
Abstract
Primary gastric Burkitt’s lymphoma is an aggressive non-Hodgkin’s lymphoma that has been rarely reported in the literature. The majority of primary gastric lymphomas are diffuse large B-cell lymphomas and mucosa-associated lymphoid tissue (MALT) lymphomas. Patients with primary gastric Burkitt’s lymphoma can present with abdominal pain, hematemesis, melena, perforation, and obstruction. Diagnosis is made with a combination of clinical, radiological, and pathological findings. Treatment data are limited due to the limited cases reported. We present a case of a 47-year-old female who presented with diffuse abdominal pain, melena, and coffee-ground emesis that was diagnosed with primary gastric Burkitt’s lymphoma following biopsies taken from a gastric ulcerated mass found on upper endoscopy.
Introduction
The vast majority of primary gastric lymphomas are diffuse large B-cell lymphomas and mucosa-associated lymphoid tissue (MALT) lymphomas. 1 Primary gastric Burkitt’s lymphoma is an extraordinarily rare primary malignancy with very few cases reported in the literature. 2 Approximately 50 cases have been reported of primary gastric Burkitt’s lymphoma. 2 Burkitt’s lymphoma can be classified as endemic, sporadic, or immunodeficiency-associated. 3 We present the case of a 47-year-old-female presenting with abdominal pain, melena, and coffee-ground emesis who was found to have an ulcerated gastric mass and subsequently diagnosed with primary gastric Burkitt’s lymphoma.
Case Presentation
A Caucasian 47-year-old female with a history of endometriosis, anxiety, and depression presented to the emergency department with a 3-month history of progressively worsening abdominal pain associated with 1 episode of melena and coffee-ground emesis on the day of presentation. The pain was located in the epigastric region, cramping in nature, non-radiating, alleviated by slow breathing and worsened with stress. She also reported intermittent melena for a few months and 1 episode of coffee-ground emesis on the day of presentation. She endorsed daily ibuprofen use for about 20 years due to endometriosis pain. She also had a 15-pound weight loss and decreased appetite for a few weeks. She denied diarrhea, fevers, chills, and night sweats. The patient endorsed smoking half a pack of cigarettes for 33 years. Of note, she received a computed tomography (CT) abdomen and pelvis with contrast 3 months prior to her emergency department (ED) presentation for her abdominal pain, which revealed stomach wall thickening and prominent gastrocolic ligament lymph nodes. She was diagnosed with a gastric ulcer, based on clinical and imaging findings and was treated with proton pump inhibitor. She was recommended to follow up for an endoscopy, but she did not have the procedure.
On examination, temperature was 99.3°F, blood pressure 146/98 mm Hg, pulse 92 bpm, respiratory rate 18, and oxygen saturation 100% on room air; the remainder of the exam demonstrated normoactive bowel sounds and epigastric tenderness without rebound tenderness or guarding. Laboratory studies were significant for white blood cell count (WBC): 16.5 10 × 3/µL, Hgb: 10 g/dL, mean corpuscular volume (MCV): 74.4 fL, platelet (Plt): 635 10 × 3/µL, iron: 15 µg/dL, total iron-binding capacity (TIBC): 310 µg/dL, iron saturation: 5%, and ferritin: 5.2 ng/mL (Table 1). A computed tomography angiography (CTA) abdomen and pelvis with contrast revealed gastric wall thickening and circumferential wall thickening with aneurysmal dilation of the fourth portion of the duodenum and proximal jejunum with adjacent mesenteric and retroperitoneal adenopathy (Figure 1); the duodenal and jejunal findings were new compared to the abdominal CT 3 months prior. A subsequent upper gastrointestinal (GI) endoscopy revealed a 29-mm oozing cratered gastric ulcerated mass with adherent clot found on the gastric body (Figure 2). Biopsies revealed gastric mucosa infiltrated with a B-cell lymphoma with morphologic and immunophenotypic features that resembled Burkitt’s lymphoma (Figure 3). Immunostaining demonstrated that atypical lymphocytes were positive for Epstein-Barr Virus (EBV), CD20, PAX5, BCL6, CD10, MYC (60%), Ki-67 = greater than 90% and negative for BCL2, and mum 1. Fluorescence in situ hybridization (FISH) found MYC translocation (8q24.1) confirming the diagnosis of Burkitt’s lymphoma. BCL6 and BCL2 were normal on FISH. Helicobacter pylori testing was negative. The patient was started on the R-EPOCH chemotherapy regimen: rituximab, etoposide, prednisone, vincristine, cyclophosphamide, and doxorubicin. The patient continues to receive her chemotherapy at this time.

