
Abstract
An 18-year-old teenager with significant atherosclerotic cardiovascular disease (ASCVD) risk factors developed acute chest pain. His electrocardiogram showed inferior ST-segment elevations. Emergent coronary angiogram revealed complete thrombotic occlusion of the right coronary artery. He underwent stenting of the culprit lesion with complete clinical recovery and resolution of his electrocardiographic abnormalities secondary to myocardial infarction.
Keywords
Case Presentation
An 18-year-old teenager with PMHx of obesity (body mass index [BMI] 37 kg/m2), hypertension, type 2 diabetes mellitus, seizure disorder, bipolar disorder, and recent suicide attempt presented to an emergency department with acute complaints of 9/10 severity sharp, nonradiating left-sided substernal chest pain associated with shortness of breath ongoing for 1 hour. His physical examination revealed a young man in obvious respiratory distress, with corresponding vital signs: respiratory rate, 24 breaths/min; oxygen saturation, 96% on room air; temperature, 98.5°F; blood pressure, 180/120 mm Hg; and heart rate, 104 beats/min. Glascow coma score (GCS) 15. Of note, patient and parents endorsed that his blood pressure has been very high recently and noncompliant with metformin and lisinopril medications. In addition, patient had presented with similar complaints 1 year prior, with unrevealing electrocardiogram (EKG) and troponin, so further workup was not pursued. Blood sugar was 396 mg/dL enroute to the ED per EMS. Recent A1c was 11.7. Diabetes and hypertension were diagnosed at 16 years old, and he had not been compliant with lisinopril or metformin since diagnosis. Family history significant for diabetes and hyperlipidemia in maternal grandmother and hypertension in mother. Denied any additional personal or family history of cardiac disease. Denied any recent drug use but endorsed remote cocaine use. No history of cigarette use or smokeless tobacco. Heart auscultation revealed normal rate, regular rhythm, normal heart sounds, and intact distal pulses. No murmurs, gallop, or pericardial rub. No crackles were appreciated on lung auscultation. The rest of his examination was normal. Upon receiving sublingual nitroglycerin, his pain completely subsided. EKG obtained in the emergency department revealed Inferior ST elevation myocardial infarction and reciprocal ST depression in lead aVL (Figure 1). Patient was immediately placed on O2 and telemetry. 