
Abstract
Modern medicine has made tremendous advancements and succeeded in increasing longevity through adequate screening and diagnosis and various new therapeutic approaches. However, alternative medicine is a branch of health care practicing different traditional and unconventional, potentially hazardous therapies to treat commonly known ailments. Standard low-dose vitamin C, ie, 500-1000 mg, is approved in medical conditions like methemoglobinemia, scurvy, burns and also helps iron absorption in anemia. However, toxic doses carry high nephrotoxicity potential like in our case. We present a 74-year-old Caucasian female falling victim to one such alternative therapy leading to acute kidney injury requiring lifelong hemodialysis. She had endometrial cancer and received 100 gm of intravenous vitamin C weekly through a provider for the last 6 weeks as part of this alternate approach to cure her cancer. Upon admission, the serum creatinine level was elevated at 8.2 mg/dl, which subsequently did not improve with conservative management. Renal biopsy revealed diffuse acute tubular injury with polarized microscopy demonstrating calcium oxalate crystals. While her blood vitamin C levels were high, the serum oxalate level was normal. She ended up requiring renal replacement therapy permanently. Alternative medicine continues to be a significant health care hazard with the potential to cause unwanted irreversible nephrotoxicity. Public attention is necessary at various social levels to counter the detrimental outcomes of alternative medicine.
Introduction
Alternative medicine continues to flourish in developed countries like the United States despite modern advancements in evidence-based therapeutics. This medium is a branch of practice where patients are treated with various unconventional and experimental therapies which have yet to be rigorously studied and reviewed. Patients flock to these professionals out of fear, hope, and false advertisement against modern approved therapeutics. So often, we see television advertisements, newspaper propaganda, and social media negativities about these scientifically proven therapy options. One such option, unproven yet often used by these alternative medicine practitioners, is targeted toward patients with cancers whose prognosis is poor. Our patient received a high dose of vitamin C, advertised to improve appetite, reduce pain, and promote quality of life. Vitamin C is approved for scurvy, methemoglobinemia, burns, and vitamin C deficiency. It may also help absorb oral iron in iron deficiency anemia. Even studies are ongoing to interpret if vitamin C effectively improves outcomes in patients with sepsis. The therapeutic approved dose is no more than 2 gm daily as per the regulatory Food and Nutrition Board of US National Academics. 1 The high, toxic dose of vitamin C has been proven to cause hyperoxaluria and complications like acute kidney injury. Acute kidney injury occurs secondary to the deposition of calcium oxalate crystals in renal tubules leading to acute oxalate nephropathy. 2
Case Report
A 74-year-old Caucasian female presented to the hospital after being referred by her oncologist for abnormal outpatient laboratory values. Four years earlier, she was diagnosed with endometrial cancer. She has been getting weekly paclitaxel injections for the last 6 months. Three years ago, she had undergone surgical resection and, after that, was getting chemotherapy through her oncologist. She had previously received carboplatin and pembrolizumab a year ago. She has a history of goiter and thyroid cancer. Her home medications were vitamin C 500 mg daily, ferrous sulfate 325 mg twice daily, and levothyroxine 25 μg daily. Her creatinine was elevated at 6.8 mg/dl when she came in, with blood urea nitrogen high at 113 mg/dl. Hemoglobin was low at 8.5 gm/dl. Her creatinine checked as an outpatient was normal at 1.3 mg/dl 4 weeks ago. She had no diarrhea, vomiting, chest pain, or shortness of breath. She did report decreased urine output recently. Her vital signs were unremarkable, with stable blood pressure, heart rate, temperature, and oxygen saturation, and her physical examination was grossly normal, with no abnormal systemic findings. The rest of the labs were normal and unremarkable. Laboratory values are as in Table 1. Urine was bland with no hematuria, proteinuria, or casts. Renal ultrasound was unremarkable for any obstruction or neoplasm. Initially, she was started on intravenous fluids with isotonic normal saline, but her renal functions did not respond to fluids and kept getting worse.
Laboratory Values.

Abbreviation: RBC, red blood cells.
Upon further history, she admitted receiving 100 gm of intravenous (IV) vitamin C weekly through a person practicing alternative medicine. She has started it for the last 1.5 months, and her last dose was a week before admission. She was getting it to improve her immunity and help with her quality of life and her cancer state. She denied ingestion of excess vitamin C–rich fruits like citrus fruits, peanuts, and rhubarb, nor did she admit to drinking alcohol or any of its derivatives.
