
Abstract
Co-infection with Mycobacterium tuberculosis and Aspergillus in an immunocompetent host is rare but can occur. In this case, we present a patient with central nervous system tuberculosis (TB) and biopsy-proven spinal co-infections with TB and Aspergillosis. We highlight the complexities of treating a TB-Aspergillosis co-infection given drug-drug interactions between standard therapy for both conditions. Using susceptibilities for the Aspergillus and carefully monitoring drug levels of the antifungal agents, we were able to optimally treat the co-infection. This patient was ultimately discharged on isoniazid 1200 mg (15 mg/kg) daily, levofloxacin 750 mg daily, rifabutin 450 mg daily, and posaconazole 300 mg twice daily with a tentative plan to treat for at least 1 year with close outpatient follow-up. This case can serve as a guide for other providers who need to treat cases of TB and Aspergillosis co-infection by learning from our experience and paying attention to potential pitfalls.
Introduction
Vertebral osteomyelitis from Aspergillosis in healthy patients who are not immunocompromised can occur but is rare. 1 Aspergillus is an opportunistic fungal infection that typically affects the respiratory tract but can have a wide variety of presentations. 2 Aspergillus can affect both the central nervous system (CNS) 3 and the spine. 4 Some reports have shown that invasive aspergillosis in the thoracic spine is often misdiagnosed as spinal tuberculosis (TB). 5 TB of the spine is considered the most common cause of non-traumatic spinal cord injury in developing countries and can present with back pain, night sweats, and fever among other systemic symptoms. 6 In our case, the patient was experiencing intermittent mid to low thoracic back pain that was not improving with over-the-counter medications. The diagnosis of spinal TB with concomitant aspergillosis in immunocompetent patients is usually unexpected and therefore not actively sought after. Hence, only a few reports are available. Herein, we report a case of an immunocompetent male patient who had Mycobacterium tuberculosis in both the brain and spine and Aspergillus co-infection in the thoracic spine. Concomitant treatment of these 2 infections can be challenging due to drug-drug interactions and host-driven medication dose adjustments, as illustrated in our case.
Case Description
A 36-year-old Indonesian male was brought to the emergency department for 2 weeks of intermittent and worsening fevers and headaches. The patient was encephalopathic on the initial exam in the emergency room; therefore, the initial medical history was limited and taken from his brother-in-law. The history suggested that the patient had been experiencing intermittent mid to low thoracic back pain for over 1 month that had not resolved with over-the-counter remedies. He also had fevers and a headache for approximately 2 weeks before coming into the hospital. Just before his diagnosis, the patient was working on a cruise ship that traveled from Asia to the Bahamas and Mexico. His job included bringing beverages to clients on the cruise. He was actively working one evening when he became acutely confused and had to be brought in directly to the nearest medical facility.
The patient’s initial presentation revealed a young, toxic-appearing encephalopathic male with no known past medical history. His vital signs at the time of evaluation were unremarkable except for a fever of 39.7°C, heart rate of 76 bpm, respiratory rate of 20 breaths/min, blood pressure of 127/72 mmHg, and oxygen saturation of 98% on room air. The physical exam was unremarkable, as well, other than the patient’s somnolence and inability to cooperate with questioning. The patient had a normal complete blood count with a white blood cell count of 10.2 × 10(3)/µL (normal range 4-10.5 × 10(3)/µL), hemoglobin of 13.7 g/dL (normal 13.3-16.3 g/dL), hematocrit of 39% (normal 39%-47.1%), and platelets of 324 × 10(3)/µL (normal 140-400 × 10(3)/µL). His blood urea nitrogen was 13 mg/dL (normal 9-20 mg/dL), creatinine was 0.7 mg/dL (normal 0.66-1.25 mg/dL), and serum glucose was 115 mg/dL (normal 74-106 mg/dL). Initial testing was negative overall and included blood cultures, a respiratory viral panel, HIV screening, an MRI brain, and a chest X-ray. A QuantiFERON was sent due to the patient’s recent travel history to endemic areas, his altered mental status, and his place of origin being Indonesia. A lumbar puncture was also performed due to acute altered mental status, and cerebrospinal fluid (CSF) was sent for fungal culture, bacterial culture, cell count, fluid analysis, stain and culture for acid-fast bacilli, Mycobacterium tuberculosis (MTB) PCR complex, and a meningoencephalitis panel.
