
Abstract
Freshwater exposure is associated with a diverse range of infections from pathogens present in soil and water. This includes skin and soft tissue infections and wound infections, gastrointestinal infections, and central nervous system infections acquired through recreational exposure or trauma. Case reports of freshwater-associated infections typically focus on waterborne pathogens as the cause of illness; however, patients who experience significant physical trauma during freshwater exposure may also be at increased risk for infection with their own flora if the nature of the injury allows entry of bacteria through a mechanism such as mucosal injury. Here, we present a case of a healthy 18-year-old man who rapidly developed bacteremia with oral flora following several falls submerging his face into lake water while water skiing, as well as acute polymicrobial sinusitis and subsequent pre-septal cellulitis. Shortly after his water skiing falls, the patient developed sinusitis that rapidly progressed to headaches, emesis, and significant periorbital swelling. Blood cultures grew Prevotella salivae, a bacterium naturally found in the oral cavity. Sinus cultures grew Klebsiella aerogenes and Listeria monocytogenes, which may be associated with lake water. The infection improved with antibiotic therapy, and the patient was discharged on a regimen of amoxicillin/clavulanic acid and trimethoprim-sulfamethoxazole. Reports of bacteremia with oral flora following freshwater injury are not typically reported, and to our knowledge, this is the first report describing bacteremia with P salivae.
Introduction
Freshwater and saltwater exposure can lead to various infections via exposure to pathogens in the water and soil through infection of skin or wounds, inhalation, or ingestion through recreation or trauma. Manifestations include skin and soft tissue infections (SSTIs), ocular infections such as keratitis and conjunctivitis, urinary tract infections, gastrointestinal infections, pneumonia, central nervous system (CNS) infections, and disseminated infections. Bacterial species implicated in water-associated illness include Aeromonas hydrophila, Chromobacterium violaceum, Edwardisella tarda, Erysipelothrix rhusiopathiae, Plesiomonas shigelloides, Pseudomonas aeruginosa, Leptospira, Mycobacterium spp, Shewanella spp, and Vibrio spp, as well as Escherichia coli, Shigella, and Staphylococcus aureus and Streptococcus spp. Other pathogens, such as Cryptosporidium, Giardia, and norovirus also lead to gastrointestinal infections, and the amoeba Naegleria fowleri is associated with devastating meningoencephalitis.1-7
Reports of water-associated illness in the literature usually focus on waterborne pathogens as the cause of disease. However, depending on the nature of the injury and resulting exposure, patients may also be at risk for serious infections with their own flora, such as oropharyngeal flora. In this report, we present a case of an 18-year-old man who rapidly developed bacteremia with oral flora and polymicrobial sinusitis leading to pre-septal cellulitis, shortly after exposure to lake water after several high-speed falls into the water while water skiing.
Case Presentation
A healthy 18-year-old man presented to the hospital with purulent nasal drainage and swelling around his left eye following freshwater exposure. Five days prior to presentation (hospital day −5; see Table 1), the patient went water skiing in West Point Lake in Georgia and fell face-first into the water several times at high speeds. He initially felt fine, but developed left sinus pain and congestion with yellow nasal discharge the following day (day −4). He presented to the emergency department (ED) at an outside hospital where he was prescribed amoxicillin as an outpatient. The next day (day −3), his sinus pain worsened, and he began to develop mild left eyelid swelling. He presented again to the ED; blood cultures were drawn, and the patient was sent home. His sinus pain and periorbital swelling worsened over the next 2 days and symptoms progressed to include severe headaches, emesis, and subjective fevers and chills. He then presented to an urgent care facility (day −1) and his antibiotic was switched to cefdinir. He was then instructed to return to the ED the next day (day 0) as his blood cultures were growing gram-negative rods (GNRs), and he received a dose of vancomycin and piperacillin-tazobactam. Computed tomography scan of the head and orbit showed pansinusitis without orbital involvement. He was transferred to our facility for evaluation by ophthalmology and otolaryngology due to the rapid increase in swelling and pain with initial concern for orbital cellulitis.
Overview and Timeline of Illness, Hospitalization, and Antibiotics.

Abbreviations: ED, emergency department; GNR, gram-negative rod; IV, intravenously; PO, by mouth.
On arrival, vital signs were normal, and the patient was afebrile. Laboratory testing revealed leukocytosis to 16 100/mL with an absolute neutrophil count of 1216/mL and elevated creatinine to 1.43 mg/dL. Physical examination was significant for marked left periorbital swelling and tenderness with minimal to no opening of the eye, tenderness to palpation over the left maxillary sinus, and purulent drainage from the left nare. Extraocular movements were intact, and the patient did not report any pain with eye movement. He had no visual deficits. A bedside nasal endoscopy was performed by otolaryngology for sinus cultures. The outside hospital confirmed their blood culture Gram stains demonstrated GNRs and gram-positive cocci in pairs, and he was given cefepime intravenously (IV) and vancomycin IV and isotonic IV resuscitation (day 1).