Workup for glomerulonephritis, paraproteinemia, and thrombotic microangiopathy was sent—hepatitis B and C virus, anti-neutrophil cytoplasmic antibodies, antinuclear antibodies, complements C4, human immunodeficiency virus, serum immunoelectrophoresis, lactate dehydrogenase, ADAMTS 13. All of them came back negative. Complement 3 was low at 66 mg/dl (normal 92-190 mg/dl). Plasma vitamin C levels were elevated at 259.1 mg/dl (normal being less than 2 mg/dl). Plasma oxalate levels checked later came back within normal limits. However, the normal oxalate level could be an erroneous value due to challenges in analyzing the specimen, which needs rapid collection and swift centrifugation at −80°C. Because of worsening azotemia, anuric state, and acidosis, she was initiated on hemodialysis after 4 days. A kidney biopsy done reported diffuse acute tubular injury accompanied by oxalosis, mild arteriosclerosis with mild interstitial fibrosis and tubular atrophy, with negative features of immune complex-mediated or active glomerulonephritis. Polarizing microscopy revealed numerous polarizable calcium oxalate crystals in the tubular lumen. The biopsy findings are shown in Figures 1 and 2. One and a half years later, she continues to require hemodialysis support, and her urine output has not picked up, unfortunately. She has detached her ties with the above practitioner, and to this day, she is otherwise doing well on periodic chemotherapy and regular follow-ups.

Hematoxylin and eosin staining showing diffuse acute tubular injury with oxalosis, interstitial fibrosis, and tubular atrophy.

Polarizing microscopy with polarizable calcium oxalate crystals in the tubular lumen.
Discussion
Vitamin C metabolism to oxalate was first reported in the 1960s. 3 Almost a century ago, in the 1930s, it was reported how the kidney filters vitamin C and subsequently reabsorbs it. 4 Because the vitamin C excretion pathway is through the kidneys, it is expected that acute kidney injury can develop from high doses of vitamin C. Hyperoxaluria is the primary driving force that causes this injury. The pathology stems from calcium oxalate crystal deposits in the renal tubules resulting in obstruction. 5 Calcium oxalate monohydrate (COM) crystals get endocytosed by epithelial cells in the kidney and incite a proliferative reaction. 6 Nephrocalcin is a glycoprotein in normal human urine which inhibits aggregation, nucleation, and growth of COM crystals and has been demonstrated to block DNA synthesis ability of these crystals. 6 Also, calcium oxalate stimulates specific genes in rebel tubular cells like connective tissue growth factor. This, in turn, promotes interstitial fibrosis and further renal damage. 7
The pathogenesis of hyperoxaluria-induced nephropathy is complex. Tubular fluid saturated with calcium oxalate crystals lead to lumen obstruction, recruiting more macrophages and increasing reactive oxygen species. This draws profibrinogenic and proinflammatory cytokines leading to a cycle of interstitial nephritis, necrosis, fibrosis, and finally, tubular atrophy. 8 Hyperoxaluria can be of two categories—the genetic variant of primary hyperoxaluria and the other type called secondary hyperoxaluria. Type 1 primary hyperoxaluria is mainly from a reduction in hepatic alanine-glyoxylate aminotransferase (AGT) activity causing increased oxalate buildup in the body. Type 2 primary hyperoxaluria results from mutation of enzyme glyoxylate reductase D-glycerate dehydrogenase, causing expanded elimination of oxalate and L-glyceric acid. 2
The most common causes of secondary hyperoxaluria are tabulated in Table 2. Secondary hyperoxaluria results from increased oxalate absorption from the gut (enteric hyperoxaluria), increased oxalate intake in the diet, and increased oxalate synthesis. 8 Other causes include decreased excretion in renal failure. Enteric hyperoxaluria is commonly seen in celiac disease, Crohn’s disease, orlistat therapy, and Roux-en-Y-gastric bypass surgery, where there is a varying degree of enteric fat malabsorption. When fat malabsorption occurs, there is increased available free fatty acids, which bind to the calcium leading to decreased calcium available to bind to oxalate, reducing the average calcium oxalate formation in the feces. This causes heightened absorption of soluble oxalate in the gut. Increased dietary intake is uncommon, reported in a few cases of excess star fruit juice ingestion or peanut intake. Increased production of oxalic acid has also been noted when there are increased oxalate precursors such as glyoxylate, which is elevated in the setting of ethylene glycol and vitamin C ingestion. Last, though uncommon, chronic renal failure patients can also suffer from secondary oxalosis. The authors suggest it is related to increased plasma oxalate levels with longer duration of azotemia leading to exceeding solubility product of calcium oxalate and thus tissue deposition. 9
Secondary Oxalosis Causes.

