
Abstract
Hypokalemia is a common condition that has been well studied. In most patients, mild hypokalemia is asymptomatic, while those with moderate-to-severe hypokalemia tend to show more prominent symptoms. In patients with a potassium level of 2.5 milliequivalents/liter (mEq/L) or lower, symptoms such as muscle cramps or weakness, rhabdomyolysis, and myoglobinuria tend to arise. These manifestations can lead to more debilitating consequences, such as renal failure secondary to rhabdomyolysis or respiratory failure secondary to muscle weakness. Other symptoms such as ileus, nausea, and vomiting, as well as cardiac arrhythmia and abnormalities, are also associated. Here we would like to present a patient with a potassium level of 1.4 mEq/L secondary to furosemide who presents to the emergency department with only complaints of muscle spasms for the past few days.
Introduction
Throughout medicine, there have been many different causes that can be attributed to hypokalemia, whether they are genetic, pathological, physiological, or medication-induced. However, despite all these medications, diuretic usage has been a very common cause, and one of the most commonly associated diuretics is furosemide. In fact, prior studies have reported severe hypokalemia in patients with chronic furosemide use.1,2 When also considering the fact that this medication is widely used throughout the United States for patients with volume overload and heart failure, it is understandable why it can be chronically misused in an outpatient setting. 3 In most inpatient settings, the side effects are addressed by providers more accordingly, since potassium wasting is a fairly common side effect of loop diuretics. However, in outpatient settings, miscommunication can occur, and patients can often take too much or too little of their medication. 4 As such, proper education regarding medications adherence should always be made clear to the patient to prevent misuse. This is particularly true since hypokalemia due to furosemide, although may be a common side effect of loop diuretics, can also result in a large electrolyte deficit if it is not taken as prescribed. In this case, we would like to present a patient who arrived at the emergency department with complaints of muscle cramps and weakness. Blood work revealed that the patient had a potassium level of 1.4 mEq/L, and a prior chart review revealed that he had a similar hypokalemia episode of 2.1 mEq/L in a different hospital. This case attempts to not only highlight the management of hypokalemia but also stress the importance of patient education and proper medicine adherence.
Case Presentation
The patient is a 62-year-old male with a history of inguinal hernia, hypothyroidism, and hypertension who presents with bilateral upper and lower extremity weakness and muscle spasms for 2 days. The patient noted that he never had a history of diabetes or asthma. He also denies any history of trauma, strenuous exercise, or any insult that could lead to his extremity weakness and spasms. On chart review, the patient was admitted to another hospital approximately 7 months prior for his inguinal hernia and was noted to have a potassium level of 2.1 millimoles/liter (mmol/L) and a magnesium level of 1.7 milligrams/deciliter (mg/dL) which was replenished accordingly, with a potassium of 3.4 mmol/L at discharge. He stated that he had not had any episodes of hypokalemia prior, except when he was hospitalized 7 months ago. The patient stated that during that time he was taking 20 mg of furosemide for hypertension and had no symptoms of hypokalemia and noted that the hypokalemia was an incidental finding at that time. He was then prescribed 30 pills of 20 milliequivalents (meq) of potassium chloride with a few refills, along with 30 pills of 20 milligrams (mg) of furosemide with 5 refills at discharge from his prior outside hospitalization. However, in our emergency department, the patient states that he currently takes furosemide 20 mg and enalapril 20 mg oral daily for hypertension and levothyroxine 25 micrograms (mcg) for hypothyroidism and no other medications. The patient did not go into further details as to why he did not take his other prescribed medications and simply shrugged his shoulders. He notes that he does not take his medication as prescribed because he sometimes forgets and takes much more to compensate, believing that there was no harm to taking more blood pressure medication. Family and social history was unremarkable, and he denied consumption of any black licorice.
On the physical exam, the patient’s vitals were unremarkable, with a temperature of 36.4°C, heart rate of 87 beats per minute, respiratory rate of 20 breaths per minute, blood pressure of 107/65 mm Hg, and a SpO2 of 100%. Decreased range of motion was appreciated in the bilateral upper and lower extremities, secondary to weakness and mild pain. Trace edema was noted in the bilateral lower extremities however, the rest of the physical exam was unremarkable.
