
Abstract
A thyroid storm is a medical emergency that requires high clinical suspicion and emergency treatment. We report an unusual case of thyroid storm and agranulocytosis managed with lithium therapy. The patient is a 32-year-old woman with a history of Graves’ disease on methimazole therapy who presented to the emergency department with fever and palpitations. She was diagnosed with COVID-19 infection a week ago. She was febrile and tachycardic with fine tremors on examination. Routine laboratory workup showed agranulocytosis. Serum thyroid-stimulating hormone levels are <0.01 µIU/ml (normal range is 0.45-5.33) with elevated T4 and T3 (10.4 pcg/ml [2.1-4.1 pcg/ml], 4.34 ng/dl [0.61-1.24 ng/dl]). Burch-Wartofsky Point Scale score was 60 points, highly suggestive of thyroid storm. A clinical diagnosis of thyroid storm was made. The precipitating factor in this case was identified as the recent COVID-19 infection. Adding to the conundrum is the co-existent agranulocytosis, precluding the usage of antithyroid medications. She was treated with beta-blockers, intravenous fluids, and steroid therapy to suppress T4 to T3 conversion. Lithium was started, given her neutropenia and thyroid storm. She responded to oral lithium therapy and was discharged. During follow-up, her symptoms were controlled and leucopenia resolved. In conclusion, COVID-19 is a recognized precipitating factor for thyroid storms. It is very rare to see co-existent thyroid storm and agranulocytosis, and lithium can be a useful option in such cases. This case report adds to the minimal literature existing on lithium use in patients with thyroid storm.
Introduction
A thyroid storm is a medical emergency that should be suspected and treated immediately. Several precipitating factors have been identified, including surgery, sepsis, and stress. 1 Recently, there has been increasing evidence of thyroid storm in the setting of COVID-19 illness. However, the literature is still limited to a few case reports. It is also not very rare to see patients with thyroid storms already on methimazole. Co-existent severe agranulocytosis and thyroid storm may be extremely rare but presents a therapeutic conundrum. We present a case of concomitant thyroid storm and severe agranulocytosis precipitated by methimazole therapy and COVID-19 infection managed with lithium therapy.
Case Presentation
Background History (September 2023)
The patient is a 32-year-old morbidly obese (body mass index: 42.25 kg/m2) woman with a prior diagnosis of Graves’ disease diagnosed in September 2023, when she presented with catabolic symptoms in the form of significant unintentional weight loss of 45 pounds in 3 weeks and other symptoms like heat intolerance, palpitations, and anxiety. Of note, the patient is a lactating mother and is 3 months into the postpartum state at the time of diagnosis of Graves’ disease. Before that presentation in September, she denied any history of goiter, thyroid disease, or any other autoimmune disease. She is a lifetime non-smoker. When she presented to the emergency department (ED) with the above symptoms, she was found to have a fever (101°F), a heart rate of 143/min, and tachypnea, and was evaluated for various causes like Sepsis, and Endocrine disorders, including thyroid pathologies. Burch-Wartofsky Point Scale (BWPS) score was 65 points, highly suggestive of thyroid storm (Table 1). 2 Serum thyroid-stimulating hormone (TSH) was <0.01 (Reference range: 0.45-5.33 µIU/ml), free T3 levels were 14.9 (Reference range: 2.1-4.1 pcg/ml), and free T4 level was 5.21 (0.61-1.24 ng/ml). Serum TSH receptor-binding antibodies (TRAb) were elevated, 17.36 IU/l (Reference range is <2 IU/l). Serum thyroid peroxidase antibodies (TPO) were also borderline elevated to 12 IU/ml (Reference range is <9 IU/ml). Given her symptoms of hyperthyroidism with consistent lab parameters and elevated TRAb levels, Graves’ disease was diagnosed. An ultrasound neck was done, pending lab results to establish an early diagnosis, which showed a diffusely heterogeneous and hypervascular thyroid, without discrete nodules. A clinical diagnosis of thyroid storm was made, and she started treatment. She was admitted to the intensive care unit (ICU) and started on an intravenous (IV) beta-blocker (Esmolol) later transitioned to oral metoprolol, IV fluids, and IV hydrocortisone (100 mg, 3 times daily), oral methimazole (20 mg, 3 times daily later transitioned to 30 mg once daily), Lugol’s iodine 5%, 0.4 ml every 8 hourly 1 hour after methimazole therapy. She improved significantly with the above treatment and was discharged. She was discharged on the following medications: metoprolol succinate 50 mg once daily and methimazole 30 mg once daily. The dose reduction of methimazole based on symptoms is as per the standard American Thyroid Association guidelines.3,4
Burch-Wartofsky Point Scale Score at the Time of Admission in September and October 2023.

