department with a 2-month history of persistent, dull, and aching lower back pain, which had progressively worsened over the past week and radiated to the left groin. Associated with intermittent fevers with chills over the past month and she also reported an unintentional weight loss of approximately 4.5 kg over the last 4 months. She denied any alcohol or tobacco use. No history of difficult delivery or pregnancy complications was present. However, as the patient is an immigrant from the Caribbean area, no official documentation is available to verify her obstetric history.
The patient’s vital signs were as follows: temperature of 38.3°C, heart rate of 110 beats per minute, blood pressure of 130/85 mmHg, respiratory rate of 21 breaths per minute, and oxygen saturation of 98% on room air. On examination, she appeared uncomfortable, with pallor. Mild tenderness was noted in the left lower quadrant and over the left costovertebral angle, with no rebound tenderness or guarding. Other system examinations, including cardiovascular, respiratory, and neurological, were unremarkable. Initial lab tests showed notable abnormalities, including a white blood cell count of 9.7 × 109/L (normal: 4.0-11.0 × 109/L), hemoglobin of 5.4 g/dL (normal: 12.0-16.0 g/dL), hematocrit of 21.2% (normal: 36.0%-46.0%), and platelets at 422 × 109/L (normal: 150-400 × 109/L). The C-reactive protein was elevated at 67.4 mg/L (normal: <3.0 mg/L). Serum creatinine was 1.31 mg/dL (normal: 0.6-1.2 mg/dL) with a decreased estimated glomerular filtration rate of 54 mL/min/1.73m² (normal: >90 mL/min/1.73m²). In addition, urine protein was elevated at 295 mg/dL (normal: <150 mg/dL), and the prothrombin time was prolonged at 15.4 seconds (normal: 11.0-13.5 seconds). The chest X-ray was within normal limits. A retroperitoneal ultrasound revealed that the left kidney contained multiple echogenic foci compatible with renal calculi, the largest of which was located in the left mid-pole. In addition, fullness of the left renal pelvis was noted.
A CT scan of the abdomen and pelvis with contrast revealed mild enlargement of the left kidney compared to the right, with multiple large areas of low attenuation centrally within the parenchyma, the presence of large staghorn calculi (blue arrow), and a characteristic “bear paw” sign (red arrow; Figure 1). One of the calculi was located in the lower pole calyces and extended into the renal pelvis. Another large calculus was identified within the mid and upper pole calyces. These findings were suggestive of XGP. The primary cause of XGP in this patient is a staghorn calculus. The patient reported previous episodes of dysuria but did not seek medical attention due to a lack of insurance. In addition, ill-defined, loculated, rim-enhancing collections and soft tissue density adjacent to the left kidney were seen, contacting the spleen, raising concerns for potential phlegmon or early abscess formation. The patient was initiated on intravenous ceftriaxone. Urine cultures grew Staphylococcus agalactiae, which was pan-sensitive to antibiotics. Urine cytology was not performed, and therefore, xanthoma cells were not observed. A urology consultation was obtained, and interventional radiology was recommended for the insertion of a nephrostomy tube. Subsequently, a nuclear medicine (NM) kidney function test was performed, which revealed markedly diminished renal function in the left kidney, contributing approximately 2% to the total renal function, with the right kidney supplying the remaining 98% (Figure 2). The patient underwent diagnostic ureteroscopy, retrograde pyelogram, and antegrade pyelogram as part of the evaluation.

Axial contrast-enhanced computed tomography scan of the abdomen showing the characteristic “bear paw” sign (red arrows) and a staghorn calculus (blue arrow) in the left kidney, indicative of xanthogranulomatous pyelonephritis.