Blood work showed the patient to have a potassium level of 1.4 mmol/L and a magnesium level of 1.6 mg/dL. The phosphorus level was also noted to be low at 1.3 mg/dL, but all other electrolytes were unremarkable. Thyroid function tests were unremarkable, resulting in any thyroid related causes of the patient’s hypokalemia being unlikely. Patient creatine kinase (CK) was also noted to be elevated at 2537 units/L. Aldosterone was noted to be low, ruling out hyperaldosteronism induced hypokalemia (Table 1). Urine electrolytes were done on initial presentation and approximately 32 hours after and showed no significant changes. Urine toxicology screen was also unremarkable (Table 1). Initial electrocardiogram (EKG) showed only premature ventricular contraction (PVC) and a prolonged corrected QT but otherwise no significant abnormalities (Figure 1a), and a prior chart review of the patient’s last hospitalization revealed a CT scan that detailed the patient’s inguinal hernia but no adrenal masses or enlargement.
Laboratory Findings.

Hours noted, are hours after initial presentation and the units are the same as the reference noted. References that are noted N/A are equivalent to not available.
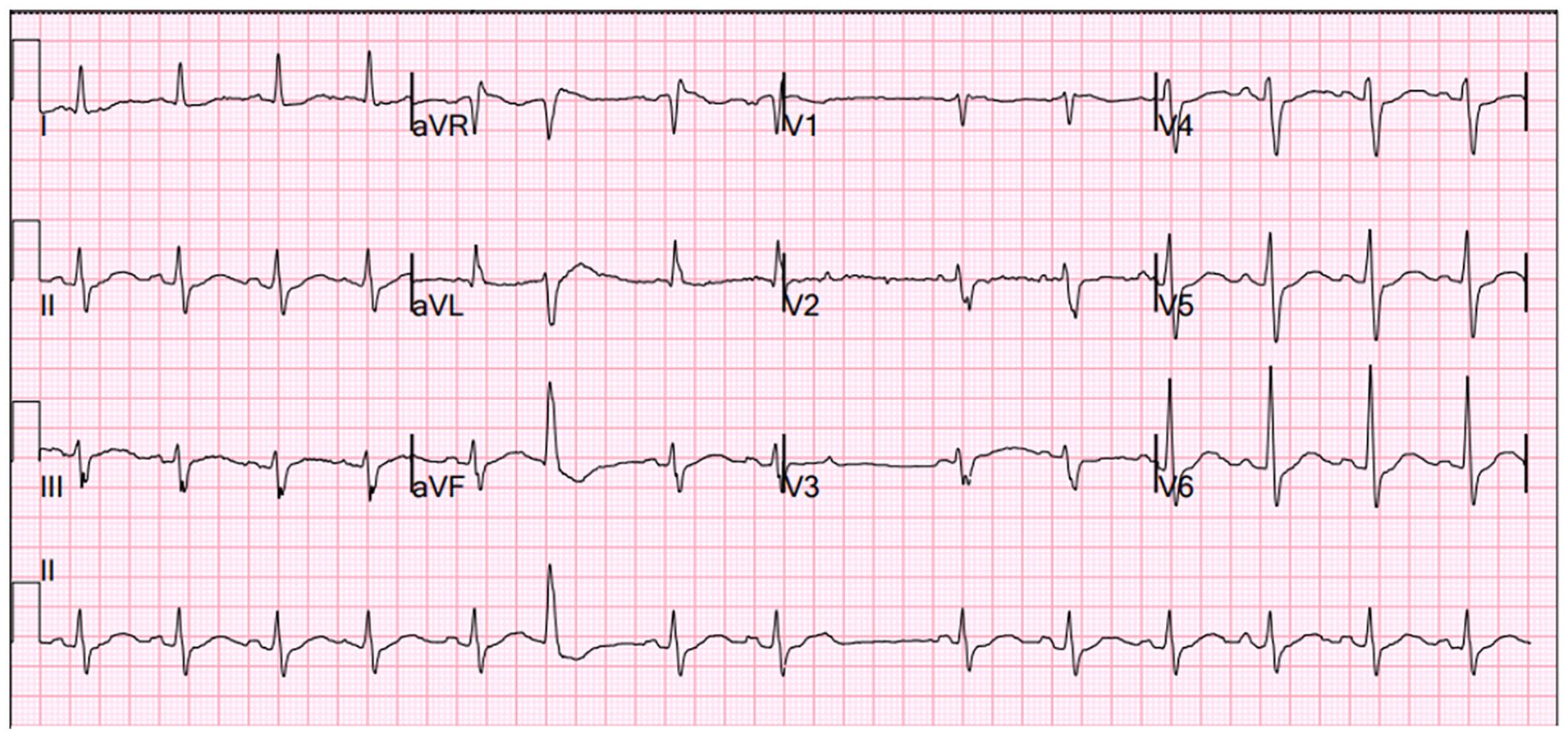
EKG at initial presentation.