325 mg Aspirin, 600 mg Plavix, IV Heparin, and morphine were initiated. Initial cardiac troponin I (cTnI) was normal (<0.03 ng/mL) but creatine kinase-myocardial band (CK-MB) levels were elevated (113.0 U/L). Other significant labs included elevated blood glucose (308 mg/dL), elevated alanine aminotransferase (ALT; 221 U/L), elevated aspartate aminotransferase (AST; 76 U/L), elevated AlkPhos (154 U/L) elevated red blood cell (RBC) count (6.44 M/uL), elevated Hb (16.7 g/dL), and elevated Hct (51.3%). Bedside echocardiogram revealed moderate inferior and mild inferoseptal wall hypokinesis with an ejection fraction of 50% to 55%. He was emergently rushed to the cardiac catheterization laboratory where he was noted to have multivessel disease, complete obstructive stenosis (100%) of distal RCA (right coronary artery), along with moderate stenosis (50%-70%) in the mid segment of LAD (left anterior descending artery) and septal diagonal artery. Right coronary artery was noted to be the culprit vessel. He subsequently underwent percutaneous coronary intervention (PCI) to distal RCA with restoration of TIMI 3 flow using bifurcation stenting technique to rPLV and rPDA branches (Figures 2 and 3). Hypercoagulable workup panel came back normal. Post op lipid panel revealed elevated total cholesterol (211 mg/dL), triglycerides (178 mg/dL), and low-density lipoprotein (LDL; 142 mg/dL) and decreased high-density lipoprotein (HDL; 33 mg/dL). Laboratory summary denoted in Table 1. Loading dose of Aspirin and Plavix were discontinued and patient was started on Aspirin 81 mg, Prasugrel 10 mg, Lipitor 80 mg, Coreg 3.125 mg, Lisinopril 20 mg, sliding scale insulin, and Trileptal 300 mg. Lovenox was given for deep vein thrombosis (DVT) prophylaxis. Postoperative hospital course was uneventful, and he was subsequently discharged home 5 days later. At 6 years follow-up, his blood pressure remained elevated in the stage 2 hypertension range despite prescribed Lisinopril. Diabetes remained uncontrolled with A1c of 14.4, despite prescribed Metformin, Jardiance, and Glimiperide, Medication compliance has been challenging due to various socioeconomic factors. Of note, due to history of elevated liver enzymes (ALT 103 U/L), Lipitor was decreased to 40 mg. 6-year follow-up lipid panel revealed elevated Triglycerides (431 mg/dL), Cholesterol (226 mg/dL), and borderline HDL (38 mg/dL), LDL (120 mg/dL). He has developed diabetic neuropathy with occasional urinary incontinence, gastroparesis, and sensory neuropathy. Metformin and Glimepiride were stopped; Jardiance was increased; and Insulin Lantus, Acarbose, and Gabapentin were added to her diabetic medication regimen. Lipitor was switched to Crestor 40 mg and Lisinopril was increased to 40 mg for his cardiovascular medication regimen. He has not experienced recurrent cardiac events.
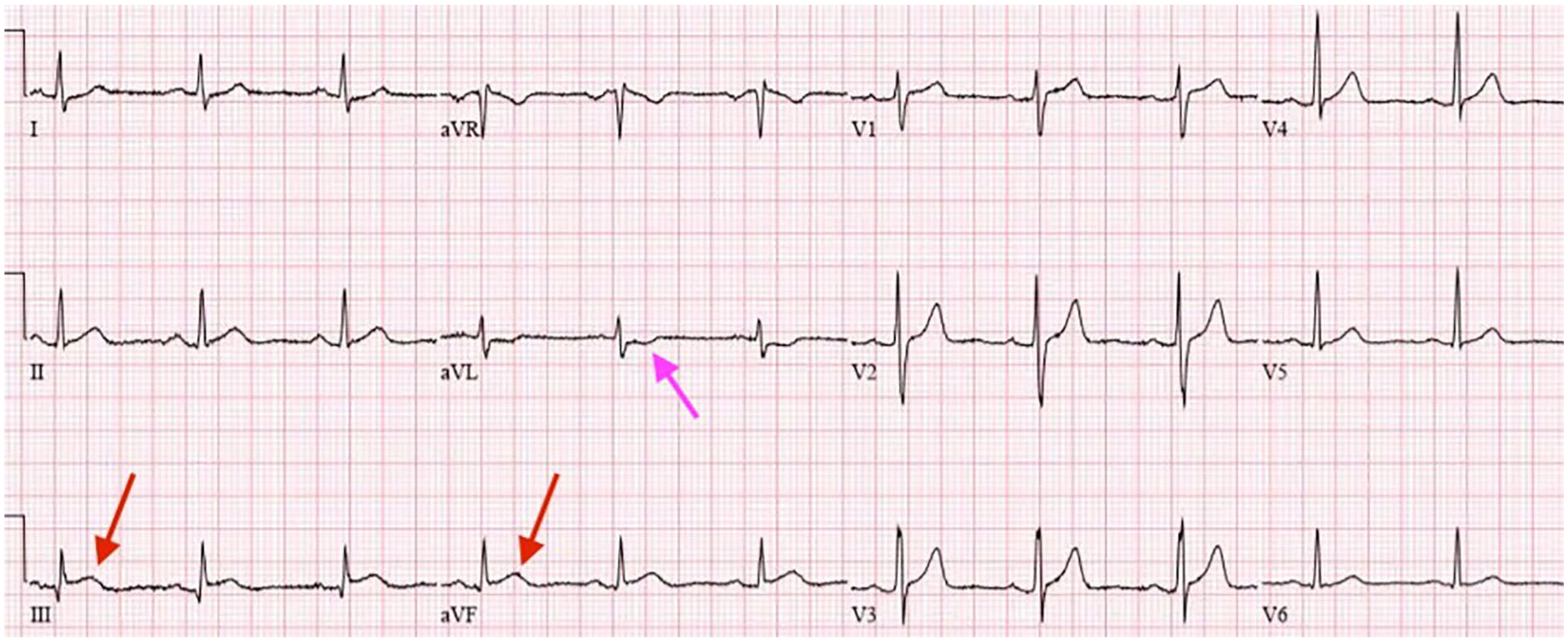
Twelve-lead ECG on presentation showing changes consistent with acute inferior ST-elevation myocardial infarction (STEMI red arrow) with reciprocal ST depression in lead aVL (pink arrow).

