
Abstract
A 57-year-old woman was diagnosed with adrenocortical carcinoma. Following the adrenalectomy, she underwent adjuvant radiation and mitotane therapy; however, liver metastases were observed. Repeated radiofrequency ablation (RFA) was performed for liver metastases. In addition, a multidisciplinary approach combining systemic chemotherapy, radiotherapy, and surgery was used for lung and distant lymph node metastases that arose during the course of treatment. Notably, 49 months have passed since the adrenalectomy and 36 months since the recurrence of the liver metastases, and the patient remains on multidisciplinary therapy. Thus, RFA for liver metastasis of adrenocortical carcinoma may be an effective component of a multidisciplinary treatment.
Keywords
Introduction
Adrenocortical carcinoma (ACC) is a rare malignancy, with a prevalence of 0.72 million cases per year. 1 Although the only curative treatment is complete surgical resection, its availability is limited because most patients are diagnosed at advanced stages of the disease. 2 The frequency of metastasis to other organs at diagnosis is 60% to 70%, 3 and the 5-year survival rate of ACC cases with metastasis to other organs is 0% to 17%. 4 Moreover, ACC is associated with high recurrence rates, despite complete resection of the primary tumor. 5 The treatment options for metastatic ACC are limited. Complete resection of metastases is recommended in some cases; however, complete resection is difficult in many cases because the metastatic lesions are often multiple or large, and systemic chemotherapy is recommended. 6 Nonetheless, options for systemic chemotherapy are limited. A regimen combining etoposide, doxorubicin, and cisplatin (EDP) with mitotane is commonly used; however, progression-free survival was 5.3 months and overall survival was 14.8 months, which were unsatisfactory results.7,8 Therefore, it is difficult to achieve the long-term prognosis with systemic chemotherapy alone.
Radiofrequency ablation (RFA) is a minimally invasive and highly curative treatment. 9 Although the efficacy of RFA on hepatocellular carcinoma is well established, 10 its curative or cytoreductive effects on metastatic liver tumors have also been reported.11,12
We encountered a case in which aggressive RFA was performed for the recurrence of multiple liver metastases after resection of a primary ACC tumor, and favorable therapeutic effects were obtained. Systemic chemotherapy was effective for the subsequent concurrent lung and distant lymph node metastases. However, controlling liver metastasis is difficult with systemic chemotherapy, and the combination of RFA and systemic chemotherapy effectively prolongs prognosis. Multidisciplinary RFA therapy may be an effective treatment option for liver metastases of ACC.
Case Presentation
A 57-year-old woman presented with muscle weakness, hypertension, and hypokalemia. She had a history of dyslipidemia and osteoporosis. She reported no history of smoking or occasional alcohol consumption. The patient had no relevant family history. Typical features of Cushing’s syndrome, such as a moon face, purple striae, or central obesity, were not observed. The laboratory data for the first visit are presented in Table 1. Hormone studies revealed high plasma aldosterone concentration (PAC, 297 pg/mL) and low plasma renin activity (PRA, 0.4 ng/mL/h). Captopril challenge test revealed an increased aldosterone-to-renin ratio, suggesting primary aldosteronism. Basal adrenocorticotropic hormone levels were <2.0 pg/mL, and cortisol levels were 17.0 μg/dL. The 24-hour urinary-free cortisol excretion rate increased to 102 μg/d. Serum cortisol levels were not suppressed by administration of 1 and 8 mg dexamethasone, which were in concentrations of 15.3 and 17.7 µg/dL. The bedtime serum cortisol level was 17.4 µg/dL, greater than 5.0 µg/dL. All the results met the criteria of Cushing’s syndrome. Dehydroepiandrosterone sulfate concentration was not elevated (9.0 g/dL). Contrast-enhanced computed tomography (CT) revealed an irregular mass measuring 54 mm × 61 mm in the left adrenal gland with heterogeneous contrast enhancement (Figure 1A and B). Based on these findings, she was suspected to have aldosterone- and cortisol-coproducing ACC and underwent left adrenalectomy.