The patient was then started on cardiac monitoring with electrolyte replenished and a basic metabolic panel (BMP) every 4 hours. He was given 40 mEq of intravenous (IV) potassium chloride, along with 40 mEq of tablet extended release and 40 mEq of liquid potassium solution, for the first 4 hours after the initial presentation. Another 120 mEq was given from the fourth hour to the eighth hour, and the patient was noted to have a slight rise in potassium. The patient did have some mild chest pain, and a repeat EKG was done, which showed a shorter corrected QT compared with prior and was otherwise unremarkable (Figure 1b). He was then given 80 mEq of potassium chloride via IV, tablet, or liquid, due to patient preferences, every 4 hours, and eventually 40 mEq every 4 hours. Overall, the patient had received approximately 840 mEq of potassium replenished over the course of approximately 60 hours. Other electrolytes were also replenished accordingly. The patient then noted significant improvement in his muscle spasms and aches; however, he urgently had to return home to address family issues and no longer wanted potassium supplementation due to the resolution of his symptoms. As such, final BMP’s to ensure the patient’s potassium had normalized were unable to be obtained; however, the patient was properly educated on medication side effects and proper adherence right before the patient left. He was also asked to repeat the reason why he was prescribed the medications he was prescribed, as well as the dosage and side effects, to ensure understanding. The patient was also provided with printouts of his medications as well as side effects, and given printouts on the importance of adherence and how a repeat situation could occur if he failed adherence once more. He was then prescribed 20 mEq of potassium chloride along with 20 mg of furosemide with a follow-up appointment. Unfortunately, since the patient was not from our local area, he stated that he would most likely not follow-up, and as such, he was lost to follow-up.

EKG after approximately 24 hours after initial presentation.
Discussion
Furosemide is a very common loop diuretic with a lot of applications, but is particularly used as the first line in heart failure and fluid-overloaded patients. However, other effects that these classes of medications have included their ability to lower blood pressure. In fact, some studies have noted loop diuretics as having potential advantages, preferably fewer side effects, over thiazide diuretics. 5 Due to this, side effects can tend to be overlooked.
When the patient presented to our emergency department, an initial diagnosis stemmed from 3 particular concepts that could have resulted in the patient’s hypokalemia. These included increased potassium entry into cells, gastrointestinal loss, and finally, urinary loss. In regard to increased potassium entry into cells, the patient denied any history of asthma or diabetes. Therefore, he never used any medications that would drive potassium into cells, such as insulin or albuterol. This was further proven when the patients prescribed outpatient medications were assessed. He also denied any history of nausea, vomiting, or any constipation that would require laxative use; however, even though laxative use was not specifically asked for, he denied taking any other medications. Thus, gastrointestinal causes of potassium wasting were deemed highly unlikely. Consequently, it was inferred that the patient’s primary cause of potassium wasting was urinary loss.
When the patient was asked about the medications he was taking, he had 3 bottles of medications which were furosemide 20 mg, enalapril 20 mg, and levothyroxine 25 mcg. Despite the patient taking such a low dose of furosemide, the patient developing furosemide-induced hypokalemia was unlikely but not impossible. As such, other differential diagnoses included primary mineralocorticoid excess due to an adrenal adenoma, mineralcorticoid excess, or genetic disorders such as Bartter or Gitelman syndrome, which had to be ruled out before concluding that this was furosemide induced. Initially, the diagnosis of primary mineralocorticoid excess due to primary hyperaldosteronism was considered due to the patient’s history of hypertension, hypokalemia, and low renin. However, this was deemed unlikely due to the patient’s low aldosterone blood levels (Table 1). The patient also denied consumption of any black licorice that could result in any apparent mineralocorticoid excess. The patient did have low renin and low aldosterone along with a history of hypertension and muscle weakness which could be due to Cushing syndrome, leading to hypokalemia via the mineralocorticoid effect that cortisol has. However, the patient denied any weight gain, hirsutism, mood changes, or any other symptoms indicative of Cushing syndrome. The physical exam also did not reveal any buffalo hump, signs of bruising, abdominal striae or any other physical exam findings besides muscle weakness. Blood glucose was also noted to be unremarkable throughout the entire admission. As such, the suspicion of Cushing syndrome causing the patient’s hypokalemia was low, and therefore, a cortisol level was not tested. Finally, the fact that the patient had a history of hypertension rather than hypotension argues against potassium wasting genetic diseases such as Bartter or Gitelman syndrome. The patient also denied any family history of genetic disorders and had also noted no past medical history of genetic diseases or being hypokalemic prior, except his prior hospitalization, made the diagnosis of a 62-year-old male with a newly diagnosed Bartter or Gitelman syndrome highly improbable.