Angiographic images of the right coronary artery (RCA) before and after percutaneous intervention. Critical obstructive distal RCA (green arrow) and moderate right posterior descending artery (rPDA) and posterior left ventricular artery (pLV) stenosis with plaque rupture before stenting.
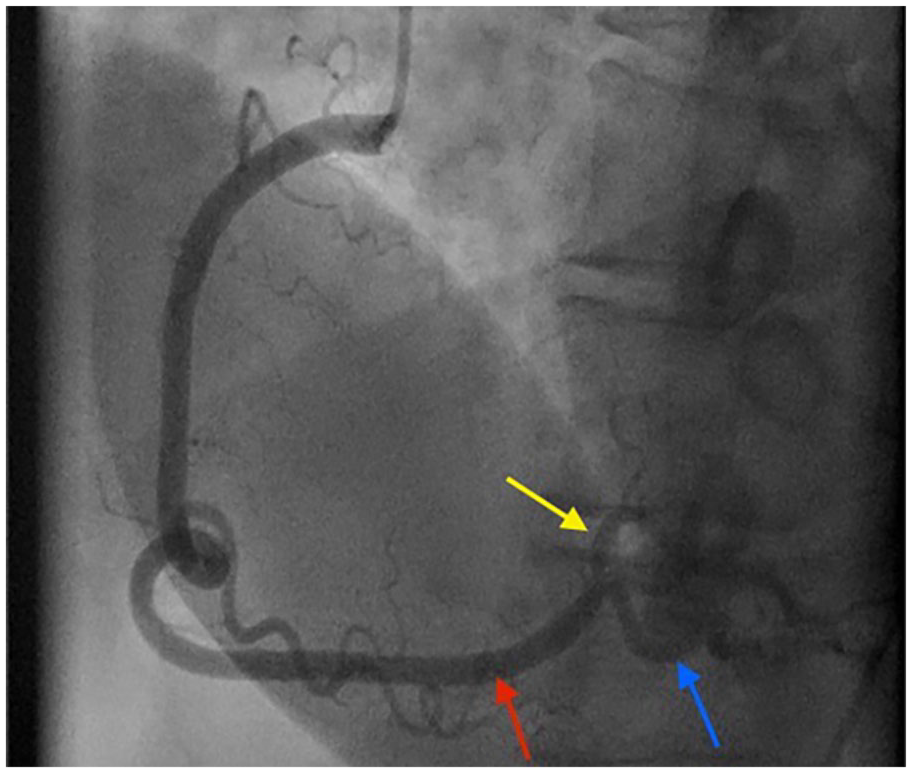
Subsequent appearance after percutaneous coronary intervention with bifurcation stenting of distal RCA (red arrow) to pLV (yellow arrow) and rPDA (blue arrow).