Excess vitamin C ingestion/injection has been reported to cause acute kidney injury and should be cautiously watched and discouraged. We did extensive research on PubMed and Google Scholar on the nephrotoxicity of high doses of vitamin C. So far, 21 cases of acute kidney injury from toxic doses of vitamin C have been published. They are depicted in Table 3.2,5,8, 10 -27 Apart from 3 instances,11,13,21 and another case where the patient declined dialysis, 16 all of them required hemodialysis support. There have been reported cases of 1-time doses of 60 gm of IV bolus vitamin C 13 and twice of 45 gm of IV vitamin C dosage.10,11 The highest dose reported so far has been 220 gm IV total. 20 The patient received this high dose to recover from an extensive burn injury. In the other instance where 2 patients were given a high dose of vitamin C IV, ie, 112 and 160 gm, respectively, 26 both had severe sepsis, and it was attempted as a therapy to improve the sepsis outcome. On the contrary, our patient had the maximum amount recorded so far (100 gm x 6 = 600 gm), and she received it as a practice of alternative therapy. Along with this, she was also on a daily dose of vitamin C 500 mg tablets, so the cumulative dose might have been much higher. Unfortunately, she never had the chance to recover from kidney failure and remains dialysis dependent. There were three instances where alternative therapy prescribed megadose of vitamin C was used,13,22,23 but none of them had such a high dose as our case. Thus, we must be very cautious about the amount of vitamin C that can be safely used to prevent renal failure and dialysis. In a reported survey by Auer et al, 66% of the general population take vitamin C either as part of a multivitamin supplement or on its own. They also reported that ingestion of megadose of vitamin C exceeding recommended daily allowance is very common. 28
List of Published Cases in Chronological Order With References.
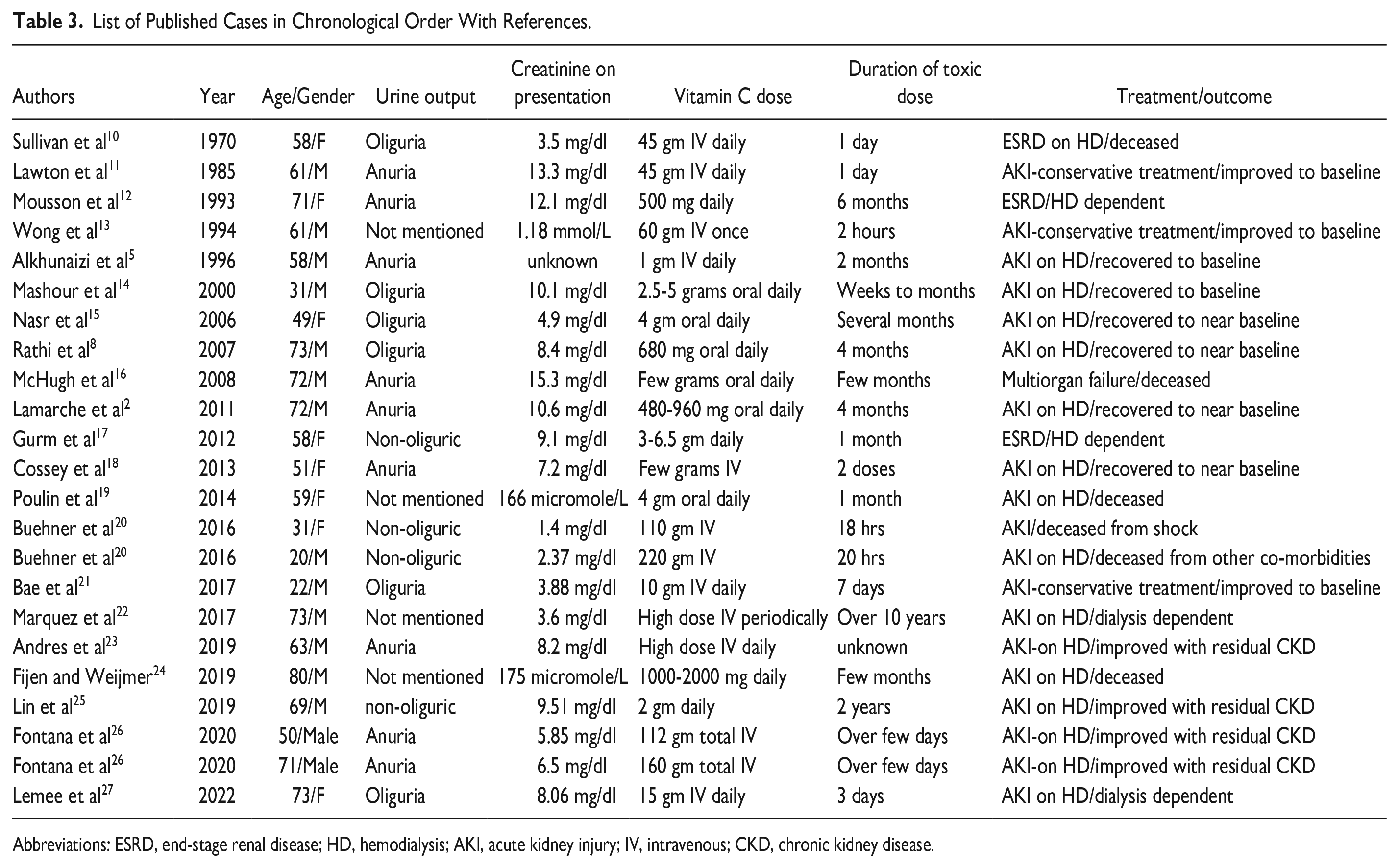
Abbreviations: ESRD, end-stage renal disease; HD, hemodialysis; AKI, acute kidney injury; IV, intravenous; CKD, chronic kidney disease.
Also called ascorbic acid, vitamin C is a water-soluble vitamin that helps grow collagen and wound healing. Commonly approved therapy with vitamin C is scurvy or vitamin C deficiency. 29 Because of its antioxidant property, there have been encouraging ideas about using it in chronic degenerative diseases like cardiovascular diseases and cancers. 29 More recently, vitamin C IV has been attempted in sepsis patients, and authors have concluded that it has no benefits and found it harmful. 30 Because of its antioxidant nature, it was thought to benefit a patient with cancer. However, studies have repeatedly proved that it has no benefits,31,32 and more extensive, randomized trials are needed to prove its valuable role.