At this time, the patient was started on empiric viral, fungal, and bacterial meningitis therapy. The CSF analysis noted an elevated total nucleated cell count of 395 µL (normal range 0-5/ µL), 159/mm3 red blood cells (normal 0/mm3), low glucose of 27 mg/dL (normal 40-70 mg/dL), high total protein of 451 mg/dL (normal 15-45 mg/dL), 15% neutrophils (normal 0-6%), and lymphocytic pleocytosis with 85% lymphocytes (normal 40%-80%). The QuantiFERON (QFT-Nil 0.24 International Unit/mL, QFT-TB1 minus Nil 2.23 International Unit/mL, QFT-TB2 minus Nil 2.19 International Unit/mL, QFT-Mitogen minus Nil 3.89 International Unit/mL) test was positive. The computed tomography (CT) of his thoracic spine reported findings consistent with T10 to T11 discitis/osteomyelitis with possible phlegmon. The chest CT revealed multiple nodular opacities in the right lung apex, suspicious for pulmonary manifestations of TB. Other differential diagnoses of the nodular lung infiltrates considered include community-acquired pneumonia, lung abscess, septic pulmonary emboli, acute fungal pneumonia such as histoplasmosis or coccidioidomycosis, and non-infectious etiologies such as sarcoidosis and primary or metastatic lung cancer. Interventional radiology was subsequently consulted for aspiration and/or biopsy of the disc space and bone. The T10 to T11 biopsy of the vertebral collection revealed a few acid-fast bacilli on smears and a positive MTB GeneXpert PCR. The empiric antibiotics were discontinued, and CNS TB meningitis/TB osteomyelitis therapy was started alongside steroids. The patient was initiated on rifampin 600 mg IV daily, pyrazinamide 2 g IV daily, pyridoxine 50 mg PO daily, ethambutol 2000 mg (25 mg/kg) PO daily (dosed for empiric treatment of multi-drug resistant (MDR) TB due to patients’ Indonesian background), isoniazid 1200 mg (15 mg/kg) IV daily (dosed for empiric treatment of MDR TB), levofloxacin 750 mg IV daily, linezolid 600 mg IV BID, as well as dexamethasone 6 mg daily.
Several days after initial admission and commencement of anti-TB therapy and steroids, the patient improved even though he still complained of a headache, remained mildly somnolent, and was intermittently confused. A daily review of infectious testing exhibited a positive mold result from the thoracic spine biopsy mycology microbiology report. Thus, intravenous liposomal amphotericin was started.
Eight days after the spinal biopsy, specimens started growing Aspergillus flavus/oryzae in addition to acid-fast bacilli. Amphotericin B was switched to voriconazole for more targeted Aspergillus coverage, and rifampin was changed to rifabutin to mitigate the interaction with azoles. However, the strong interaction between voriconazole and rifabutin still caused the voriconazole trough levels to remain undetectable. 7 Voriconazole was then switched to isavuconazole because it exhibits the least strong drug interaction with rifabutin among the triazoles. 8 One week later, drug susceptibilities for the Aspergillus returned with minimum inhibitory concentrations (MICs) for voriconazole of 0.5, posaconazole of 0.06, and isavuconazole of 0.5. The decision was then made to switch isavuconazole to posaconazole because it had the lowest MIC. Since posaconazole also has a strong interaction with rifabutin, 9 the posaconazole dose was increased to 300 mg twice daily to target trough levels greater than 2 µg/mL. The susceptibilities for the M. tuberculosis isolated from the thoracic spine biopsy also came back. It was a pan-susceptible isolate with MICs of 0.5 to linezolid, levofloxacin, and moxifloxacin. No rpoB mutation was identified.
