
Abstract
Macrophage activation syndrome (MAS) can rarely coexist with lupus pancreatitis. We report on a 20-year-old woman with abdominal pain, nausea, and vomiting. Laboratories were notable for pancytopenia, elevated liver enzymes, elevated ferritin, lipase, and triglycerides. Chest and abdominal computerized tomography (CT) scans revealed bilateral axillary lymphadenopathy, patchy lower lobe consolidations, small pleural effusions, ascites, and splenomegaly. Peritoneal fluid cytology showed lymphocytes and histiocytes with hemophagocytic changes. Immunological workup met the criteria for systemic lupus erythematosus (SLE). Pulse-dosed steroids relieved her condition. Given the high mortality rate associated with MAS, early detection of concomitant pancreatitis and MAS in the context of underlying SLE is critical.
Introduction
Gastrointestinal disorders are prevalent in systemic lupus erythematosus (SLE), affecting approximately 8% to 40% of adult SLE patients. 1 The development of pancreatitis in SLE is multifactorial and complex, involving immune-mediated pancreatic injury and vasculitis. 2 Some patients with lupus-related pancreatitis also experience macrophage activation syndrome (MAS). 3 However, the incidence of MAS in lupus pancreatitis is still not well understood. 4 In this case report, we present a patient with SLE who initially presented with symptoms of pancreatitis and MAS.
Case Presentation
