
Abstract
Aortoesophageal fistula (AEF) is an uncommon, but potentially fatal cause of upper gastrointestinal bleeding. Aortoesophageal fistulas caused by foreign body ingestion are rare but devastating. The classic clinical triad of AEF consists of mid-thoracic pain or dysphagia, a herald episode of hematemesis, followed by fatal exsanguination after a symptom-free period (Chiari’s triad). Computed tomography angiography (CTA) is the preferred diagnostic tool for identifying AEF and is substantially more sensitive than upper endoscopy for detecting AEF. Endoscopy can detect AEF as it might show pulsatile blood, pulsatile mass, hematoma, or adherent blood clot in the esophagus, or a deep esophageal tear. However, endoscopy has a low sensitivity and may delay definitive treatment. Several management options for AEF have been suggested; however, the definitive treatment is surgery performed on the thoracic aorta and esophagus, including esophagectomy, surgical replacement of the thoracic aorta, thoracic endovascular aortic repair, or omental flap. We report a case of a 63-year-old man who presented with hematemesis 2 weeks after chicken bone ingestion.
Introduction
Aortoesophageal fistula (AEF) is a rare but mortal cause of upper gastrointestinal bleeding that arises from various aortic and esophageal diseases including aortic aneurysms, malignancy, postoperative complications, and foreign body ingestion. 1 Massive hemorrhage from the AEF may be preceded by a mild, intermittent herald bleed with a symptom-free period. 2 The interval between sentinel bleeding and subsequent cataclysmic hemorrhage is unpredictable and can occur within hours to days apart.3,4 Treatment should not be delayed once AEF bleeding is suspected, and surgical intervention is the definitive therapy.
We present a case of a patient who had cataclysmic AEF bleeding after chicken bone ingestion.
Case Presentation
A 63-year-old man presented with hematemesis and chest tightness after swallowing a chicken bone 2 weeks prior. He was tachycardic with hemoglobin of 10.2 g/dL on presentation. He had a computed tomography (CT) abdomen and pelvis with contrast that showed severe thickening of the mid-esophagus above the level of the carina with stranding noted within the periesophageal soft tissues. A small extraluminal fluid collection to the left of the esophagus measuring 1 × 1 cm with a tiny focus of increased density extending to involve the adjacent distal aortic arch was also found (Figure 1). These findings were concerning for possible esophageal perforation with extraluminal fluid collection involving the adjacent aortic arch. Cardiothoracic surgery was consulted, and they recommended upper endoscopy (EGD). Emergent Esophagogastroduodenoscopy (EGD) was performed with findings of a deep bleeding mucosal tear about 15 mm in length with possible perforation in the middle third of the esophagus at 25 cm from the incisors (Figure 2). The edges of the esophageal tissue around the tear were approximated, and 3 hemostatic clips were successfully placed. The patient was started on antibiotics and transferred to the intensive care unit (ICU) for close intensive care unit monitoring, and the patient was planned for emergent surgical intervention. Unfortunately, the patient started having several episodes of hematemesis followed by cataclysmic bleeding with multiple cardiac arrest events requiring intubation, and several resuscitation attempts. The patient received several units of red blood cells, fresh frozen plasma, and platelets in an attempt to stabilize him enough for either surgery or interventional radiology, but these measures were futile as he continued to pour out blood from his mouth and nose. The patient eventually expired.
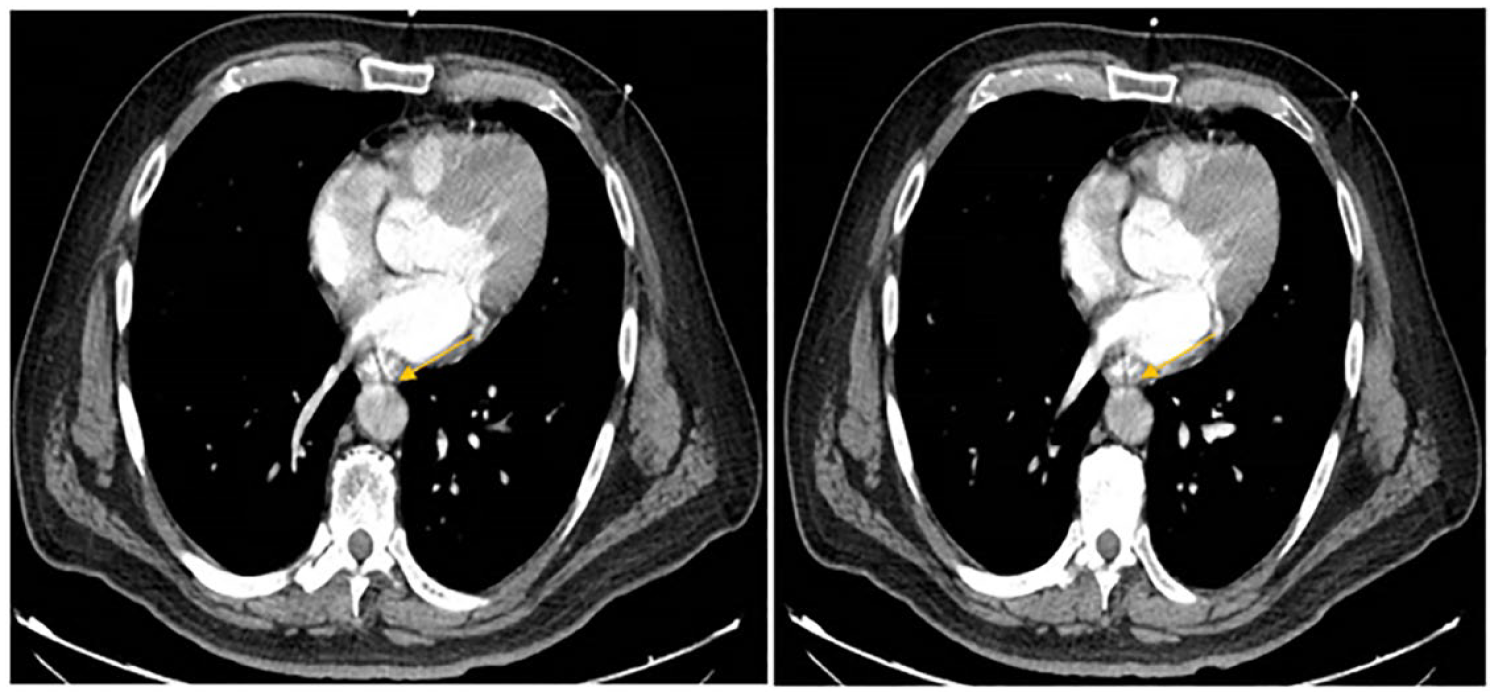
CT abdomen and pelvis with contrast showing communication between esophagus and aorta. Abbreviation: CT, computed tomography.