As part of patient follow-up, a repeat MRI of the brain and CSF analysis were performed. The brain MRI revealed extensive leptomeningeal enhancement, and compared to the previous study there was increasing hydrocephalus with associated trans ependymal CSF flow. The patient’s CSF studies from his initial lumbar puncture came back positive for M. tuberculosis. A repeat CSF culture and MTB PCR were also positive, confirming MTB meningitis as well as Pott’s disease (spinal TB). This patient’s background and past medical history were unremarkable except for coming from an endemic area, which does not automatically predispose that population to such an invasive disease. No evident diagnosis or history of immunosuppression was uncovered by either the patient or his family history. The patient continued to improve. His persistent headaches resolved, and he was later able to be discharged on an oral regimen of isoniazid 1200 mg (15 mg/kg) daily), levofloxacin 750 mg daily, rifabutin 450 mg daily, and posaconazole 300 mg twice daily with a tentative plan to treat for at least 1 year with close outpatient follow-up. Repeat imaging at almost 2 months with an MRI of the thoracic spine showed improvement but continued enhancement at T10 and T11 (see Figure 1).
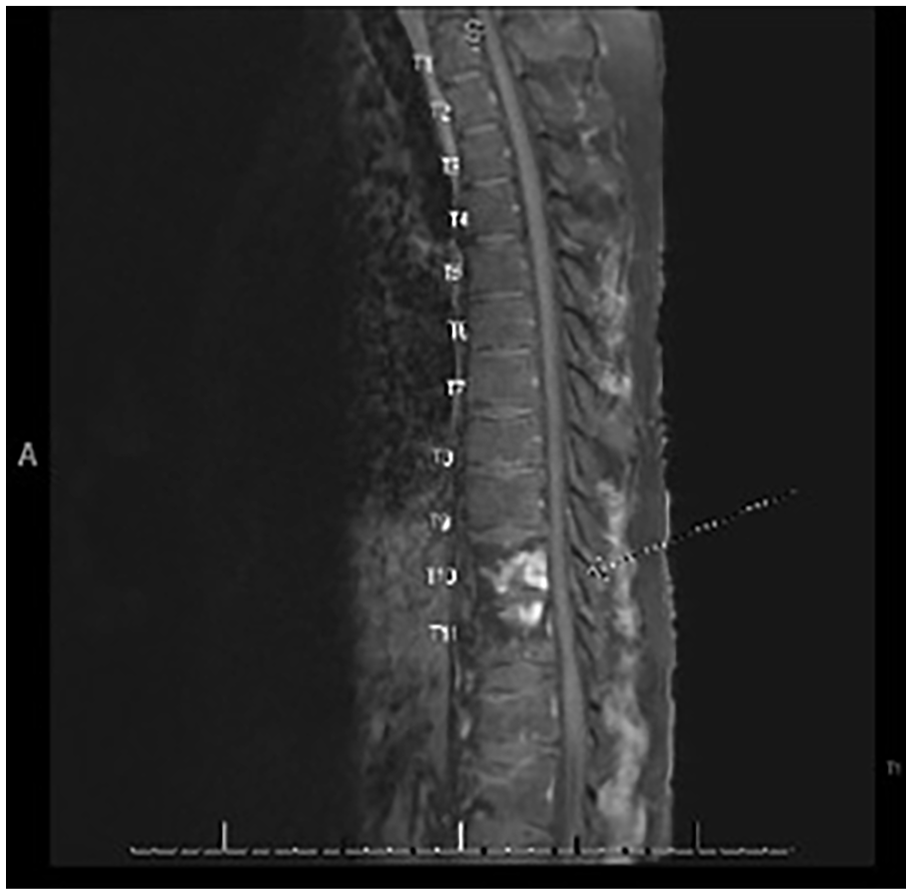
MRI of the thoracic spine with and without contrast shows enhancement and T2/STIR signal at the T10 and T11 vertebral bodies.
Discussion
This patient had both CNS/spinal TB and Aspergillosis co-infection. This co-infection is an extremely rare phenomenon, particularly in immunocompetent patients. This case illustrates both the diagnostic and therapeutic challenges associated with this unusual combination of pathogens in a young immunocompetent individual, highlighting the importance of utilizing culture data and drug levels to optimize treatment.