A 20-year-old female initially presented with stabbing epigastric abdominal pain with nausea and vomiting. She also had undocumented episodes of fever and rash over her face and arms over the past few months. On examination, her blood pressure was 85/56 mm Hg, pulse 129 beats per minute, temperature 100.2 F, respiratory rate 22 breaths per minute, and oxygen saturation 95%.
Physical examination was notable for a distended abdomen with diffuse tenderness on palpation. In addition, she had nonscarring patchy hair loss with a hyperpigmented rash covering her cheeks and arms with isolated lesions over her abdomen and enlarged axillary and inguinal lymph nodes. Laboratories (Table 1) were notable for pancytopenia, elevated liver function tests, ferritin, lipase, and triglyceride levels.
Initial Laboratory Results, Immunology, and Serology Workup.
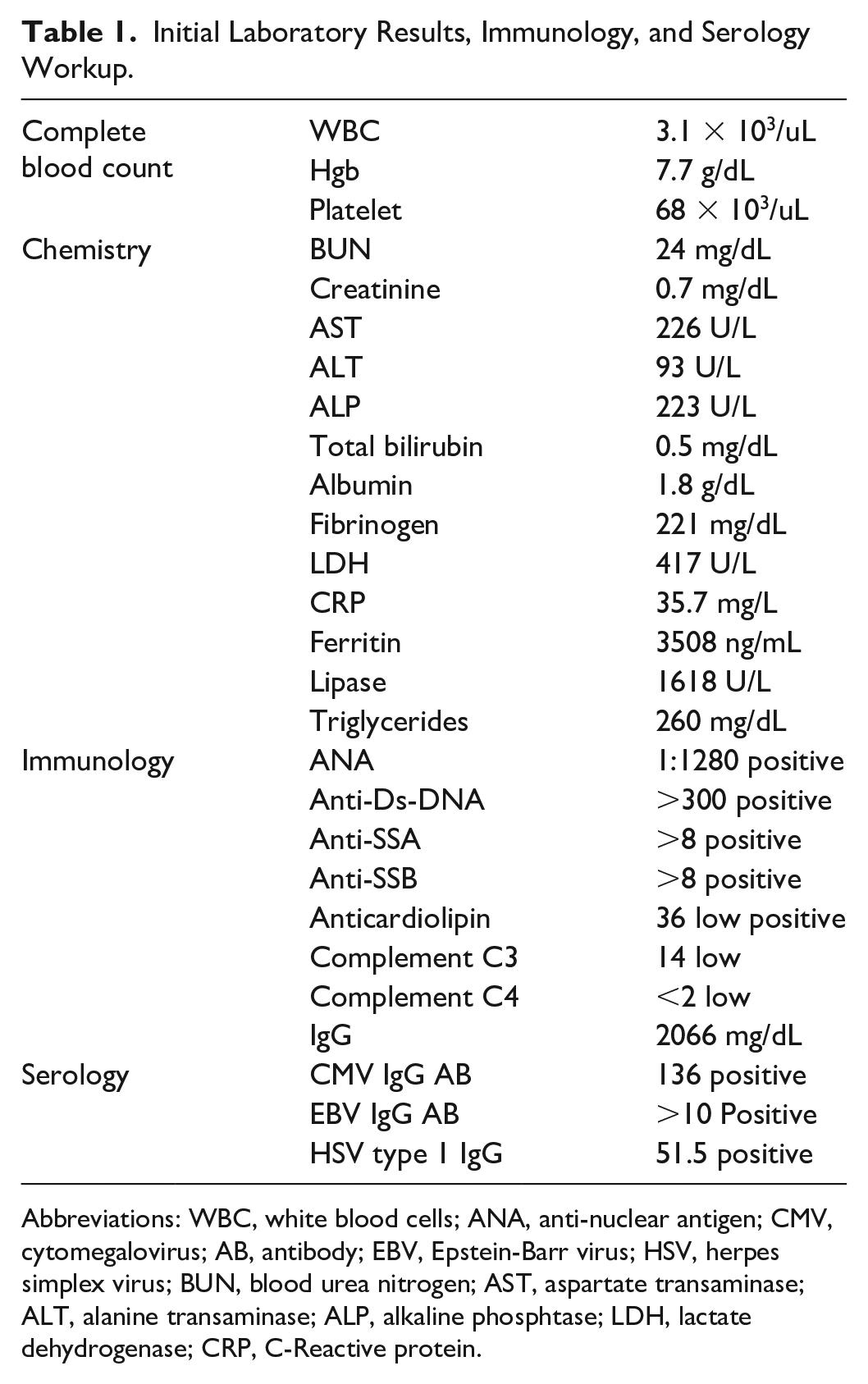
Abbreviations: WBC, white blood cells; ANA, anti-nuclear antigen; CMV, cytomegalovirus; AB, antibody; EBV, Epstein-Barr virus; HSV, herpes simplex virus; BUN, blood urea nitrogen; AST, aspartate transaminase; ALT, alanine transaminase; ALP, alkaline phosphtase; LDH, lactate dehydrogenase; CRP, C-Reactive protein.
Computerized tomography abdomen with contrast (Figure 1) showed ascites, enlarged lymph nodes in the celiac axis, and gastro-hepatic region in addition to mild splenomegaly without focal lesions. In addition, there was an edematous pancreas with significant peripancreatic fluid with a distended gallbladder with sludge versus gallstones. Computerized tomography chest with contrast (Figure 2) showed bilateral axillary lymphadenopathy and patchy consolidations in the lower lobes associated with small pleural effusions.