CTA of the abdomen and pelvis with contrast revealing gastric wall thickening as indicated by the red arrow (A) and circumferential wall thickening with aneurysmal dilation of the fourth portion of the duodenum and proximal jejunum as indicated with the red arrow with adjacent mesenteric and retroperitoneal adenopathy (B).

Esophagogastroduodenoscopy demonstrating a 29-mm oozing, cratered, ulcerated gastric mass with adherent clot.
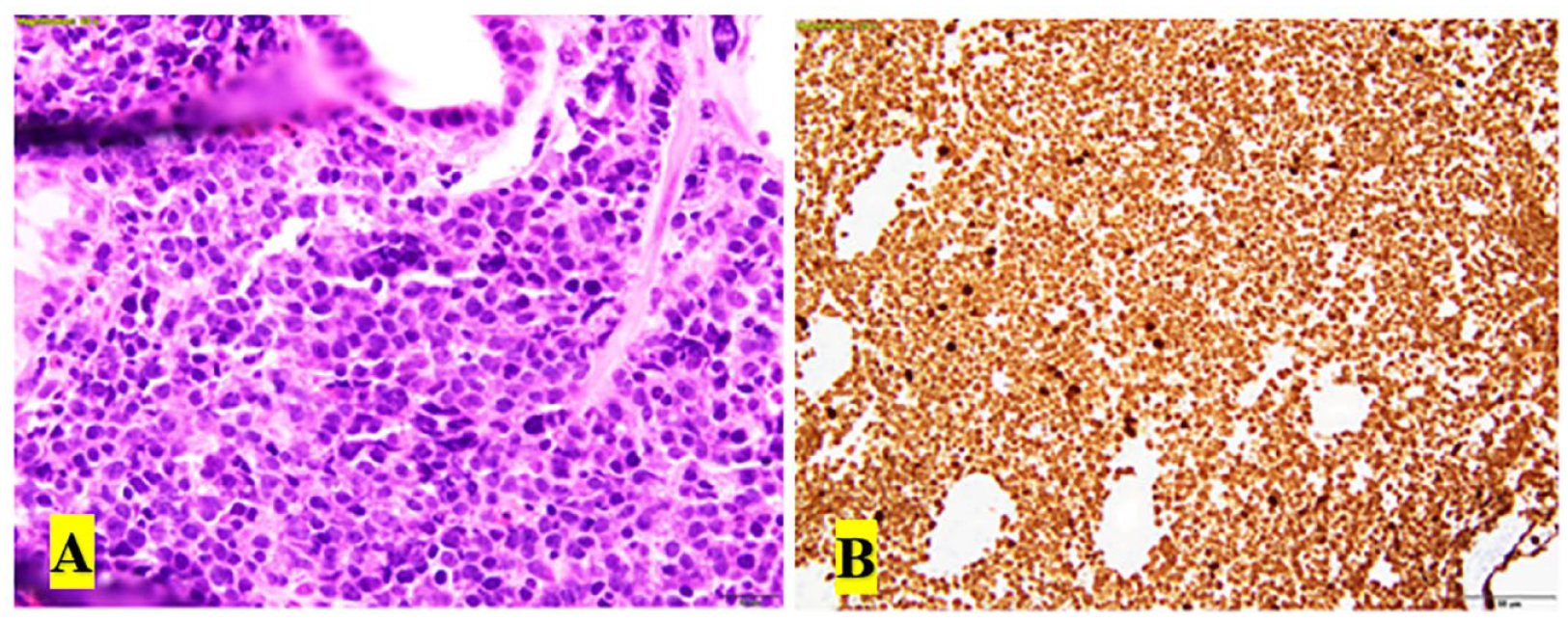
(A) Staining with hematoxylin and eosin revealing gastric mucosa infiltrated with a B-cell lymphoma with morphologic and immunophenotypic features that resemble Burkitt’s lymphoma. (B) Immunohistochemistry stains with atypical lymphocytes that are greater than 90% positive for Ki-67.