Based on prior chart review, it was concluded that our patient most likely had medication induced hypokalemia secondary to furosemide. A counterpoint would be that the patient was also noted to have a low urine potassium, which would argue against furosemide induced hypokalemia. However, the reason for this was most likely due to the fact that the patient’s recent dose of furosemide had worn off. This, as a result, would cause the patient’s body to retain as much potassium as possible. This hypothesis is further supported by the fact that the patient also has low urine sodium and chloride, which would be expected to be high if furosemide was in effect. Unfortunately, the patient was unable to confirm this since he had difficulty recalling when he took his last furosemide dose.
Due to the presentation, history, blood work, and prior imaging, it was safe to conclude that our patient developed hypokalemia secondary to furosemide, which not only resulted in serum hypokalemia but also a severe state of low total body potassium stores. This concept was key in terms of treatment, mainly because the replenishment of potassium in smaller doses can lead to a rapid hyperkalemic episode if the patient’s body has proper potassium stores. In fact, prior studies have noted that patients who were hypokalemic (2 mEq/L) became rapidly hyperkalemic (>5.5 mEq/L) with a rate of 10 mEq of potassium per hour over 8 hours, with EKG changes. 6 Due to our suspicion that the patient’s hypokalemia was due to intermittent high uses of furosemide over a long period of time, the likelihood that the patient had a lack of potassium stores was high; however, the possibility that the patient did not have low body potassium stores and simply had hypokalemia remained. Thus, a more moderate to high dosage of potassium replenishment of 30 mEq per hour was the initial replenishment rate of choice, with a constant monitor of the patient’s potassium levels every 4 hours.7,8 Initially, a rate of 40 mEq per hour was considered since 1 cohort study concluded that potassium infusions of 20 to 40 mmol replenishment per hour were safe to administer in critically ill patients. 9 However, since there was a concern about whether or not the patient had a potassium deficit, as well as the fact that he only had mild symptoms with no severe EKG changes, it was decided to start the patient on a relatively moderate to high replenishment rate. In short, the patient was noted to have a potassium deficit requiring 840 mEq of potassium. Persistent telemetry and monitoring should also be crucial to ensuring arrhythmias are addressed.10-12 Other clinical signs and symptoms such as muscle spasms and weakness should also be taken into account. Fortunately, the patient was able to respond to the replenishment rate, and after persistent monitoring of the patient’s potassium, there was eventual normalization with an improvement in symptoms.
Conclusion
Overall potassium replenishment can vary based on clinical symptoms, with a maximum replenishment rate of 40 mEq of potassium chloride IV per hour; however, patients that require such a high rate are usually those in need of life-saving measures.8,9,13 As such, more moderate replenishment rates, such as 20 to 30 mEq of potassium chloride per hour, should be considered. One important point is that patients can also present with low urine potassium along with other low urine electrolytes if the loop diuretic effect has worn off by the time the urine electrolytes were sent. The reason being is that after the furosemide effects have abated, the kidneys would respond by retaining as much electrolytes as possible. As such, it should be key to ask the patient when their last dose of diuretic was taken to correlate it with the patient’s urine electrolytes accordingly. Another key point that should be addressed is the importance of patient education and physician communication. This patient history had shown that this was the second time that the patient developed severe furosemide-induced hypokalemia due to not properly adhering to the medication once a day. Per the patient, there were multiple times when he had taken it more than once a day due to occasional forgetfulness about whether he took the medication. This is where having patients more involved with their health care and encouraging health literacy can improve medication adherence. 14 In fact, many studies have highlighted the multifactorial nature of why patients are not adhering to their medications.4,14,15 As physicians, patient education regarding why they are prescribed these medications and their side effects can not only increase medical literacy but possibly also increase medicine adherence. This in and of itself does not only pertain to furosemide but to medications as a whole. Hopefully, this case helps provide a crucial component in patient education, the dangers of medical side effects of commonly prescribed medications, and the importance of physician communication and providing health literacy to all our patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval to report this case was obtained from the Kern Medical Institutional Review Board; approval ID: 24038.
Informed Consent
Written informed consent was obtained from the patient for their anonymized information and photography to be published in this article.