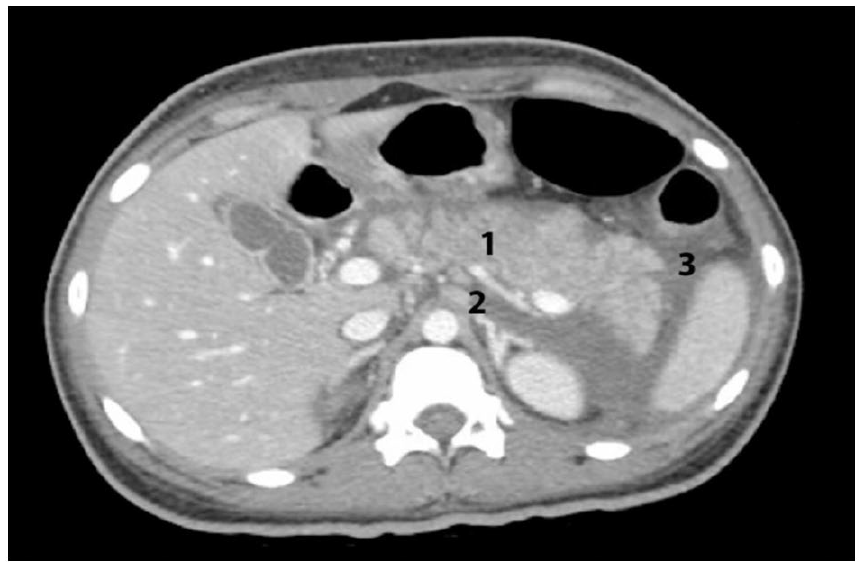
Computerized tomography abdomen with contrast showing (1) an edematous pancreas with significant peripancreatic fluid, (2) enlarged lymph nodes in the celiac axis and gastro-hepatic region, and (3) ascites.
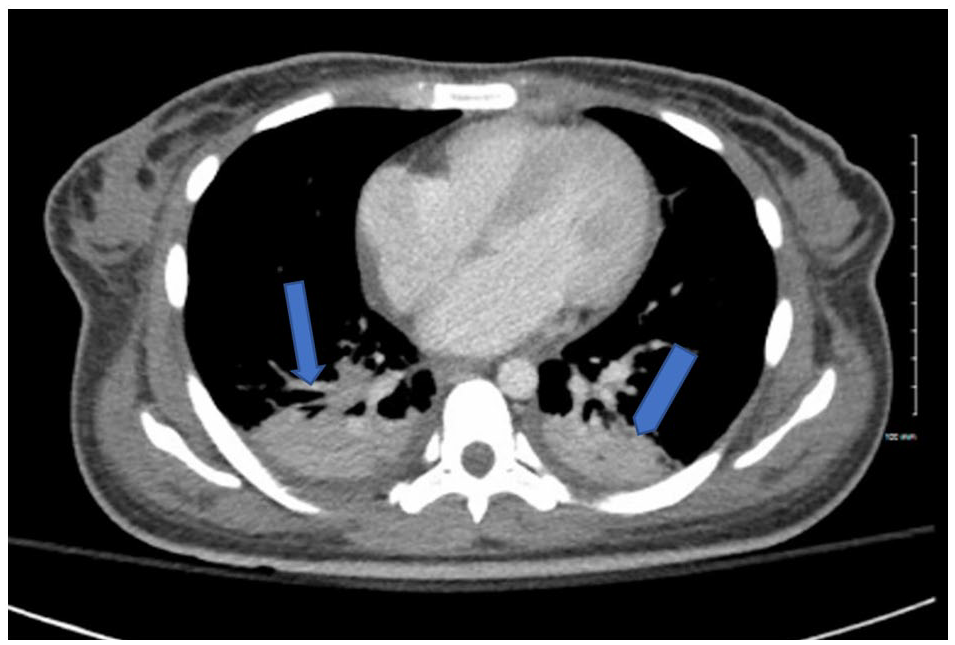
Computerized tomography chest with contrast showing bilateral pleural effusion and patchy lower lobes consolidations.
Immunology workup (Table 1) was remarkable for positive ANA, anti-Ds-DNA, anti-SSA, anti-SSB, and anticardiolipin. Furthermore, she had highly positive IgG titer and low complement levels of C3 and C4.
Peritoneal fluid analysis showed serum ascites albumin gradient (SAAG) of 0.8, which is consistent with an exudative fluid, and the cytology (Figure 3) showed multiple hemophagocytic changes by lymphocytes and histiocytes.

Ascites fluid sample showing hemophagocytic cells.
Given the high suspicion of MAS secondary to SLE, she was started on 1000 mg methylprednisolone for 3 days. Thereafter, a dramatic improvement in her clinical condition was observed, so she was switched to methylprednisolone 40 mg twice daily for an additional 2 days to begin the slow tapering off of the steroids.