Alternative medicine is practiced worldwide with no scientific evidence-based data but with traditional ideas passed through generations. These therapies pose a risk to conventional medical methods and therapeutics. 33 Various forms of herbs and other products are used either in grocery stores or sold online. Even some licensed providers are advocating and promoting these therapies. These agents have yet to go through rigorous clinical trials and research like modern therapeutics and pose a risk to the effectiveness and benefits of conventional treatment. The alternative therapist has tried to utilize this principle of antioxidant nature of vitamin C, as in our case. However, we have seen the harmful consequences of it in our patient.
Treatment of hyperoxaluria-induced nephropathy is non-specific and mainly governed by interrupting the pathogenesis. The preferred options are increased fluid intake, a low oxalate diet, discontinuing vitamin C and calcium tablets, thiazide diuretics to reduce urine calcium, and adding sodium bicarbonate tablets to enhance urine citrate. Tubular fluid citrate is the predominant factor inside the body that prevents calcium oxalate precipitation; this level decreases with metabolic acidosis, and hence alkali salts like sodium bicarbonate or citrate help to negate it through increasing urine citrate levels and thereby reduce urine calcium deposition. Vitamin B6, through promoting the conversion of glyoxylate to glycine instead of oxalate, can also be helpful. 8
Conclusion
Acute kidney injury can occur from toxic doses of vitamin C, which can be organ-threatening and lead to end-stage renal disease like our patient. Although vitamin C has favorable antioxidant effects, which can be helpful in degenerative diseases like cancer and cardiovascular diseases, studies have not proven them beneficial yet. More strict licensing and regulation must be made to prevent the practice and unregulated use of these medications. Clinicians and citizens need to be aware of the detrimental effects of these alternative practices so that they stop alluding to these dangerous treatment options.
Footnotes
Authors’ Note
Author Contributions
SR reviewed patients’ charts. SR, PC, VS, PE, SP, and SA contributed in writing introduction, discussion, and conclusion. All authors contributed equally to preparation of this manuscript, and all the authors reviewed the manuscript and agreed with the findings and interpretation.
Data Availability
PubMed, Goggle Scholar databases. The authors declare that data supporting the findings of this article are available within the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethics approval for reporting individual cases.
Informed Consent
Written informed consent was obtained from the patient for her anonymous information to be published in this article.