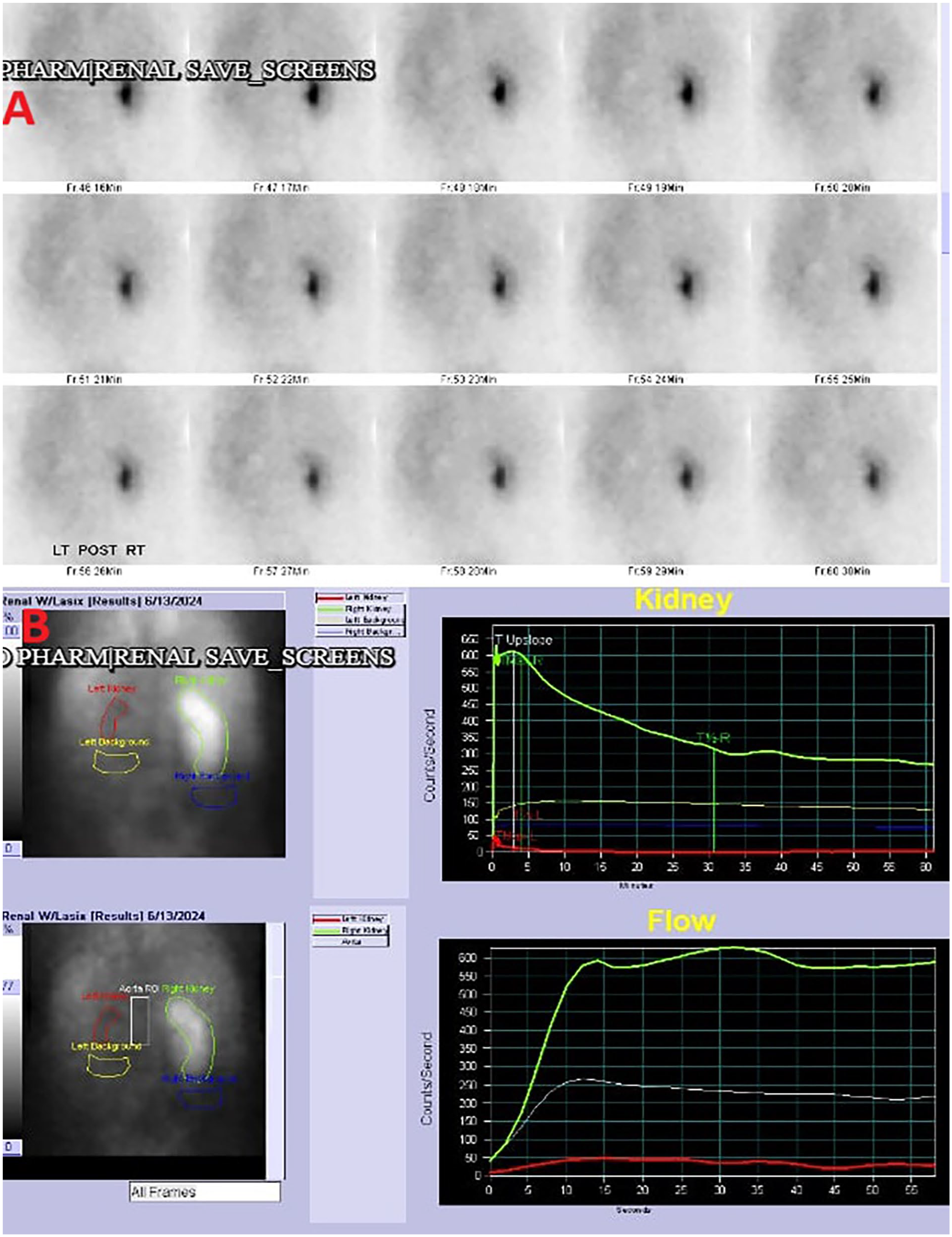
Nuclear medicine renal scan (A) demonstrating severely diminished function of the left kidney (2%; B), with compensatory hyperfunction of the right kidney (98%; B).
The patient underwent CT-guided drainage of the left perinephric collection, during which an 8 French pigtail drainage catheter was inserted into the mid-to-upper pole collecting system of the left kidney. Approximately 55 cc of purulent fluid was aspirated during the procedure.
The gold standard treatment of nephrectomy was discussed with the patient, but she initially declined and requested to continue with medical management. The diagnosis of XGP does not require a kidney biopsy, as it is typically confirmed through histopathological examination following nephrectomy. The patient was scheduled for nephrectomy; however, due to severe inflammation and adhesion to adjacent organs, nephrectomy was not feasible without en bloc resection. The urologist opted for left percutaneous nephrolithotomy and initiated antibiotic therapy to control the infection. A repeat nephrectomy will be attempted once the infection is cleared. She was discharged on a 2-week course of antibiotics. However, the patient was readmitted 1 week later with complaints of referred left shoulder pain and recurrent UTI. A repeat CT scan of the abdomen and pelvis showed an interval decrease in the size of the left perinephric abscess. Given the persistence of her symptoms, the patient agreed to undergo a left nephrectomy, which was performed without complications. Postoperatively, she has been doing well, with follow-up showing no complications.