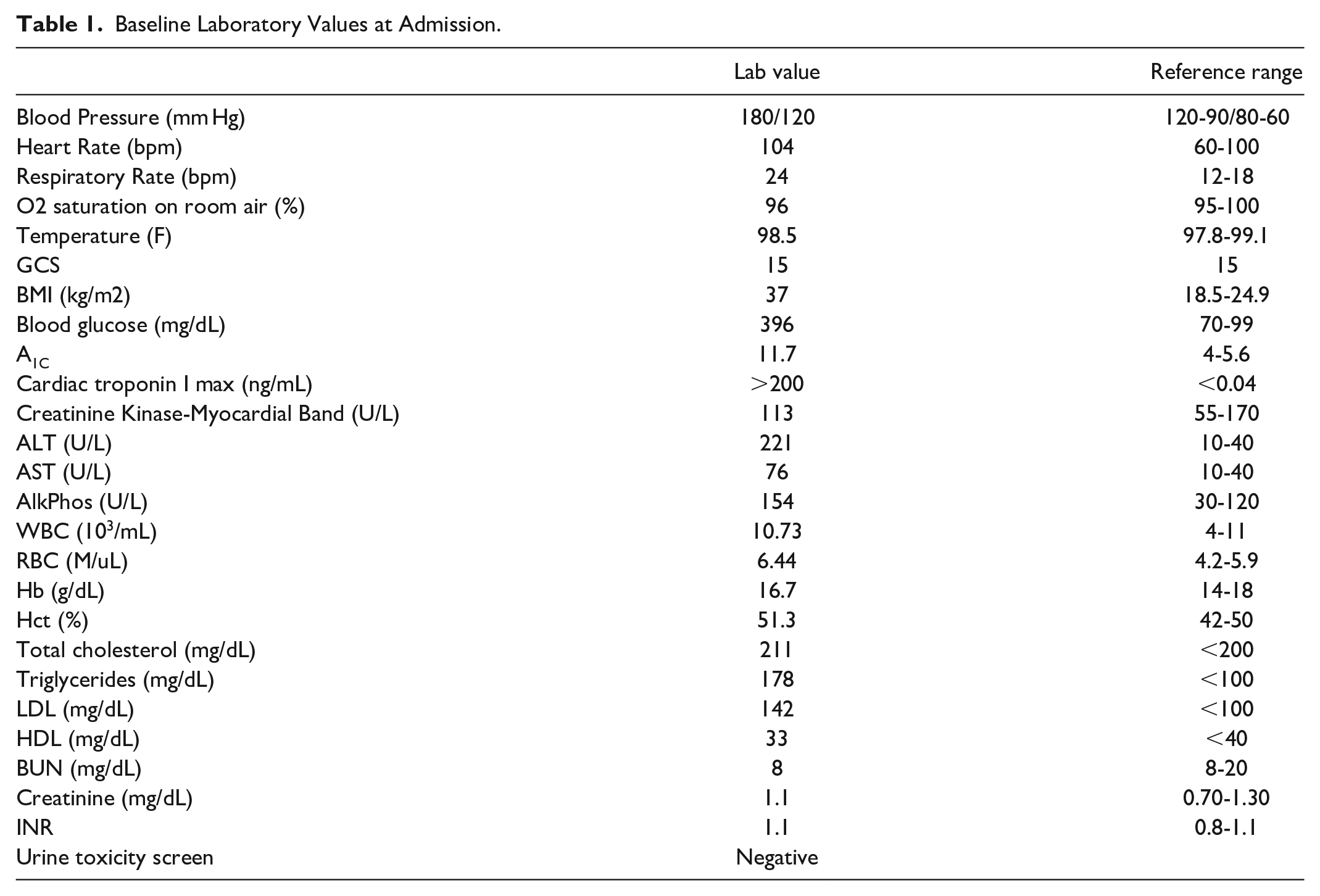
Baseline Laboratory Values at Admission.