Laboratory Data at the First Visit.
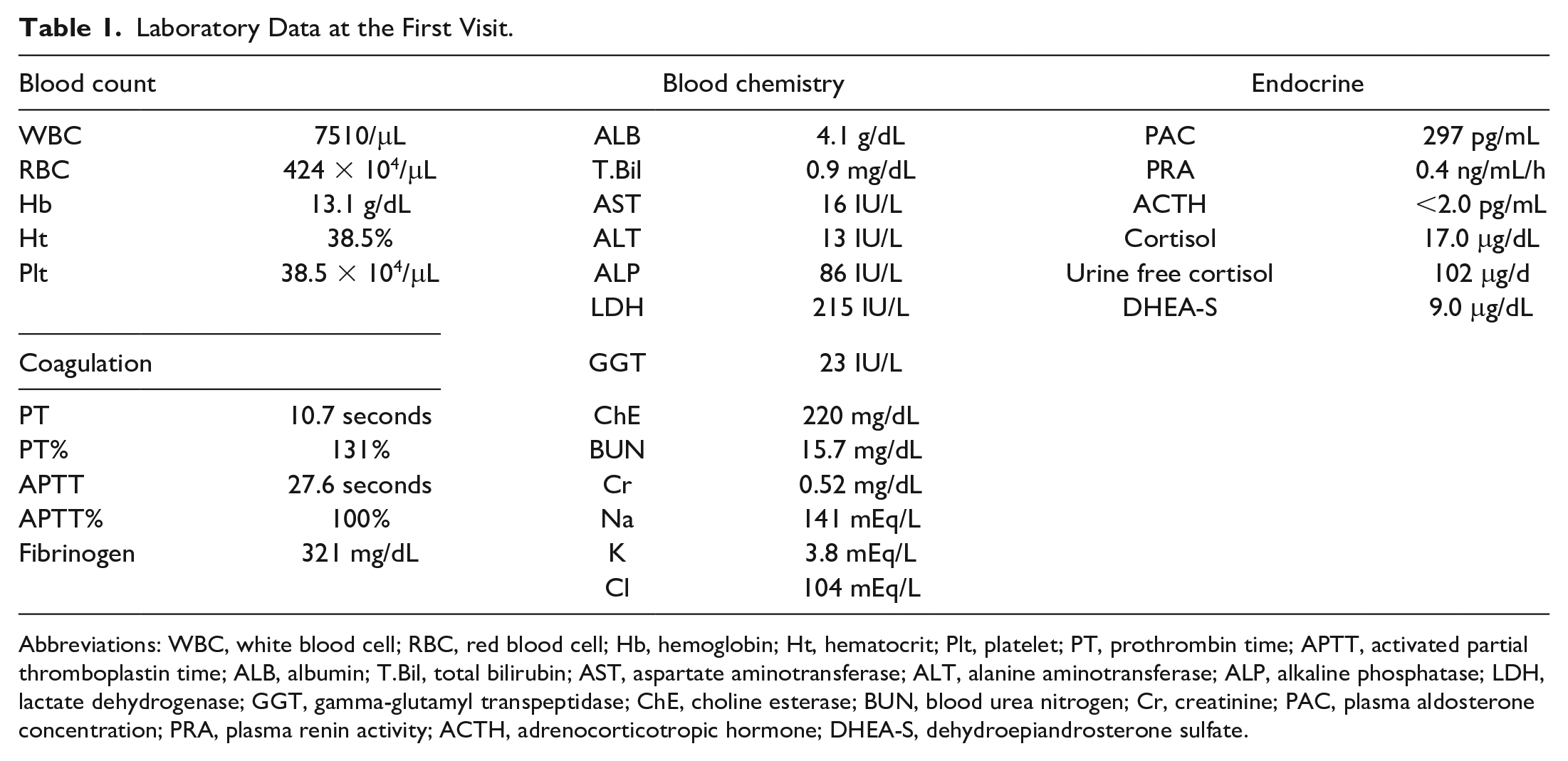
Abbreviations: WBC, white blood cell; RBC, red blood cell; Hb, hemoglobin; Ht, hematocrit; Plt, platelet; PT, prothrombin time; APTT, activated partial thromboplastin time; ALB, albumin; T.Bil, total bilirubin; AST, aspartate aminotransferase; ALT, alanine aminotransferase; ALP, alkaline phosphatase; LDH, lactate dehydrogenase; GGT, gamma-glutamyl transpeptidase; ChE, choline esterase; BUN, blood urea nitrogen; Cr, creatinine; PAC, plasma aldosterone concentration; PRA, plasma renin activity; ACTH, adrenocorticotropic hormone; DHEA-S, dehydroepiandrosterone sulfate.