Subsequent Presentation (October 2023)
With the above background history, the patient presented again to the ED with a history of fever and palpitations of 1-day duration. Of note, the patient was found to be COVID-19 positive about a week prior, when she visited her primary care physician (PCP). She had upper respiratory symptoms in the form of a runny nose, cough, and myalgias but denied any fever or shortness of breath. Given her risk factors for severe disease (Morbid obesity and Graves’ disease), she was started on oral Molnupiravir 800 mg twice daily for 5 days for her mild COVID-19 illness by her PCP. She completed her course of Molnupiravir before this presentation. She continued to take her methimazole 30 mg once daily and metoprolol succinate 25 mg once daily.
Clinical Findings
On presentation to ED, she was febrile with a temperature of 102.3°F, blood pressure of 110/70 mmHg, tachycardic with a pulse rate of 136/min, respiratory rate of 22/min, and saturating well in room air with a SpO2 OF 98%. A general physical examination revealed an anxious woman with tachycardia and fine tremors. A diffusely enlarged thyroid gland was appreciated. It was non-tender on palpation and vascular bruit was heard on auscultation. There were no features of Graves’ Orbitopathy or dermopathy on clinical examination.
Pertinent Labs and Investigations
An electrocardiogram showed sinus tachycardia. Laboratory workup revealed severe leukopenia with a white blood cell (WBC) count of 1300 cells/mm3 with an absolute neutrophil count (ANC) of 110 cells/mm3 and hypokalemia with a serum potassium of 3.3 mEq/l. TSH was <0.01 µIU/ml with an elevated T4 and T3 10.4 pcg/ml (2.1-4.1 pcg/ml), 4.34 ng/dl (0.61-1.24 ng/dl), respectively. Blood cultures were sterile. Pertinent baseline labs and follow-up labs are described in Table 2.
Laboratory Investigations Before, During, and After Index Hospitalization.
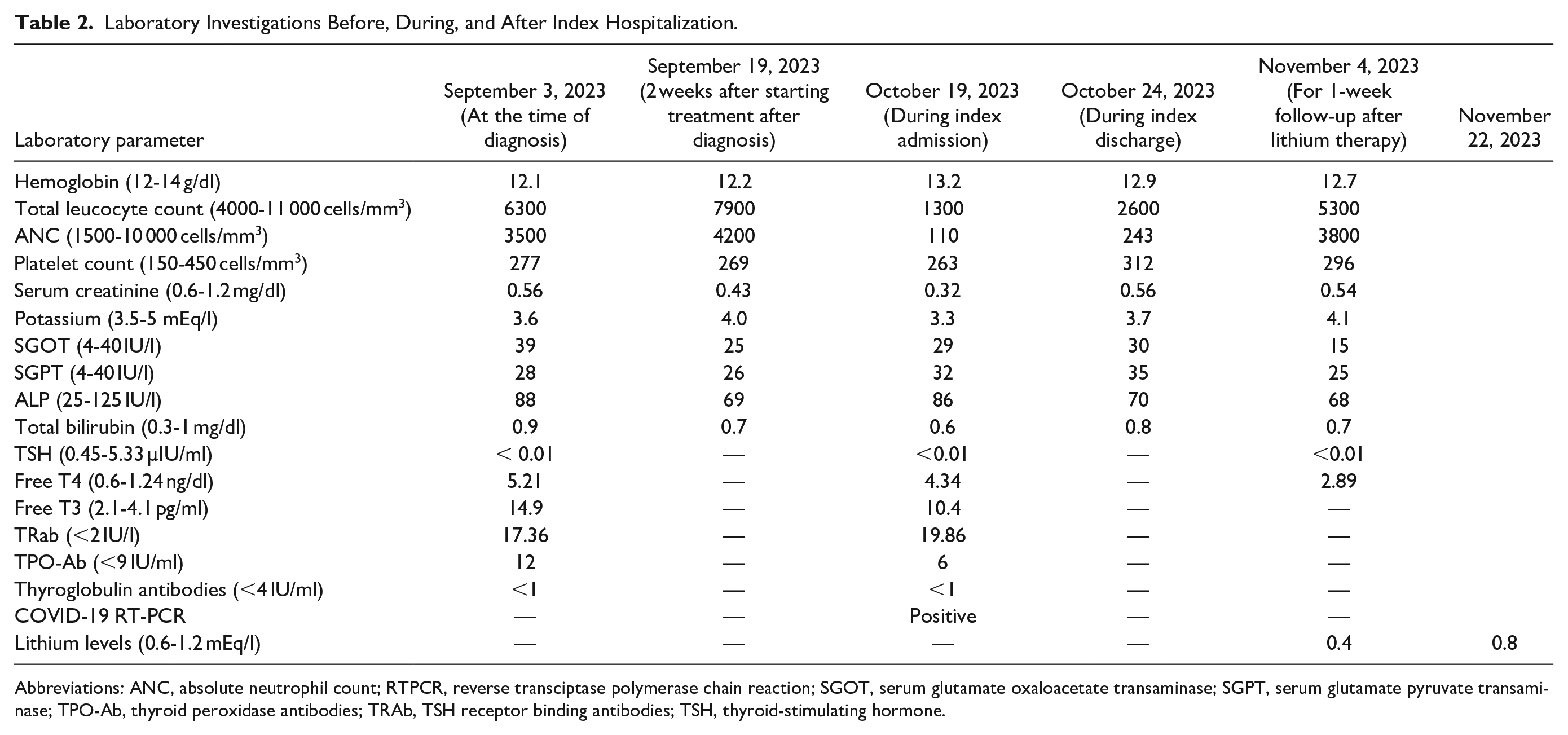
Abbreviations: ANC, absolute neutrophil count; RTPCR, reverse transciptase polymerase chain reaction; SGOT, serum glutamate oxaloacetate transaminase; SGPT, serum glutamate pyruvate transaminase; TPO-Ab, thyroid peroxidase antibodies; TRAb, TSH receptor binding antibodies; TSH, thyroid-stimulating hormone.
Hospital Course