Discussion
Recent reports by the American Heart Association indicate that mean age of first acute myocardial infarction in the United States is 65.6 years for men and 72 years for women. 1 But in the last few decades, several studies have shown an increased incidence of coronary artery disease (CAD) in young people. A retrospective analysis based on 2016 to 2020 National Inpatient Sample recorded 2170 hospitalizations for acute myocardial infarction in teenagers. 2 It is estimated that approximately 10% of CAD presenting as acute myocardial infarction occur in patients 45 years of age or younger, defined as premature disease. 3
However, as seen in our patient and other cases, CAD is presenting nearly 2 to 3 decades earlier, and there is limited research on age-specific risk factors causing this paradigm shift. Outcome data from long-term follow-up studies is particularly important in the adolescent population and is currently lacking. We need to know more about the natural history, unique risk factors, and long-term prognosis for this young population to have guideline directed treatment options to prevent early morbidity and mortality.
It is well-known that atherosclerosis starts at a young age and with childhood obesity becoming an epidemic in certain regions of the United States, the number of young individuals developing atherosclerosis is on the rise. Multiple studies have shown that smoking, lipid disorders, and family history of premature CAD are the most important risk factors in patients with premature myocardial infarction, smoking by far being the most prevalent and modifiable. 3 Hyperlipidemia in particular has been on the rise in recent decade. 4 All 2023 data from the USPSTF pooled analysis of 36 030 participants from 6 U.S.-based cohort studies with a median follow-up period of 17 years studied the independent association between exposure to high lipid levels in young adults age 18 to 39 years and later cardiovascular events; results showed LDL >100 mg/dL in adolescents was associated with 1.64 HR for coronary heart disease compared to those with levels <100 mg/dL. 5 Research shows that more than half of patient with premature CAD have dyslipidemia, with high LDL, low HDL, and higher lipoprotein(a). In fact, lipoprotein(a) >50 mg/dL is associated with a 3× higher likelihood of premature disease. 3
Although the 2019 American College of Cardiology/American Heart Association (ACC/AHA) Guideline on the Primary Prevention of Cardiovascular Disease recommends assessment of cardiovascular risk beginning at age 20 years, 6 the published ACC/AHA ASCVD risk calculator is unable to compute scores before age 40. 7 Recommendations regarding lipid and cholesterol screening of pediatric/adolescent populations, initiation of statin therapy for hyperlipidemia treatment, and referral to a specialist for further management remains unclear. 8 Current primary prevention recommendation for pediatric population between age 0 to 19 focuses on lifestyle modification. Statin initiation is only indicated if there is a diagnosis of familial hypercholesterolemia (FH). 6 According to 2018 guidelines, adolescents older than age 10 with LDL > 190 or LDL > 160 with clinical presentation persistent with FH who do not respond to 3 to 6 months of lifestyle therapy (caloric restriction and 30-60 minutes vigorous physical activity daily) can be started on statin therapy. 9 Multifactorial dyslipidemia is defined as elevated levels of LDL (≥130 mg/dL) or TC (≥200 mg/dL) that is not attributable to FH. Multifactorial dyslipidemia onset in adulthood is widely established as a risk factor for cardiovascular disease and ischemic heart disease mortality, but little is known regarding its long-term effects on the adolescent population. 10 Regarding children and adolescents, the USPSTF found inadequate evidence on the benefits of lipid-lowering intervention for multifactorial dyslipidemia to reduce adverse health outcomes. 