Endoscopic image showing deep bleeding esophageal tear and endoscopic clips placed.
Discussion
We presented a case of AEF due to chicken bone ingestion that resulted in mortality from massive bleeding.
Aortoesophageal fistula is an uncommon but serious disorder that can lead to massive upper gastrointestinal bleeding with high mortality. 3 Aortoesophageal fistula is more common in males, and its prevalence is unknown; however, some studies suggest an annual incidence of 0.007 per million. 5 Predisposing conditions that may lead to AEF include septic aortitis, mycotic infection, tuberculosis, syphilis, tumor, radiotherapy, foreign bodies, collagen vascular diseases, and postoperative complications of aortic or esophageal disorders. 6 A case review by Hollander and collaborators found 50% of cases of AEF cases were from aortic disease, 20% were from foreign bodies and esophageal malignancy, and less than 5% were due to cases of AEF postaortic or esophageal surgery. 1 Aortoesophageal fistula can present with a herald bleed, and recognition of this bleed is important for quick intervention and to prevent subsequent cataclysmic bleeding where intervention might be too late to stop the bleeding. Herald bleeding often does not result from an actual aortoenteric communication but from focal necrosis and mucosal ulceration.7,8 In AEF, the sentinel bleeding may be minor initially due to the formation of thrombus plugging the fistula as a result of hypotension. However, the plug may be dislodged and extruded out of the canal after the patient becomes normotensive with resuscitation leading to further bleeding and can result in exsanguination. 9 These bleeds appear in approximately 20% to 75% of cases. 7
Suspicion and identification of AEF is crucial to the patient’s survival as timely diagnosis directly influences outcomes. Computed tomography angiography is the favored diagnostic tool for identifying AEF, and studies have shown CTA to be substantially more sensitive at detecting AEF than EGD.10,11 The sensitivity of EGD in diagnosing AEF has been reported to be approximately 50%. 4
Aortoesophageal fistula treatment options have included endoscopic, radiological, and surgical management; however, definitive treatment is surgical intervention. The timing and indication of each type of intervention is still to be determined. Suspected AEF in a hemodynamically unstable patient should proceed immediately to surgery without further diagnostic studies. 11 Endoscopic treatment options to control bleeding have included covered esophageal stents, and 1 study reported the effective use of endoclips to manage AEF.12 -14 Such endoscopic interventions may serve as a bridge but may be done as definitive therapy in patients with advanced age, multiple comorbidities, and poor surgical candidates where endoscopic and radiological embolization may be the best alternatives.15,16 In our case, placement of endoclips did not prevent the massive and lethal bleeding that ensued, reinforcing the need for emergent surgical readiness and intervention in any case of suspected AEF.
Most surgical procedures for the management of AEF include endovascular surgery, esophagectomy, omental wrapping, and graft replacement.17,18 The diagnosis of AEF should be considered in middle-aged and older adults with severe bleeding arising from the esophagus, especially if there is a history of foreign body ingestion. Any patient with a history of foreign body ingestion and imaging findings suspicious for AEF should be considered to have AEF until proven otherwise. Since the time between herald bleed and subsequent massive hemorrhage from AEF is unpredictable, the diagnosis and treatment decision including surgical intervention should be made quickly because of the rapid and mortal course of this condition.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.