Initial Lab Values on Presentation.

Abbreviations: ALT, alanine transaminase; AST, aspartate transaminase; BUN, blood urea nitrogen; WBC, white blood cell.
Discussion
Primary gastric lymphomas are typically divided into 2 histological subtypes: diffuse large B-cell lymphomas and MALT lymphomas.1,4 These 2 subtypes make up approximately 90% of all primary gastric lymphomas. 4 The other most commonly seen primary gastric lymphomas are mantle cell lymphoma (1%), follicular lymphoma (0.5%), and peripheral T-cell lymphoma (1.5%). 4 Secondary GI involvement is common in non-Hodgkin’s lymphoma compared with primary GI involvement. 2 A 2015 report by Chen et al 5 examined 299 patients with primary GI lymphomas and found primary GI Burkitt’s lymphoma in 1.3% of those patients. A 2014 report by Mitra et al 2 found 48 primary gastric Burkitt’s lymphomas and 97 primary intestinal Burkitt’s lymphoma reported in the literature at the time of its publication.
Burkitt’s lymphoma can be classified as endemic, sporadic, and immunodeficiency-associated. 3 Endemic Burkitt’s primarily affects children around the ages of 4 to 7 years, and it has the highest incidence in Africa. 3 It typically affects males twice as often compared with females. 3 Sporadic Burkitt’s occurs globally and can occur at any age. 3 Immunodeficiency-associated Burkitt’s mainly occurs in patients infected with human immunodeficiency virus (HIV). 3 The exact mechanism leading to the formation of Burkitt’s lymphoma is not completely understood. 3 The vast majority of Burkitt’s lymphomas are caused by EBV; 3 our patient’s ulcerated gastric mass biopsy was EBV positive.
The clinical symptoms reported with primary gastric Burkitt’s lymphoma can include abdominal pain, hematemesis, melena, perforation, and obstruction.1,2 Clinical, radiological, and pathological findings aid in the diagnosis of primary gastric Burkitt’s lymphoma. The presence of gastric wall thickening without other GI involvement on initial imaging points toward primary gastric involvement and not primary intestinal involvement. Burkitt’s lymphoma is histologically classified as a starry sky appearance, which is due to scattered macrophages surrounded by proliferating lymphoma cells. 6 A chromosomal translocation between the Myc proto-oncogene and one of 3 immunoglobulin genes is a defining characteristic in Burkitt’s lymphoma. 7 The most common translocation involves the long arm of chromosome 8 at the 8q24 locus. 7 80% of translocations with Burkitt’s lymphoma involve the translocation of the telomeric region of chromosome 8 to the immunoglobulin heavy chain gene on chromosome 14. 7
Burkitt’s lymphoma is an aggressive malignancy and requires immediate intervention.3,8 Treatment data are limited due to few number of cases of primary gastric Burkitt’s lymphoma reported.1,2 Ayoub et al 1 reported a case of primary gastric Burkitt’s lymphoma that was treated with prophylactic intrathecal methotrexate and R-EPOCH chemotherapy. Our patient was similarly started on R-EPOCH chemotherapy and is currently planned to receive 5 scheduled doses. Dose adjusted R-EPOCH is less toxic than other Burkitt’s lymphoma regimens and maintains a high rate of cures amongst a wide variety of Burkitt’s lymphoma patients. 9
Conclusion
Primary gastric Burkitt’s lymphoma is a rare, aggressive malignancy that has been scarcely reported in the medical literature and physicians should consider primary gastric Burkitt’s lymphoma in their differential for patients presenting with abdominal pain, hematemesis, and melena.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Informed consent for patient information to be published in this article was not obtained because the patient and next of kin were both non-responsive when contacted for consent despite multiple attempts. All of the patient’s information was de-identified.
Prior Presentation of Abstract Statement
The case was not presented anywhere else.