CT findings at the initial examination and pathological findings at primary tumor resection. Plain CT findings of the ACC at initial examination (A). The lesion (arrow) is a 54 mm × 61 mm heterogeneous mass in the left adrenal gland with heterogeneous enhancement (B). Macroscopic findings reveal a brownish solid tumor with internal hemorrhage and necrosis (C). Microscopic findings revealed alveolar growth of tumor cells, accompanied by high-grade nuclear atypia and multiple mitotic counts. Magnification 100× (D) and 400× (E).
Histological examination met all the Weiss criteria 13 and confirmed the diagnosis of ACC (Figure 1C-E). The European Network for the Study of Adrenal Tumor staging was stage II (T2N0M0) and the Ki-67 index was 13%, suggesting a high risk of recurrence. 6 In addition to hydrocortisone supplementation, she received adjuvant radiotherapy (54 Gy in 30 fractions) and mitotane; however, multiple liver metastases were observed 13 months postoperatively. Systemic chemotherapy was considered; however, metastatic lesions were limited to the liver. Therefore, more curative treatment options were sought. Owing to the large number of liver metastases, complete surgical resection of these tumors is considered difficult and highly invasive. Furthermore, the liver metastases were not highly vascularized, and transarterial chemoembolization (TACE) was considered less effective. Therefore, RFA was selected as the local therapy for liver metastases because it is highly curable and less invasive. The laboratory data at the initial RFA are presented in Table 2. Hepatic and biliary enzyme levels, blood counts, and coagulation test results were normal. However, as the blood concentration of mitotane was as low as 7.8 μg/mL, the mitotane dosage was increased from 3000 to 4500 mg per day. Imaging using plain CT revealed the presence of multiple low-density nodules in the periphery of the liver (Figure 2A and B), and contrast-enhanced CT revealed lesions with a lower density than the surrounding normal liver tissue (Figure 2C and D). Gadolinium ethoxybenzyl diethylenetriamine pentaacetic acid magnetic resonance imaging (Gd-EOB-DTPA MRI) revealed low-intensity lesions in the hepatobiliary phase (Figure 2E and F). While CT revealed 4 lesions, Gd-EOB-DTPA MRI detected 11 metastatic tumors in both liver lobes. Ultrasonography detected only 4 lesions that were identifiable on CT.
Laboratory Data at the Initial RFA.

Abbreviations: RFA, radiofrequency ablation; WBC, white blood cell; RBC, red blood cell; Hb, hemoglobin; Ht, hematocrit; Plt, platelet; PT, prothrombin time; APTT, activated partial thromboplastin time; ALB, albumin; T.Bil, total bilirubin; D.Bil, direct bilirubin; AST, aspartate aminotransferase; ALT, alanine aminotransferase; ALP, alkaline phosphatase; LDH, lactate dehydrogenase; GGT, gamma-glutamyl transpeptidase; ChE, choline esterase; BUN, blood urea nitrogen; Cr, creatinine; CRP, C-reactive protein.