Discussion
XGP accounts for less than 1% of chronic pyelonephritis cases, leading to significant destruction and morbidity. 8 Our case is unique in that it involves a young, otherwise healthy female with an advanced stage of XGP requiring nephrectomy. Most reported cases occur in older adults with predisposing risk factors. 2 Etiology primarily involves recurrent UTIs or renal obstruction, leading to granulomatous inflammatory infiltrate destroying the renal parenchyma and abscess or fistula formation.4,8 Our patient had multiple risk factors for XGP, including recurrent UTIs, obstructive uropathy due to staghorn calculi, mixed hyperlipidemia, and female gender. XGP progression is categorized based on the extent of renal and extrarenal involvement. 1 XGP may be focal and only localized to the cortex, segmentally involving only a region of the kidney, or the most common from diffuse widespread involvement. 9 This widespread involvement carries a significant health burden. Initially, the XGP is stage 1, involving only the kidney, followed by stage 2, including the renal pelvis or the perinephric fat, and finally, stage 3 is perinephric, involving adjacent organs or the retroperitoneum. 1 As the disease advances to more severe stages, involving retroperitoneum, psoas abscess formation, or fistula development, the risk of complications rises significantly, leading to increased morbidity and a higher likelihood of septicemia. 10
Most patients present with nonspecific symptoms similar to pyelonephritis, including flank pain, fever, gross hematuria, and recurrent UTIs. 9 However, they can also develop other symptoms, such as shoulder pain from abscess formation near the diaphragm, found in some patients with diffuse stage 3 XGP, such as in our case.1,8 The lack of symptoms specific to XGP makes it difficult to differentiate from other infective processes. Fever has been documented in some literature to only be present in about half of patients, but flank pain was present in nearly 90% of patients. 11 Other findings reported in the literature, such as weight loss, anemia, and ischemic colitis, but again are all atypical presentations. 1
Diagnosing XGP can be difficult, as the only definitive way is by biopsy.8,9 Definitive confirmation relies on histopathological findings. CT imaging can capture the inflammatory destruction by noting a radiological sign called “bear paw” secondary to hypoenhancement of the renal parenchyma with other multiple enhancing rings. 12 The presence of foam cells helps distinguish renal XGP from tuberculosis or tumors, eliminating diagnostic uncertainty. 13 Due to the chronic inflammatory response, renal function can become compromised, and patients later lose renal function. 9
Initial management often involves antibiotic therapy and percutaneous drainage of the renal pelvis to control infection. 1 Definitive treatment typically requires total or partial nephrectomy, as was done in our case, and it generally yields favorable outcomes. 1 Since preoperative diagnosis can be challenging—especially in the absence of xanthoma cells in urine—broad-spectrum antibiotic therapy and symptomatic treatment play a crucial role before surgery. 14 Early nephrectomy is often necessary for definitive treatment, while postoperative care should focus on maintaining fluid and electrolyte balance and preventing infections through continued broad-spectrum antibiotic coverage. 14 These steps are essential for ensuring successful patient outcomes. The diffuse form of XGP does lead to severe chronic inflammation and irreversible changes, unfortunately leaving nephrectomy as the only definitive form of treatment, again emphasizing the burden of the disease. 15 Nephrectomy, however, can lead to various complications, but our patient reported no complications thereafter. 16
In our case noted above, the young 36-year-old female initially presented complaining of lower back pain that radiated to the groin. In the subsequent presentation, she developed shoulder pain as the perinephric abscess appeared to be caused by diaphragmatic irritation. It was not until the patient agreed to have a nephrectomy that the diagnosis of XGP was confirmed. In fact, XGP is rarely seen in younger healthy patients, which made this diagnosis even more surprising. 8 Cultures grew S. agalactiae, however, the most commonly reported organisms are Escherichia coli, Proteus mirabilis, Pseudomonas, Enterococcus faecalis, and Klebsiella. 17 The patient did not present for any evaluation until her symptoms progressed for 2 months. As noted in our case, NM imaging revealed that the affected kidney only contributed 2% of the total renal function. It can be theorized that if she had presented earlier and the staghorn calculi were diagnosed, XGP would not have developed, and she would have maintained her renal function and preserved her kidneys.
Conclusion
Our case highlights the importance of timely evaluation and intervention, as earlier detection of staghorn calculi might have prevented progression to XGP. The unfortunate burden XGP placed on our patients emphasizes the importance of prompt evaluation and clinician insight into the possible outcomes if not treated earlier. Increased clinical awareness is crucial to avoid delays in diagnosis and to minimize disease burden.
Footnotes
Acknowledgements
None.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.