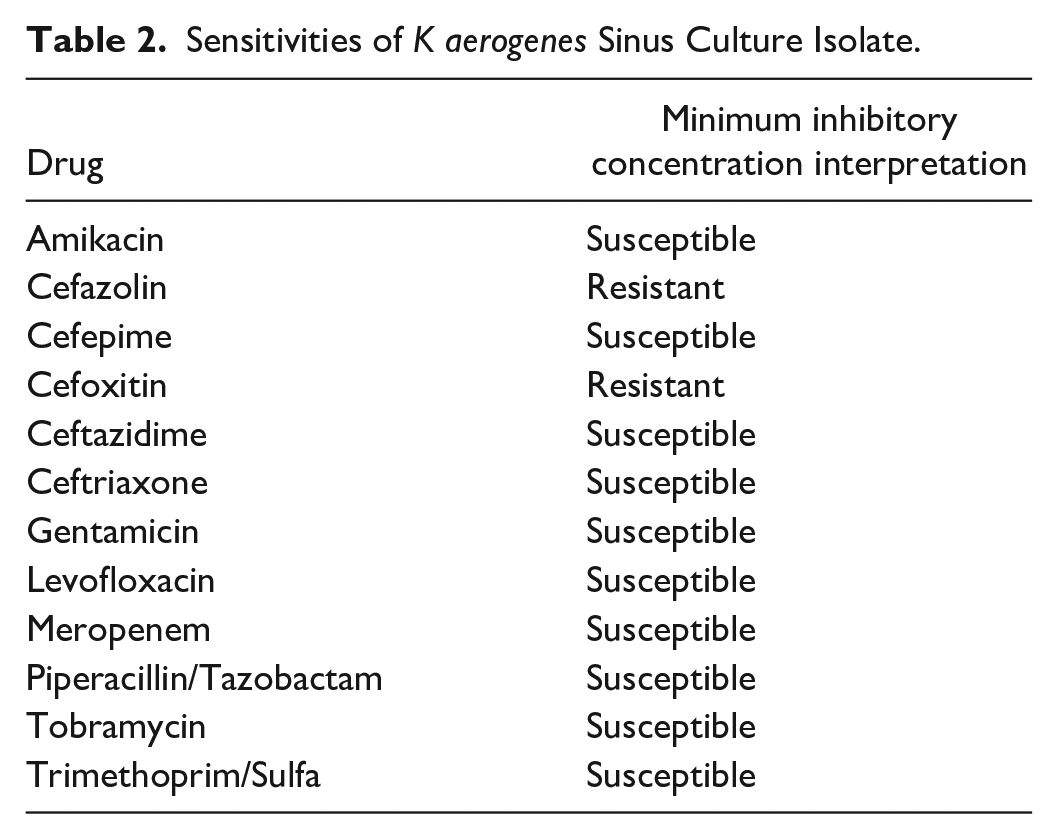
The following day (day 2), the nasal culture from the previous day grew Klebsiella aerogenes. His creatinine was elevated to 1.34 mg/dL, suggesting acute kidney injury (AKI); the vancomycin was renally dosed, and he received another 1 L of Lactated Ringer’s solution. The cefepime was switched to meropenem. He also received metronidazole, as the outside hospital reported the blood cultures were growing anaerobes. Otherwise, the patient’s condition remained stable, still with significant pain and left periorbital swelling, and left nasal drainage. The next day (day 3), blood cultures from the outside hospital further speciated to Prevotella salivae, and the patient was continued on vancomycin and meropenem. His AKI resolved, with a creatinine of 1.08 mg/dL. The next day (day 4), the nasal cultures additionally grew Listeria monocytogenes. The sensitivities of the K aerogenes cultured are shown in Table 2; sensitivities of the P salivae and L monocytogenes were not performed by the microlab. The gram-positive cocci noted on the Gram stain of the outside hospital blood culture ultimately did not grow. The patient was switched to amoxicillin/clavulanic acid by mouth (PO) and trimethoprim-sulfamethoxazole PO per recommendations from infectious disease consultation, as all recovered pathogens and other common bacterial causes were covered by this broad regimen. By this time, his pain and periorbital swelling were much improved, and the patient was able to fully open his eye. He was discharged home the following day (day 5) to complete a total 10-day course of antibiotics with a plan to follow up in the otolaryngology, ophthalmology, and infectious disease clinics. An overview of his illness and hospitalization is presented in Table 1.
Sensitivities of K aerogenes Sinus Culture Isolate.