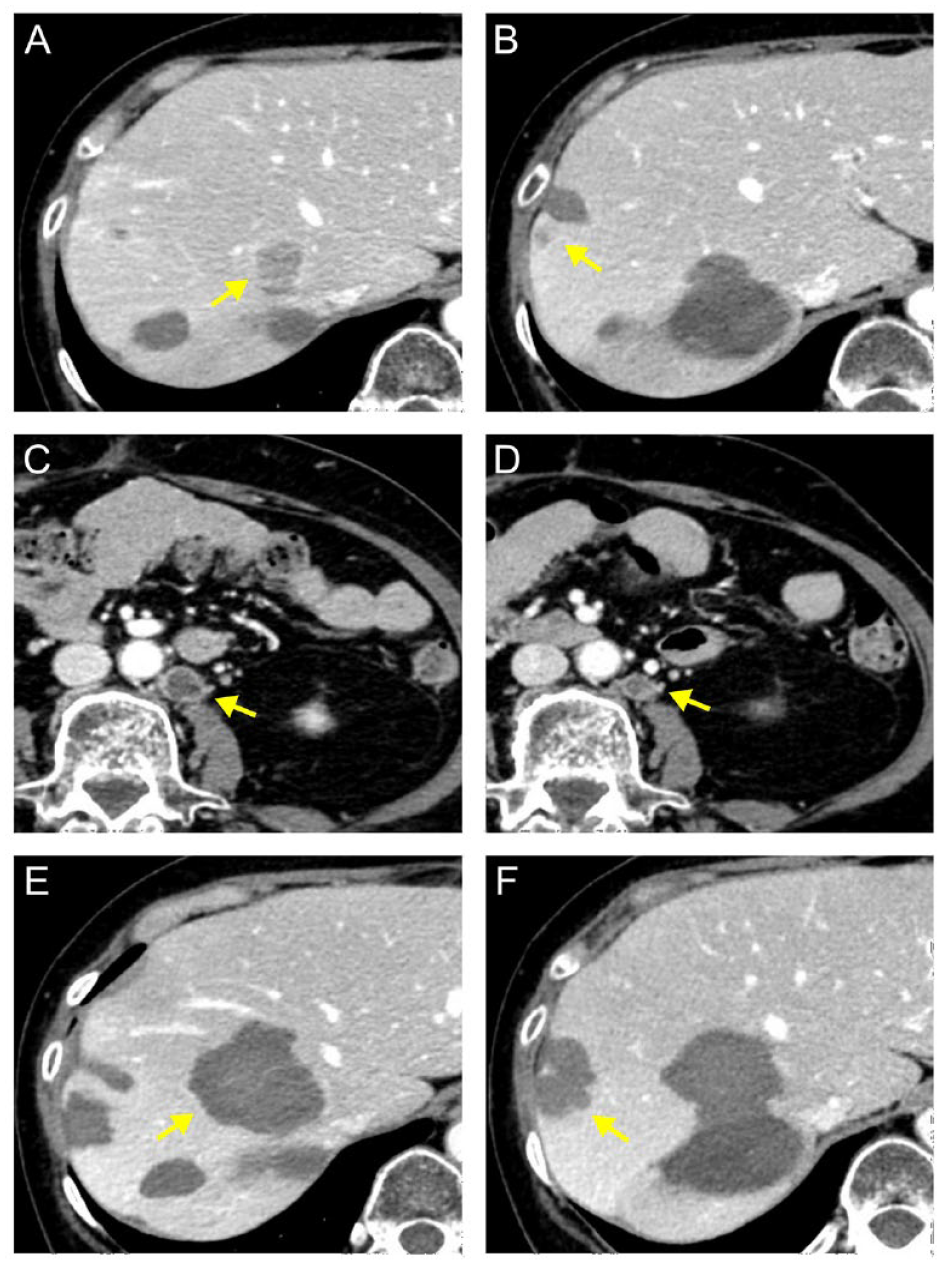
CT and MRI findings of the liver metastases at the initial RFA. Representative CT and Gd-EOB-DTPA MRI findings of liver metastases of ACC at the initial RFA. Plane CT reveals multiple low-density areas (arrows) in the periphery of the liver (A and B). These lesions were of relatively low density compared to the surrounding normal liver with indistinct borders on contrast-enhanced CT (C and D). In addition, a total of 11 lesions (arrows) were observed in the hepatobiliary phase of GdEOB-DTPA MRI (E and F).
