
Abstract
Right atrial thrombosis, which occurs alone, is rare in clinical practice. Its incidence and mechanism are unclear, but susceptibility factors are usually present at its occurrence: ischemic heart disease, heart failure, atrial fibrillation, and chronic kidney disease. Complete isolated right atrial thrombosis rarely occurs. We report here a 47-year-old male patient with a right atrial mass on cardiac ultrasound and chest computed tomography (CT) and a history of previous right heart surgery with type 2 diabetes mellitus and atrial fibrillation, complaining of “chest tightness and shortness of breath after activity for half a month.” The patient was admitted to the hospital and underwent right atrial mass resection, and the postoperative pathology showed “right atrial thrombus.” As right atrial thrombus is very rare and can be a serious threat to life when it occurs in the heart, the prevention and treatment of right atrial thrombus are very important. Based on the analysis of this case, we believe that for patients with special medical history such as “post right heart surgery and atrial fibrillation,” we need to be vigilant for atrial thrombosis.
Keywords
Introduction
Patients with right atrial thrombosis are often associated with ischemic heart disease, heart failure, chronic kidney disease, and malignancy. Right atrial thrombosis is usually associated with medical devices, and patients with mechanical valves, right pacemaker leads, ventricular or atrial septal closure devices, and indwelling central venous lines are also at higher risk of right atrial thrombosis.1-4 The incidence of right atrial thrombus has a very low probability compared with the left atrium, and even in the setting of atrial fibrillation (AF), right atrial thrombus that occurs alone and without any risk factors is very rare.5,6 It has been suggested that perhaps the superficial attachment of the right atrium and the unfavorable environment for thrombus formation contribute to the formation of this rare case. 7
In a biventricular right ventricle, a muscular band exists in the middle region of the right ventricle, thereby dividing the ventricle into two parts and creating an obstruction between the inlet and outlet portions. The prognosis for patients with untreated right ventricular outflow tract obstruction is similar to that of patients with valvular pulmonary stenosis, requiring surgery when the obstruction is moderate to severe. 8
Here, we report a case of a 47-year-old male with “right atrial mass” and AF who underwent surgery in our hospital 10 years ago for congenital heart disease—double-chambered right ventricle. The patient was considered to have a mucinous tumor on preoperative echocardiography, but the diagnosis of “right atrial thrombus” was confirmed by intraoperative exploration and postoperative pathology of the mass.
Case Report
Presentation
A 47-year-old man (height 170 cm, weight 64 kg) was admitted to the author’s hospital with the complaint of “chest tightness and shortness of breath after activity for half a month.” He was diagnosed with “congenital heart disease (double-chambered right ventricle, mild to moderate aortic regurgitation, dilated ascending aorta, pericardial effusion, and cardiac insufficiency)” and underwent “double-chambered right ventricle correction + tricuspid valvuloplasty”: The right ventricle was separated into a high-pressure chamber and a low-pressure chamber by the abnormal myocardial bundle and septal tissue. The abnormal myocardial bundle and septal tissue were fully excised, the tricuspid valve and its tendon cords were protected, relevant sutures were performed, and then a longitudinal incision was made in the right atrium to reveal the tricuspid valve, and sutures were taken for tricuspid kayoplasty. After cardioversion and discontinuation of extracorporeal circulation, intraoperative esophageal ultrasound showed satisfactory correction of the biventricular right ventricle.
But the patient did not follow the doctor’s orders for regular follow-up after the operation. Currently, the patient has a blood pressure of 170/110 mm Hg, a heart rate of 90 beats/min, an irregular heart rate and a first heart sound of varying intensity, and a short pulse. Electrocardiogram suggests AF, ectopic rhythm, and complete right bundle branch block. Cardiac ultrasound suggests: right atrial mucinous tumor?