5 But importantly, there is no current guidelines on the role of statin therapy in patients with multifactorial dyslipidemia and ASCVD risk factors such as diabetes. According to American Diabetes Association Standards of Care 2023 Report, after the age of 10 years, addition of a statin may be considered in youth who despite medical nutrition therapy and lifestyle changes, continue to have LDL cholesterol >160 mg/dL (4.1 mmol/L) or LDL cholesterol >130 mg/dL (3.4 mmol/L) and one or more cardiovascular disease risk factors such as diabetes. If fasting triglycerides are >400 mg/dL or nonfasting triglycerides >1000 mg/dL, fibrate therapy can be initiated. Owing to the potential teratogenic effects of statin, adolescents of childbearing age should receive reproductive counseling regarding reliable contraception. Initial therapy should always consist of optimizing hyperglycemia with target HbA1C < 7%, nutritional therapy by limiting the amount of calories from fat to 25% to 30% and saturated fat to <7%, limiting cholesterol <200 mg/day, avoiding trans-fat, and aiming for ~10% calories from monounsaturated fats for elevated LDL. Optimal goals are LDL <100 mg/dL, HDL cholesterol >35 mg/dL, and triglycerides <150 mg/dL. 11 In the case of our patient, he did have a prior diagnosis of type 2 diabetes and intensive lifestyle intervention focusing on weight loss, dyslipidemia, hypertension, and dysglycemia should have been the mainstay intervention to prevent such overt macrovascular disease in early adulthood. Unfortunately, there are no records of his lipid profile prior to his major adverse cardiovascular event; early screening of elevated lipid levels given his early onset diabetes very likely could have been indication for statin therapy and could have prevented his premature CAD and myocardial infarction. This case emphasizes the importance of close supervision and screening of lipid disorders in children and adolescents with ASCVD risk factors and routine monitoring of blood pressure, nonfasting total cholesterol/HDL/LDL/very-low-density lipoprotein [VLDL]/Triglycerides, nonfasting HbA1C and BMI should be considered. In addition, according to the 2019 ACC/AHA guidelines, the use of noninvasive imaging tests such as coronary artery calcium assessment can serve as a potential guide to identify high-risk populations and prevent further progression of CAD. 6 Younger adults, often do not display calcium buildup and may require additional testing with computed tomographic angiography to help identify remodeling and necrotic aspects of plaques associated with increased risk of coronary events. 12 The American Academy of Pediatrics also suggests that assessment of preclinical atherosclerosis with alternative vascular measurements such as carotid artery intima-media thickness (cIMT), aortic pulse wave velocity (PWV), and endothelial function with peripheral arterial tonometry (PAT) may aid in future risk management. 13
Differential Diagnosis
While focus on traditional risk factors leading to obstructive CAD in these young individuals is necessary, it also important to rule out the other pathophysiologic mechanisms for MI which can be grouped into 4 other categories: (1) use of recreational drugs such as cocaine and methamphetamine, (2) coronary vasospasm, (3) MI due to atheromatous CAD but without critical coronary stenosis, and (4) MI due to SCAD, myocarditis, or coronary embolism. 14 Our case did not demonstrate any of these additional pathophysiologies.
Although the prognosis for young patients with MI is not completely benign, younger patients have a favorable in-hospital mortality profile compared to older patients. 15 Nonetheless, such patients are at increased risk of future ischemic events with mortality as high as 30% at 15-year follow-up.10 These data underscore the importance of earlier interventions to positively modify the risk factor profile and lifestyle approaches in younger patients presenting with MI.
Conclusion
This case describes an 18-year-old male who presented with ST elevation myocardial infarction (STEMI). Coronary artery disease and myocardial infarction is extremely rare in adolescents. Unfortunately, due to alarmingly high rates of obesity, diabetes, and hyperlipidemia in our young population, symptomatic atherosclerotic disease is presenting very prematurely as in our patient; acute coronary syndrome (ACS) should remain in the differentials. Atherosclerosis has revealed its pediatric face and unmanaged obesity, diabetes, hyperlipidemia, and hypertension should not be taken lightly as it can cause myocardial infarction as early as teenage years. Even though there are no current established guidelines on primary prevention of ASCVD in adolescents and children age <19 with risk factors such as dyslipidemia, diabetes, and hypertension, early risk-focused screening with lifestyle and medical management is a window of opportunity to slow down ASCVD. Intensive lifestyle management for 3 to 6 months before considering statin therapy if LDL remains >130 mg/dL is current recommendation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.