Discussion
The association between pancreatitis and MAS in SLE is not coincidental. The pancreas can be targeted by MAS in patients with SLE. 3 Several studies have indicated that 53% to 85% of SLE patients with pancreatitis also have MAS.5,6
Hemophagocytic lymphohistiocytosis (HLH) is a clinical syndrome characterized by excessive and uncontrolled activation of lymphocytes and histiocytes, leading to a cytokine storm and organ dysfunction. 7 This syndrome is typically triggered by infectious agents, autoimmune diseases, or genetic mutations that impair the function of natural killer cells and cytotoxic CD8 T-cells. 7 Macrophage activation syndrome is a specific form of HLH that primarily affects individuals with underlying rheumatological diseases. Macrophage activation syndrome can manifest at any stage of a rheumatologic disease, including at initial presentation, during therapy, or in association with concurrent infections. 7
The diagnosis of gastrointestinal involvement in SLE patients can be challenging. The symptoms can range from mild, such as loss of appetite, nausea, vomiting, and abdominal pain, 8 to severe and life-threatening, including complications like perforation, intestinal infarction, and pancreatitis.8,9 The incidence of pancreatitis in SLE patients varies from 0.7% to 4%. 3 According to a French survey, pancreatitis was the second most common gastrointestinal symptom in patients with SLE. 1
The diagnosis of pancreatitis in SLE primarily relies on clinical symptoms, imaging findings, and elevated lipase levels that are 3 times higher than the upper limit of normal. The underlying cause of pancreatitis in this patient population is still not well understood. Some propose immune-mediated or vasculitis mechanisms as potential factors, 2 while others suggest an association with the use of glucocorticoids. 10 It has been observed that taking oral glucocorticoids for the treatment of SLE may increase the risk of developing acute pancreatitis. 11 Studies indicate that the highest risk of pancreatitis occurs between days 4 and 14 after initiating glucocorticoid treatment. 11
We report the case of a young woman who presented with abdominal pain and an undocumented fever. Her clinical and laboratory findings met 12 out of 17 SLE criteria. 12 Her laboratory results revealed pancytopenia, ANA positive, anti-ds-DNA, anticardiolipin, and hypocomplementemia, and her clinical findings showed malar rash, serositis, synovitis, altered mental status, and alopecia. In addition, our patient met 5 of 8 of the HLH criteria listed in the HLH-2004. 13 She had pancytopenia, hyperferritinemia, splenomegaly, hypertriglyceridemia, and high lactate dehydrogenase levels. She has also developed pleural effusion, ascites, cholecystitis, and pancreatitis. Therefore, the patient was diagnosed with SLE, which manifested as MAS and pancreatitis.
The treatment approach for HLH typically involves managing the immune response, modulating the immune system, and using anti-cytokine medications to suppress the cytokine storm. In the case of secondary HLH, the focus is on addressing the underlying cause. Hemophagocytic lymphohistiocytosis secondary to SLE is often effectively treated with high-dose steroids and immunosuppressants such as cyclosporine, cyclophosphamide, and intravenous immunoglobulins. 14 In cases where standard care is not effective, treatment with rituximab or infliximab, along with tumor necrosis factor (TNF)-alpha inhibitors, has shown success.14,15 Our patient responded well to high-dose steroids and showed significant clinical improvement.
Lupus-related pancreatitis carries a poor prognosis, with a mortality rate as high as 45%. 9 A considerable portion of patients, approximately 22%, may experience recurrent pancreatitis attacks, and about 12% could develop pancreatic pseudocysts. 9 While lupus-related pancreatitis is not common, it can be life-threatening. Physicians should be aware that pancreatitis and MAS can occur concurrently, and there may be an underlying autoimmune disease, such as SLE. Early detection enables effective treatment and helps prevent complications.
Footnotes
Author Contributions
SaeA and SaqA wrote the manuscript. All authors were involved in drafting and editing the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this article.