Investigations
The patient was admitted to the hospital and the cardiac ultrasound examination (Figure 1A) showed that the right atrium was enlarged. In addition, a 40 mm × 48 mm strongly echogenic mass was seen in the right wall of the right atrium, which was considered to be a mucinous aneurysm; the aortic valve was mildly regurgitated and the inner diameter of the aortic root was widened; and the ejection fraction (EF) was 59%. Chest computed tomography (CT) examination (Figure 1B) showed a hypointense shadow in the right atrium, considered a possible mucinous tumor; the atrium was enlarged. Electrocardiogram (Figure 2) suggested AF, ectopic rhythm, and complete conduction block of the right bundle branch.

(A) Transthoracic echocardiography showed the cardiac mass (40 mm × 48 mm) located in the right atrium. (B) Computed tomography showed a hypointense shadow in the right atrium, considering a possible mucinous tumor; the atrium was enlarged.

ECG suggests (1) atrial fibrillation, (2) ectopic rhythm, and (3) right bundle branch complete conduction block.
Related biochemical tests: coagulation function showed international normalized ratio (INR) of 0.88, which was significantly less than that required after cardiac surgery. Blood glucose was 24.37 mmol/L. He complained that he had no previous history of diabetes and had not controlled his blood glucose, so he performed an oral glucose tolerance test (OGTT): fasting at 14.29 mmol/L and 2 hours after meal at 24.67 mmol/L. He was diagnosed with type 2 diabetes.
Combining the patient’s medical history and relevant examinations, our thoracic surgery department decided to regulate the patient’s blood glucose to meet the surgical requirements and then perform the surgical treatment to clarify the nature of the right atrial mass. The patient’s blood glucose was controlled with menthol insulin (before meal) at 12u in the morning, 8u in the middle, and 8u in the evening, and glargine insulin at 12u in the evening. After the patient’s blood glucose reached the perioperative requirement, “right atrial lesion resection” was proposed.
Treatment
After the patient’s blood glucose reached the perioperative requirement, we proposed to perform a “thoracoscopic resection of the right atrial lesion” in the Department of Thoracic Surgery. After the establishment of extracorporeal circulation, the pericardium was incised, the right atrial blood was aspirated, the interatrial septum was exposed, and the right atrial tumor was found to be about 5 × 4 cm with the tip attached to the comb-like muscle of the right heart, which was completely excised (Figure 3A). Then the wound of the tumor pedicle was burnt with an electric knife. The right atrial incision was closed with 4-0 Prolene sutures, and after complete hemostasis, a right chest drainage tube was placed and the chest was closed with sutures layer by layer.
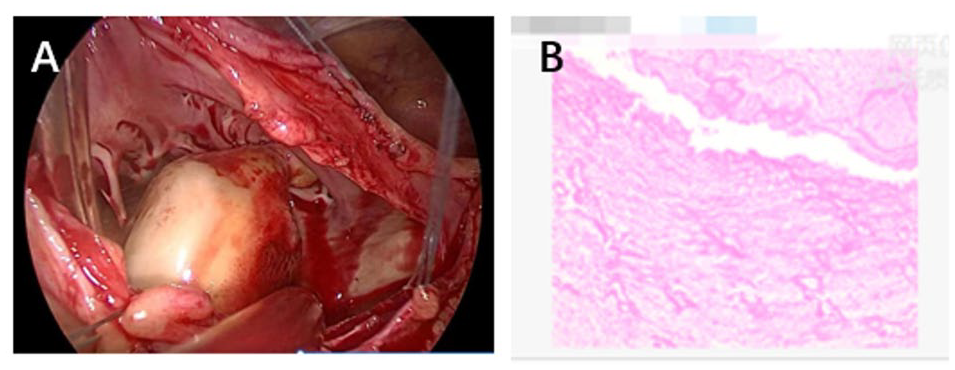
(A) The intraoperative images showed a thrombus-like mass with the root of the tip attached to the right atrium. (B) Histopathological examination revealed a mass consisting calcified deposits, consistent with thrombotic mechanization.
The right atrial mass seen intraoperatively was considered a thrombus, and the postoperative pathology (Figure 3B) suggested that (the right atrial mass) was consistent with thrombotic mechanization, with calcification in the focal area. The pathology was consistent with our intraoperative judgment.