Discussion/Conclusions
Exposure to freshwater and saltwater can lead to a variety of infections from pathogens present in the water, sand, and soil. Many bacteria associated with such infections are naturally present in aquatic environments, and certain species may be introduced into freshwater environments through fecal matter from humans and animals, such as geese, 8 agricultural runoff, and weather events. The presence of swimmers has also been suggested to stir up sand, soil, and sediment, which may re-suspend pathogens in sediment layers into the water, leading to increased human exposure through recreational activities. 6
Water skiing can lead to injury and infection, although there are currently fewer case reports in the literature specific to infections than injuries. Typical cases include injuries from the tow rope and from falling, such as muscle, tendon, or ligament sprains and tears, abrasions, and lacerations. 9 In addition, hydrostatic injuries to the vagina and rectum have been described,10-13 which result from the high pressure of water entering these orifices that occurs when participants fall backward. Water skiing accidents can also lead to infections from water exposure. The literature includes case reports describing a necrotizing foot infection in a diabetic patient following a water skiing fall, 14 a wound infection with A hydrophila following a water skiing accident involving a tow rope, 15 a case of V parahaemolyticus septicemia after water skiing in a patient with acute myelogenous leukemia, 16 as well as a fatal case of N fowleri meningoencephalitis after a previously healthy patient fell and hit his head on the water. 17 In these cases, as well as most cases describing freshwater injury, the pathogen responsible is associated with the water source.
Interestingly, this patient rapidly developed bacteremia with an oral bacterium, P salivae, and not a waterborne pathogen classically associated with freshwater exposure. As the patient experienced several falls at high speed submerging his face into lake water, it is plausible that the associated trauma to the oropharyngeal mucosa created a portal of entry for the bacteria, rapidly leading to bacteremia. Prevotella is a diverse genus of anaerobic GNRs with a prominence in the oral cavity and gastrointestinal tract, although it is also found in the respiratory tract, vagina, and skin. Prevotella spp can cause both local and systemic infections and are most commonly associated with periodontal and endodontic infections within the oral cavity. 18 Prevotella spp have also been grown from patients with orbital complications of acute sinusitis. 19 Prevotella spp have been implicated in various disease states, including bacteremia, SSTIs, brain abscesses, Lemierre’s syndrome, head and neck infections, genitourinary infections, respiratory infections, and even descending necrotizing mediastinitis from an odontogenic infection. 20 Prevotella spp bacteremia has been documented following dental procedures and dentoalveolar abscesses, an infected decubitus ulcer, and in a patient with heart failure.21-28 To our knowledge, this is the first report identifying P salivae in blood cultures in a case of clinically significant bacteremia.
The patient also developed a polymicrobial sinusitis and pre-septal cellulitis that grew K aerogenes and L monocytogenes in the nasal culture. K aerogenes (formerly Enterobacter aerogenes) is associated with nosocomial bloodstream infections and antibiotic resistance. This species is typically found in the human gastrointestinal tract, but can also be found in soil, human and animal waste, and aquatic environments.29,30 L monocytogenes is classically a foodborne pathogen that causes gastrointestinal disease as well as meningitis in the pregnant, elderly, and immunocompromised. Less frequently, it can cause pulmonary infections, endophthalmitis, necrotizing fasciitis, and focal infections such as joint sepsis.31-33 However, Listeria spp, including L monocytogenes, have been routinely isolated from soil and water, including lakes and rivers, demonstrating that this environmental pathogen can use water sources for dispersion.34,35 It is plausible that exposure to lake water from water skiing led to the polymicrobial sinusitis in the patient, especially given the acute timing of symptom development after exposure. Subsequent spread from the sinus likely resulted in the patient’s pre-septal cellulitis and bacteremia. While orbital cellulitis was initially a concern, this became less likely in the setting of no pain with eye movements and the lack of orbital involvement on imaging.
Of note, the repeat blood cultures drawn at our facility remained negative, and P salivae did not grow in the nasal sinus culture. This makes it difficult to definitively link the patient’s bacteremia to the sinusitis. We believe this is because the patient had already received multiple antibiotics in the days prior to transfer. It is difficult to know whether P salivae contributed to the pansinusitis, as nasal cultures did not grow this species, or if the bacteria were directly inoculated into the patient’s bloodstream through mucosal injury during the trauma of the falls. However, we believe this distinction is not significant to discern regarding management as this clinical scenario should prompt clinicians to pursue broad empiric antibiotic coverage. As the patient was healthy without any symptoms before water skiing, denied any sick contacts, and displayed rapid symptom development beginning shortly after his freshwater exposure, it is likely these events originated from the same incident.
This case—bacteremia with oral flora and polymicrobial sinusitis leading to pre-septal cellulitis in a previously healthy 18-year-old man shortly following exposure to lake water—is unique in that the bacteremia was caused by naturally occurring oral flora rather than bacterial species typically associated with freshwater exposure. Furthermore, while Prevotella spp have been shown to cause sepsis, this is the first report that identifies P salivae as the cause of bacteremia. This case adds to the literature of serious infections following lake water exposure and highlights that the variety of pathogens involved in such cases extends beyond the typical culprits in the water itself. It is important to discuss potential water exposure while gathering patient history in such cases to ensure antibiotic treatments have appropriate coverage.
Footnotes
Acknowledgements
The authors would like to thank Mary Ann Kirkconnell Hall, MPH, for assistance preparing this manuscript. They also thank all members of teams involved in the care of this patient.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient for their anonymized information to be published in this article.