Methimazole was withheld, given her agranulocytosis. Diagnostic possibilities considered were febrile neutropenia with sepsis, progressive symptoms related to COVID-19 infection, post-viral thyroiditis, and thyroid storm. BWPS score was 60 points, highly suggestive of thyroid storm (Table 1). So, the clinical diagnosis of the thyroid storm was made after ruling out all sources of sepsis. The thyroid storm in her case was thought to be related to Graves’ disease or post-viral thyroiditis. Non-tender thyroid gland on examination, especially in the background of known Graves’ disease, makes post-viral thyroiditis less likely. Repeat TPO and TRAb antibodies were done to differentiate Hashitoxicosis and Graves’ disease. TPO antibodies and thyroglobulin antibodies were in the normal range, but TRAb antibodies were elevated. Finally, a diagnosis of thyroid storm related to Graves’ disease was made. Thyroid scintigraphy was not done during the current admission, given her lactational status, an evident clinical picture, and supporting laboratory results. The precipitating factor in this case was identified as a recent COVID-19 infection. Adding to the conundrum is the co-existence of agranulocytosis, preventing us from using propylthiouracil and methimazole.
Treatment
The patient’s treatment plan was divided into general supportive care and specific anti-thyroid treatment. For supportive care, she started on non-selective beta-blockers (Propranolol 40 mg, 3 times daily), IV fluids, potassium supplementation, cholestyramine (4 g packets every 6 hours), and steroid therapy (IV hydrocortisone 100 mg every 8 hours) to suppress T4 to T3 conversion. An expert endocrinology consultation was obtained, given agranulocytosis and thyroid storm. She was not a candidate for acute administration of Lugol’s iodine given the contraindication for thioamide therapy, as iodine is administered only 1 hour after high-dose thioamides in thyroid storm. Given the risk for precipitating thyrotoxicosis with iodine therapy without thioamides, she was started on lithium 300 mg, 2 times daily due to the combination of neutropenia and thyroid storm after shared decision-making with the patient based on minimal available evidence. She responded to oral lithium therapy and a non-selective beta-blocker and was discharged in a hemodynamically stable state after 2 days of initiation of lithium therapy. During this admission, hypokalemia was thought to be related to hyperthyroidism, which responded to potassium supplementation. For long-term treatment options, she was given options for either surgery or radioiodine therapy. The risks and benefits of both surgery and radioiodine therapy were communicated. The patient preferred surgery over radioiodine therapy given her poor candidacy for radioiodine therapy due to lactation.