Based on relevant studies and clinical experience, we examined the patient for relevant antibodies to exclude coagulation disorders such as easy thrombosis and Evans syndrome, but the patient’s relevant antibody tests were normal.9,10 This prompted us to think, “What was the cause of the right atrial thrombosis in this patient?”
Discussion
Right atrial thrombosis is rare in cases of associated thrombosis and is usually seen in the presence of risk factors such as malignancy, right atrial catheterization, and procoagulant states. In the absence of other factors, thrombosis in the right atrium alone is rare.1,2
In a case report by Rophila, the morphological classification of right atrial masses was summarized as follows: type A: thrombus with a spiral morphology, highly mobile, can prolapse through the tricuspid valve, and is associated with deep vein thrombosis and pulmonary embolism 11 ; type B: thrombus—not easily mobile, attached to the right atrial or ventricular wall, associated with foreign bodies or structurally abnormal chambers; type C: thrombus is rare and has an appearance similar to a mucinous tumor, that is, it resembles a mucinous tumor and is highly mobile. Combined with the patient’s postoperative pathology, the patient’s right atrial mass was a type B mass.
Atrial fibrillation is one of the important factors of thrombosis, and AF can affect patients with heart disease unrelated to rheumatic heart valve disease. 12 In addition, related studies and clinical practice have shown that AF is more sensitive to the left atrium than the right atrium. 7 Furthermore, one study found that the predominant frequency of AF is located mainly in the left atrium, perhaps inducing an increased chance of left atrial thrombosis. 13
However, the evidence remains contradictory. Some studies have shown that non-valvular AF affects both atria. 14 Brezinov et al 15 suggested that contrary to what other studies have shown, more pro-thrombotic factors are present in the right atrium, including elevated platelet activation markers. 16 However, in an analysis of case reports of AF, the incidence of right atrial thrombus was found to be 3% to 6%, compared with 13% for left atrial thrombus; therefore, right atrial thrombus is less common in patients with an AF etiology. 11 Subramaniam et al 17 suggest that AF is associated with reduced right and left atrial attachments and ejection velocity, and thus the greater width of right atrial attachments and inadequate anatomical remodeling in some patients may explain the association of this group of patients with AF and their right atrial attachment thrombus. Also, Degiovanni et al 18 concluded that a differential diagnosis of thrombus and other intracardiac masses (most commonly atrial mucinous tumors) is needed when faced with a right atrial mass. We need to be alert to the possibility of atrial thrombosis if the patient has a history of prior cardiac surgery and AF or other underlying medical conditions.
In this case, the intraoperative thrombus was observed in a nonmobile form, attached to the right atrial wall, associated with a foreign body or structurally abnormal chamber, with an appearance similar to a mucinous tumor on ultrasound and chest CT. The patient’s coagulation function did not meet the criteria for postoperative cardiac surgery (INR: 0.88) because he did not strictly follow the prescribed oral warfarin anticoagulation therapy after cardiac surgery, and his electrocardiogram showed “atrial fibrillation.” On one hand, the postoperative right atrial surface provided a focal point for the clot and destroyed the original anatomical remodeling structure and, on the other hand, the patient had AF, and the large right heart area reduced the ejection return velocity, thus forming a right atrial thrombus.
Thrombus is the result of local stasis, and thrombus occurs in the atria and can be secondary to heart failure; therefore, patients with confirmed or suspected right atrial thrombus are usually treated with anticoagulants, thrombolytic agents, or surgical thrombectomy, depending on the morphology of the thrombus and the risk of pulmonary thromboembolism. 19 In this case, we had some correctness in the management of this patient. Because complications of AF are usually concentrated in the left atrium, they may lead to under-detection of right atrial thrombus, which can lead to pulmonary embolism, and its easy confusion with atrial mucinous tumor. Therefore, this study concluded that the relationship between AF, underlying disease, and right atrial thrombus requires close attention and treatment, especially in patients with a previous history of right heart surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this article.