M. tuberculosis is a pathogen that typically affects the lungs but can spread to other organs, including the CNS and axial skeleton, through hematogenous dissemination. 10 CNS TB, although rare, can manifest as tuberculous meningitis or Pott’s disease. 11 Aspergillus, on the other hand, is an opportunistic fungus that commonly infects the respiratory tract, especially in immunocompromised individuals.12,13 Invasion of the bone by Aspergillus is extremely rare and typically affects immunocompromised hosts. 4
Co-infection with Aspergillosis and TB among immunocompetent hosts is uncommon. 14 The exact percentage of co-infection with Aspergillus in patients with TB, especially in immunocompetent individuals, is not well documented in the literature. Most cases and studies focus on immunocompromised patients, such as those with HIV/AIDS, 15 transplant recipients, 16 individuals on long-term corticosteroid therapy, 16 or those with cancer. 17 However, based on available data, the occurrence of Aspergillus co-infection in patients with TB in general varies. A study with participants from Africa and Asia found an incidence of 15.4% for co-infection with pulmonary TB and Aspergillosis. 18 The precise prevalence of TB and Aspergillus co-infection among immunocompetent individuals is difficult to pinpoint due to the scarcity of cases and varying diagnostic criteria; therefore, further studies are needed. 19
In this case, the patient did not have a history of immunosuppression, HIV, steroid use, diabetes mellitus, malignancy, or other predisposing conditions. However, his origin from an endemic area and recent travel suggest exposure to both pathogens. Although he had no pulmonary symptoms, chest imaging revealed nodular opacities, suggesting possible latent pulmonary TB.
The diagnosis of co-infection was complicated by overlapping symptoms and a predominantly neurological presentation. The CSF analysis showed characteristics consistent with tuberculous meningitis, such as low glucose, high protein, and lymphocytic pleocytosis. 20 A definitive diagnosis of spinal TB was confirmed through a thoracic spine biopsy, which showed acid-fast bacilli. Subsequently, Aspergillus was also identified in the same biopsy cultures, pointing toward the need for a thorough evaluation of tissue samples in complex infection cases. We reinforce the need for vertebral and paravertebral biopsy tissues to be sent for fungal cultures and histopathology in addition to routine mycobacterial stains, PCR, and cultures in all cases of vertebral osteomyelitis. 21
Treatment was complicated by interactions between anti-tuberculosis and antifungal medications. Initially, amphotericin B was administered before the speciation of the fungus. However, once A. flavus/oryzae was identified, and treatment was refined to the drug of choice for Aspergillosis, which is voriconazole. Among the triazoles, voriconazole has the strongest drug interaction with rifamycins, followed by posaconazole and isavuconazole, which is the least. When using these drugs together, it should be done cautiously. 22 Coadministration of these antifungals can increase the concentration of rifamycin, and at the same time, rifamycins can decrease the concentrations of these triazoles. In our case, we observed undetectable levels of voriconazole while administering rifabutin and it was not until we switched to higher doses of posaconazole, twice daily dosing, that we were able to achieve therapeutic levels.13,23 In addition, the patient is from Indonesia. Previous data have shown that individuals from Indonesia may be rapid or intermediate metabolizers, due to genetic polymorphisms in the CYPC2C19 gene which codes for the enzyme involved in voriconazole metabolism. 24 There are data to suggest that CYP2C19 genotyping may aid in voriconazole dosing and monitoring. 25
The patient’s final regimen included a combination of anti-tuberculosis drugs (rifampin, isoniazid, pyrazinamide, ethambutol, levofloxacin, and linezolid) and posaconazole for the fungal infection. The addition of steroids helped manage CNS inflammation.26,27 The patient showed significant clinical improvement with the resolution of encephalopathy and persistent headache. He was discharged on an oral regimen, underscoring the efficacy of the combined treatment and the importance of close monitoring. 14 This case also highlights the importance of thorough diagnostic vigilance, utilizing culture data, and drug monitoring to avoid mortality. 28
In summary, we have highlighted the challenges in the diagnosis and management of TB-Aspergillosis co-infection in an immunocompetent patient. Our case reinforces the need to include fungal cultures, mycobacterial cultures, and MTB PCR in the analysis of biopsy specimens obtained from patients with back pain and abnormal imaging compatible with diskitis/osteomyelitis. Concomitant use of antifungal (especially azoles) and anti-tuberculosis drugs requires close drug monitoring and expert care including the input of an infectious diseases pharmacist. CYP2C19 genotyping may aid in voriconazole dosing, monitoring, and management of these complex cases.
Footnotes
Acknowledgements
We would like to thank the patient for allowing us to publish this case, April Mann, and the University of Miami Writing Center for editorial support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.