Follow-Up (November 2023)
She was asked to follow up in the clinic after 1 week. During the follow-up visit, her symptoms had resolved. Agranulocytosis resolved with a follow-up WBC count of 5300 cells/mm3. Hypokalemia resolved during follow-up. She was asked to continue lithium 300 mg, 2 times daily. Serum lithium levels were in the sub-therapeutic range, and she was not experiencing any symptoms/signs of lithium toxicity. Subsequently, the lithium dose increased to 450 mg twice daily. Emphasis was laid on definitive treatment options like thyroidectomy during follow-up, to avoid long-term lithium therapy. Lithium levels were repeated during follow-up after 2 weeks of increasing the dose of lithium and were found to be in the therapeutic range (Table 2). The patient continued to be on the same dose of lithium during the last follow-up. Since symptoms were well controlled, the patient deferred having a thyroidectomy despite explaining the toxic effects and short-term nature of the benefits of lithium therapy, and the same has been documented.
Discussion
Despite its main effects on the respiratory system, COVID-19 infection also affects other organs, including the heart, kidneys, liver, and other organs.5,6 Endocrine glands are not an exception.7,8 Infection with COVID-19 has been linked to thyroid disease. 9 Since the onset of COVID-19 in December 2019, multiple cases have been reported on the effects on the thyroid gland function, leading to hypothyroidism or hyperthyroidism. Effects on the thyroid gland are generally due to the expression of the angiotensin-converting enzyme-2 (ACE-2) on the thyroid, receptors through which the coronavirus enters the cells, and may lead to viral thyroiditis.9,10 New onset thyroid dysfunction or aggravation of an underlying thyroid pathology has been reported in COVID-19 patients, either during the active infection or later, as in our case. The thyroid abnormalities include subacute thyroiditis, euthyroid sick syndrome, thyroid storm, Hashimoto’s thyroiditis, and Graves’ disease. 11 However, the co-existent agranulocytosis and thyroid storm, as in this case, is an extremely rare combination in association with COVID-19 infection, and ours is the first case report as per our knowledge.
COVID-19 affecting the thyroid gland is postulated to be related to both direct viral toxic effects and also secondary to immune activation in the form of cytokine storm. 11 Third, the thyroid disease could be initiated by direct viral toxic effects, which are later amplified by the immune-mediated cytokine storm perpetuating the vicious cycle. 12 These viral toxic effects and subsequent cytokine release can occur either directly on the thyroid gland or at hypothalamus levels, stimulating thyrotropin releasing harmone (TRH) release and subsequently TSH release. 13 Direct effects are mediated through ACE-2 receptors, which are densely populated in the thyroid gland. Direct viral cytopathic effects through apoptosis will release damage-associated molecular patterns, which, in turn, activate proinflammatory cytokines including interleukin-1,6 and nuclear factor kappa beta (Figure 1). These mechanisms also correlate with the timing of onset of symptoms as discussed above, either during active infection (due to viral toxic effects) or later (due to immune-mediated effects). 12 Indeed, it was found that pre-existing autoimmunity, such as Graves’ disease, increases the risk of developing a thyroid storm secondary to COVID-19 infection, which is possibly due to heightened immune response due to inappropriate release of cytokines. 14 Though there is increasing evidence on the causality of COVID-19 causing new-onset thyroid dysfunction and aggravating underlying hyperthyroidism resulting in thyroid storm, evidence is still limited to case reports.15-17 Our case report is different in not only having a rare but a recognized precipitating factor like COVID-19 but also complicating the picture is the presence of agranulocytosis precluding the usage of the commonly employed anti-thyroid therapies in the management of thyroid storm. Agranulocytosis is a rare adverse effect of propylthiouracil and methimazole. The presence of agranulocytosis in this patient prevented the use of propylthiouracil/methimazole to control the thyroid storm. Another medication that is used in thyroid storm is Lugol’s iodine; however, it can only be used with thioamides given the theoretical risk of precipitating thyroid storm. 18 Though there is enough literature on iodine monotherapy usage in the long term to control hyperthyroid symptoms, its usage in the short term, especially when there is a risk of iodine precipitating thyroid storm, is questionable, as in our case. 19 Our patient, not being a candidate for the above therapies, lithium was considered as an option that counteracts thyroid storm and leukopenia through different mechanisms. Combined use of lithium and iodine has been reported in thyrotoxicosis, and lithium has been studied along with radioiodine therapy for hyperthyroidism, but we did not come across much published evidence for the use of lithium and iodine in thyroid storm.20,21

COVID-19 induced cytokine-thyroid storm leading to increased levels of T3/T4 release from the thyroid gland, which, in turn, upregulates the production of the cytokines from the macrophages and other immune cells, leading to a vicious cycle of a cytokine storm and thyroid storm. Lithium affects the thyroid gland function through multiple mechanisms. It does that by inhibiting iodine uptake, inhibiting TSH signaling, including thyroglobulin conformational change, inhibiting iodotyrosine binding, and inhibiting the peripheral conversion of T4 to T3. TSH, thyroid-stimulating hormone.
