
Abstract
Bilothorax, an exudative pleural effusion due to the accumulation of bile. It is also called cholethorax or thoracobilia and was initially reported in 1971. Here, we report a rare case of an elderly male presenting with bilateral bilothorax due to esophageal rupture. A 78-year-old man with multiple medical ailments presented to the emergency room (ER) with a severe episode of vomiting accompanied by a popping sound, respiratory distress, and right sided chest pain. The patient had tachycardia, BP of 101/89 mm Hg, and tachypnea. Computed tomography scan of the chest and abdomen revealed air adjacent to the esophagus, suggesting perforation, atelectasis of right lung, and bilateral pleural effusion (R > L). However, an esophagram did not reveal any perforation. Right-sided chest tube drained dark green bilious fluid. The day after admission, he experienced hemodynamic compromise and hypoxemia requiring intubation, along with fluids and inotropes support. Diagnosis of bilateral bilothorax complicated by hypoxemic respiratory failure with septic shock was made. Cultures were drawn, and empiric antibiotics were started. Nuclear hepatobiliary scan (HIDA) was performed to rule out a hepatobiliary fistula. Results showed reflux activity in the stomach, and distal esophageal leak was identified. Gastrojejunal stenting was performed. However, after prolonged intubation, the family decided on terminal extubation, and he died while receiving hospice care. This case highlights the rarity of bilateral bilothorax, where the HIDA scan played a crucial role in identifying an esophageal leak as the underlying cause, despite normal esophagram results. This condition necessitates prompt diagnosis and aggressive therapeutic interventions.
Introduction
Bilothorax is a rare cause of exudative pleural effusion due to the accumulation of bile and is also called cholethorax or thoracobilia. 1 The first reported case of bilothorax was in a young man who developed right-sided bilothorax following blunt trauma in 1971. 2 Most cases of bilothorax are located on the right side while bilateral presentation is extremely rare. 3 Bilothorax is usually seen in congenital causes, after a recent gastrointestinal or hepatic procedure,2,4 or after traumatic diaphragmatic ruptures. 5 Esophageal perforation causing massive pleural effusion and sudden onset of sepsis is also uncommon. 6
In this case report, we present a rare case of an elderly individual with bilateral bilothorax resulting from esophageal rupture.
Presentation
A 78-year-old male with multiple ailments of hypertension, atrial fibrillation, and rheumatoid arthritis presented to the emergency department after experiencing an episode of emesis with discomfort in his back, and right-sided chest pain for the last 2 hours. The patient described hearing a popping sensation during the retching episode. The patient was normothermic, tachycardic (131 beats/minute), had a blood pressure (BP) of 101/89 mm Hg, and a respiratory rate of 19/min. Arterial blood gas (ABG) of the patient showed pH 7.36/ pCO2 43.5/ paO2 70/ HCO3 25 on 100% O2. Chest X-ray revealed asymmetric perihilar air space (R > L). Considering esophageal perforation as the cause, an esophagram with water-soluble contrast was ordered but showed no evidence of the same. A computed tomography (CT) scan of the chest (shown in Figures 1 and 2) with oral contrast revealed air adjacent to the esophagus suggesting perforation, right lung consolidation consistent with atelectasis, and bilateral pleural effusion (R > L).
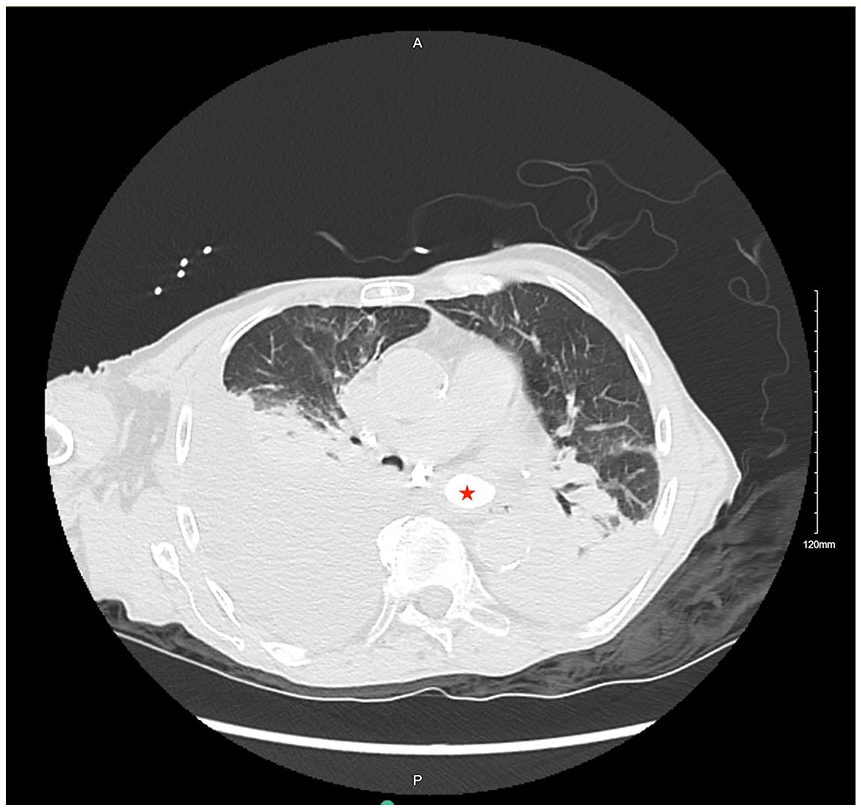
CT scan showing air adjacent to the esophagus suggesting perforation, right lung consolidation consistent with atelectasis and bilateral pleural effusion.