Radiofrequency ablation was performed percutaneously under ultrasonographic guidance using an Arfa RF ablation system (Japan Lifeline, Tokyo, Japan). Post-RFA CT revealed a sufficient ablation area without complications. Four months after the initial RFA, lesions that could only be detected on MRI became apparent on CT, and local recurrence was observed near the initial ablation site (Figure 3A and B). At this time, the blood concentration of mitotane was 14.9 μg/mL, which was the optimal concentration. We thought that RFA would be more effective than systemic chemotherapy while the metastatic lesions were limited to the liver, and the patient also wished to continue RFA. Therefore, we decided to continue RFA. A second RFA was performed (Figure 3C and D). Lung metastases appeared 6 months after the initial RFA (Figure 3E and F). Systemic chemotherapy with EDP plus mitotane was initiated. After 4 courses of EDP plus mitotane therapy, the lung metastases were stable, but the liver metastases became apparent and recurred. Radiofrequency ablation was repeatedly performed during the washout period of EDP plus mitotane therapy. During the 28-day cycle of EDP therapy, RFA was performed on day 14. Oral administration of mitotane was continued, even on the day of the RFA. Partial pneumonectomy and radiotherapy were performed as curative treatments for lung metastases 30 months after the initial RFA. Furthermore, the EDP therapy was discontinued because the cumulative dose of doxorubicin was almost maximal. Computed tomography revealed local recurrence of liver metastases and distant lymph node metastases 33 months after the initial RFA (Figure 4A-C). Systemic chemotherapy with a combination of etoposide and cisplatin (EP) was resumed, and distant lymph node metastases showed a partial response (Figure 4D). However, as there was no effect on the liver metastases, the seventh and eighth RFA sessions were performed (Figure 4E and F).

CT findings of the liver metastases at the second and third RFA. Representative CT findings at 4 months (A-D) and 6 months (E and F) after the initial RFA. New metastatic lesions (arrows) are observed in the liver (A and B). The lesions were treated with RFA (C and D). Metastatic lesions (arrows) were observed in the lungs (E, F).
Latest CT findings of liver and distant metastases. Representative CT findings at 33 months (A-C) and 36 months (D-F) after the initial RFA. Recurrence of liver metastases (A and B) and appearance of distant lymph node metastases (C) are observed (arrows). A reduction in the size of the distant lymph node metastasis was observed upon resumption of chemotherapy (D), and RFA was performed for liver metastases (E and F).
Currently, 49 months have passed since the adrenalectomy, 36 months have passed since the initial RFA, and EP therapy continues. Liver metastasis was not observed, and we will continue to monitor distant metastases and consider a ninth RFA when another liver metastasis becomes apparent. In the present case, 8 sessions of RFA were performed on 21 lesions. There were no complications, such as bleeding or infection, and each treatment required hospitalization for several days. Furthermore, the patient’s general condition and liver function did not worsen. The progress from diagnosis to the present is shown in Figure 5.

The progress from diagnosis to the present of the patient.
Discussion
Liver metastasis is strongly associated with prognosis in ACC, and the control of liver metastasis is associated with a prolonged prognosis. 14 A multidisciplinary therapy that combines systemic chemotherapy with local treatment of metastatic lesions is important. 15 Surgical resection alone is often reported to be useful for the treatment of liver metastases.16,17 If complete resection is possible, a long-term prognosis can be expected. Moreover, Datrice et al 16 reported that patients with ACC with recurrence >12 months after adrenalectomy had favorable outcomes. In our case, liver metastasis recurred 13 months after adrenalectomy. However, EOB-MRI revealed 11 metastases in both liver lobes, suggesting that surgical resection was challenging. In addition to surgical resection, RFA and TACE are considered local treatments for liver metastases. Soga et al 18 reported the efficacy of TACE for the treatment of ACC. However, we selected RFA because it is generally more curative than TACE, 19 and the vascularity of the liver metastases was not high in our case.