It is imperative to know the mechanism of action of lithium in this setting. First, lithium accumulates in the thyroid gland through the Na/I transporter, leading to levels 3 to 4 times higher than serum levels, and later inhibits the synthesis of the thyroid hormone through multiple mechanisms 22 (Figure 1). Lithium inhibits the cyclic adenosine monophosphate molecule, the secondary messenger of the TSH hormone that upregulates thyroglobulin synthesis. Lithium also causes conformational changes in thyroglobulin protein, decreases iodine uptake, and decreases iodotyrosine binding to thyroglobulin, leading to decreased T3 and T4 synthesis. Third, lithium inhibits the activity of the 5-deiodinase enzyme, decreasing the peripheral conversion of T4 to T3 22 (Figure 1). These effects are observed in acute lithium treatment and can be used as an alternative to thioamides in the treatment of thyroid storms when the use of the standard treatment is not feasible. In the index patient, though initial lithium levels are subtherapeutic, there is still a partial response to symptoms. Improvement could also be attributed to beta-blockers along with lithium therapy.
However, one important consideration before starting lithium therapy is that patients who are positive for thyroid antibodies like thyroperoxidase (TPO-Ab) and thyroglobulin (TG-Ab), seen in the Hashitoxicosis phase of Hashimoto’s thyroiditis, have a higher chance of developing hypothyroidism secondary to lithium therapy. 22 So it is always important to differentiate Graves’ disease versus the Hashitoxicosis phase of Hashimoto’s thyroiditis before starting treatment. Our patient is negative for both TPO-Ab and TG-Ab, ruling out Hashimoto’s thyroiditis. Even though it is less common, hyperthyroidism can also occur secondary to lithium treatment. The incidence of lithium-induced hyperthyroidism ranges between 0.1% and 1.7%. Multiple theories have been proposed to explain the mechanism of lithium-induced hyperthyroidism, including the direct toxic effect of lithium on the thyroid tissues, leading to destruction and thyrotoxicosis, Jod-Basedow phenomena, and increased TPO-Ab and TG-Ab secondary to increased activity of the B-cell lymphocytes. 22 Lithium-induced hypothyroidism is reversible in most patients after the discontinuation of lithium, giving it an advantage for use in treating hyperthyroidism in thyroid storms. 23
The limitation of this case report is establishing the causality of agranulocytosis and thyroid storm. Though leukopenia occurs in the setting of COVID-19 infection, severe neutropenia with an ANC of 110 cells/mm3 made us attribute it to methimazole. Also, repeat COVID-19 testing is not valuable in such a scenario, as there is no evidence to establish a linear relationship between COVID-19 viral clearance and WBC count improvement. Though COVID-19 is a directly identifiable precipitating factor for a thyroid storm, other factors like the use of iodine a month ago, and poorly controlled Graves’ disease may have an add-on effect in precipitating the storm.
Conclusion
COVID-19 is a recognized precipitating factor for thyroid storm. It is very rare to see co-existent thyroid storm and agranulocytosis, and lithium can be a useful option in such cases if not contraindicated. This case report adds to the minimal literature existing on lithium use in patients with thyroid storm after an expert opinion and shared decision-making.
Footnotes
Acknowledgements
None.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Prior Presentation of Abstract Statement
The abstract of the case report was presented at the National American College of Physicians (ACP) meeting 2024 in Boston on April 18, 2024, as a poster finalist.