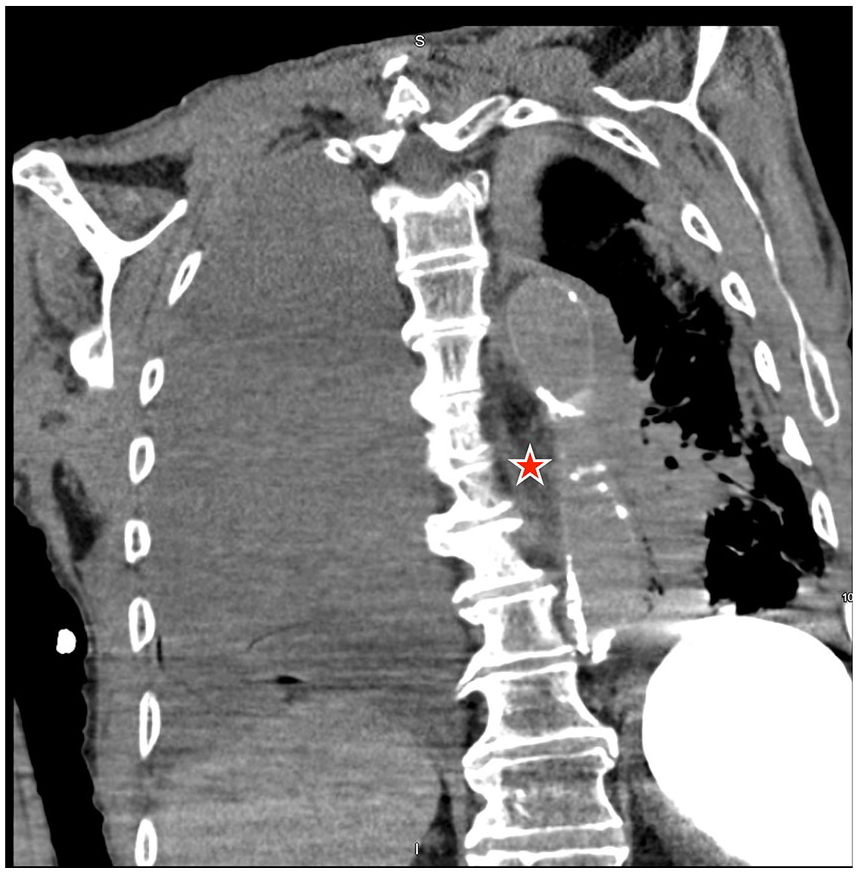
CT scan showing air adjacent to the esophagus suggesting perforation, atelectasis, and bilateral pleural effusion.
Following this, a right-sided chest tube was inserted, and 1 liter of dark green bilious fluid was drained. On the next day, the patient experienced worsening dyspnea but remained cognitively intact with hemodynamic compromise (BP of 96/63 mm Hg, respiratory rate of 21/min, and pulse of 101/min). The patient was intubated with pressure-related volume control (PRVC) mode. The hemodynamic status remained unchanged after administering 1.5 L of crystalloid fluids, and norepinephrine drip was initiated for support. Diagnosis of hypoxemic respiratory failure and septic shock was made. Blood cultures were drawn and empiric therapy of cefepime and vancomycin was started. Considering the bilious appearance of pleural fluid, a nuclear hepatobiliary scan (HIDA scan) was ordered to investigate the presence of hepatobiliary fistula. However, HIDA revealed a reflux activity in the stomach from a distal leak at the gastroesophageal junction. Following this, stenting was done using esophagoduodenoscopy. Despite, appropriate interventions and prolonged intubation, the patient’s condition did not show any improvement. The family decided on the terminal extubation, and the patient died while receiving hospice care.
Discussion
In this rare case, bilious pleural effusion occurred due to the reflux of bilious content through the rupture in the distal esophagus. The sudden increase in intraesophageal pressure and negative intrathoracic pressure which occurs during severe retching resulted in esophageal rupture. 7 The perforation resulted in mediastinitis, pleural collections, and sepsis.8,9 In some cases following rupture, fistulas can be identified using CT scan a few days after the tract has matured, between the abdominal and chest cavities. Buecker et al 10 demonstrated that esophagography performed with a contrast medium can detect a perforation. In this case, the esophagram could not detect the defect as the Gastrografin swallow has a high false-negative detection rate (70%). This discrepancy might be related to the timing of examination, technique, or the inferior radiographic detail provided by the water-soluble contrast medium.11,12 The use of barium sulfate contrast is considered to result in higher sensitivity when compared to those using water-soluble agents such as Gastrografin/diatrizoate. 12 In addition, a nuclear hepatobiliary scan (HIDA scan) can be used to visualize anatomical defects. 13 In our patient, the HIDA scan revealed a leak in the distal esophagus, which was not picked up by the esophagram.
The need for timely intervention is due to the association between bilothorax and the development of empyema. Oparah’s study on thoracobiliary fistulization showed a high incidence of bilious empyema. Gastrointestinal tract organisms like Escherichia coli, Enterobacter, Klebsiella, Enterococcus faecalis, and Staphylococcus aureus were the most common causes necessitating broad-spectrum antibiotics. 14 More than half of the bilious pleural effusions are infected and require immediate drainage of pleural effusion along with early administration of antibiotics to prevent empyema and fibropurulent effusions. 15 Aggressive management is justified, as the thick bilious fluid urgently needs an intercostal tube drain. In addition, as soon as the patient is diagnosed, early positive pressure ventilation should be taken into consideration since contaminated bile in the pleural space may rapidly result in acute respiratory distress syndrome.
Conclusion
This case highlights the rarity of bilateral bilothorax, where the HIDA scan played a crucial role in identifying an esophageal leak as the underlying cause, despite normal esophagram results. This condition necessitates prompt diagnosis and aggressive therapeutic interventions in preventing complications such as respiratory failure, sepsis, or empyema.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethic Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this article.