Radiofrequency ablation is a minimally invasive and curative local treatment for primary hepatocellular carcinoma, and it has also been reported to be effective for various metastatic liver tumors. 20 Most reports on RFA for liver metastases in ACC have examined both surgical resection and RFA, with few reports on RFA alone.21,22 Veltri et al 23 reported that RFA for liver metastasis in ACC was a safe and effective treatment option in the multidisciplinary management. They reported a high local recurrence rate of 66%, and the size of the metastatic liver tumor in the ACC significantly correlated with the local recurrence rate. 23 Bauditz et al 24 also reported a high local recurrence rate after RFA for liver metastases of ACC. They speculated that ACC tends to recur early owing to the heat sink effect due to the high vascularization in the liver metastases of ACC. 24 The fact that high local recurrence rate in lesions with large tumor sizes in our case is consistent with these reports. Metastatic liver tumors should be ablated with a wider safety margin because of stromal infiltration and the lack of a capsule, which makes it difficult for the ablation heat to remain within the tumor. 11 Considering our cases and previous reports, it is crucial to ensure a reliable safety margin to prevent the local recurrence of liver metastasis of ACC. No large clinical trials have compared RFA with surgical resection for liver metastases from ACC. Although there have been cases of long-term survival with surgical resection for liver metastasis in ACC, 16 the recurrence rate is as high as 80%. 21 Radiofrequency ablation has the advantage of being less invasive and is superior to surgical resection in this respect. Currently, surgical resection of metastatic liver lesions is the first treatment option; however, RFA is the next treatment option if surgical resection is difficult due to tumor and patient factors. Future studies are warranted to compare the outcomes of RFA and surgical resection for ACC with liver metastasis.
Surgery, RFA, and systemic chemotherapy alone are insufficient to improve the prognosis of ACC metastases; therefore, multidisciplinary therapy is important. 15 Ou et al 25 reported that RFA should be combined with systemic chemotherapy to achieve effects on microlesions that are undetected by imaging when attempting to treat liver cancer. Reports on the combination of RFA and systemic chemotherapy for ACC are scarce. The EDP therapy is a 4-week course of chemotherapy. We were able to perform RFA safely and efficiently without delaying EDP therapy by using a washout period. This approach enabled the efficient treatment of liver metastases, as well as metastases to other organs. However, the efficacy and safety of the combination of RFA and chemotherapy should be further investigated in a large number of cases.
Lung and distant lymph node metastases also appeared during treatment of liver metastases. Lung metastases were well controlled by surgical resection and radiotherapy after a certain period of chemotherapy. Aggressive local treatments for lung and liver metastases are expected to improve ACC prognosis. 26 Distant lymph node metastases and lung metastases were controlled by systemic chemotherapy, whereas liver metastases clearly increased. The doubling times of primary and metastatic solid tumors are often different. One reason for this is thought to be the acquisition of resistance to the immune system and the induction of new vascularization due to increased tumor volume. 27 Lung and distant lymph node metastases were smaller than liver metastases, which may have contributed to differences in doubling time and response to systemic chemotherapy. Therefore, aggressive RFA for fast-growing liver metastases may improve prognosis.
Our patient showed favorable tumor control with repeated RFA for ACC liver metastases and multidisciplinary therapy, including systemic chemotherapy, resection for lung metastasis, and radiotherapy. As part of a multidisciplinary therapy, RFA for liver metastasis is minimally invasive, may provide sufficient tumor control, and should be considered an effective treatment option for patients with ACC unsuitable for surgical resection.
Conclusion
We encountered a case of ACC with liver metastases, in which aggressive RFA contributed to a favorable tumor control. Radiofrequency ablation for liver metastasis from ACC is minimally invasive and can be performed with little effect on the patient’s general condition, even in combination with systemic chemotherapy. Further investigations with a larger number of cases, including comparisons with surgical resection, are required.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval to report individual cases or a case series.
Informed Consent
Written informed consent was obtained from the patient for the publication of anonymized information in this article.