
Abstract
Central venous catheters (CVCs), regarded as lines of life, are helpful in hemodynamic monitoring and delivering medications to patients. However, there are several complications that can result from the placement of CVCs. This includes accidental arterial puncture, which has a temporal association with hemorrhage, hematoma, and stroke. Infusion of vasopressors through such a mispositioned arterial CVC further increases the risk of these complications with potential end-organ ischemia. Here, we discuss the case of a 76-year-old woman who developed a myocardial infarction, heart failure, and subarachnoid hemorrhage following the arterial infusion of vasopressors through a malpositioned CVC.
Introduction
Placement of a central venous catheter (CVC) is a commonly performed bedside procedure that allows monitoring of hemodynamic parameters and administration of medications that cannot be safely delivered through peripherally placed venous catheters. In the United States, it is estimated that nearly 5 million CVCs are placed each year. 1 Despite many advancements in point-of-care imaging techniques, complications commonly arise with the placement of CVCs. The most common among these include infection, thrombosis, or mechanical complications.2,3 Examples of mechanical complications include hematoma formation, pneumothorax, and arterial puncture. 1
When unrecognized, the cannulation and subsequent dilation of arteries may result in severe neurologic complications and bleeding.4,5 These complications are further compounded by the infusion of vasoactive medications which can cause vasoconstriction in a malpositioned CVC. Here, we present the case of a 76-year-old woman who developed ST-segment elevation myocardial infarction (STEMI), subarachnoid hemorrhage (SAH), and new-onset heart failure following the inadvertent infusion of vasopressors into the aortic arch through an arterially placed CVC. As far as we are aware, this is the first reported case of acute STEMI after direct infusion of vasopressors to the coronary ostia and into the coronary arteries.
Case Presentation
A 76-year-old woman with a significant medical history of type 2 diabetes mellitus was admitted on account of poor oral intake and lightheadedness. On presentation, she was hypotensive with a systolic blood pressure (BP) around 70 mm Hg. On examination, she was alert and had bibasilar crackles on lung auscultation. Neurological and cardiovascular examinations were unremarkable. Covid-19 testing was negative. Chest radiograph showed bilateral infiltrates. Empiric broad-spectrum antibiotics were started.
Her BP, however, remained persistently in the 70s/40s mm Hg despite the infusion of intravenous fluid boluses. Due to difficulties encountered with the right side, a left-sided central venous catheter (CVC) was placed emergently, and norepinephrine infusion was initiated. Following post-procedure chest radiography, the catheter was retracted 6 cm as recommended (Figure 1A). Follow-up chest radiography reported appropriate placement (Figure 1B). Her BP remained borderline with systolic BP in the 90s mm Hg despite escalation of pressors to vasopressin and the maximal dosing of norepinephrine per institutional protocol.
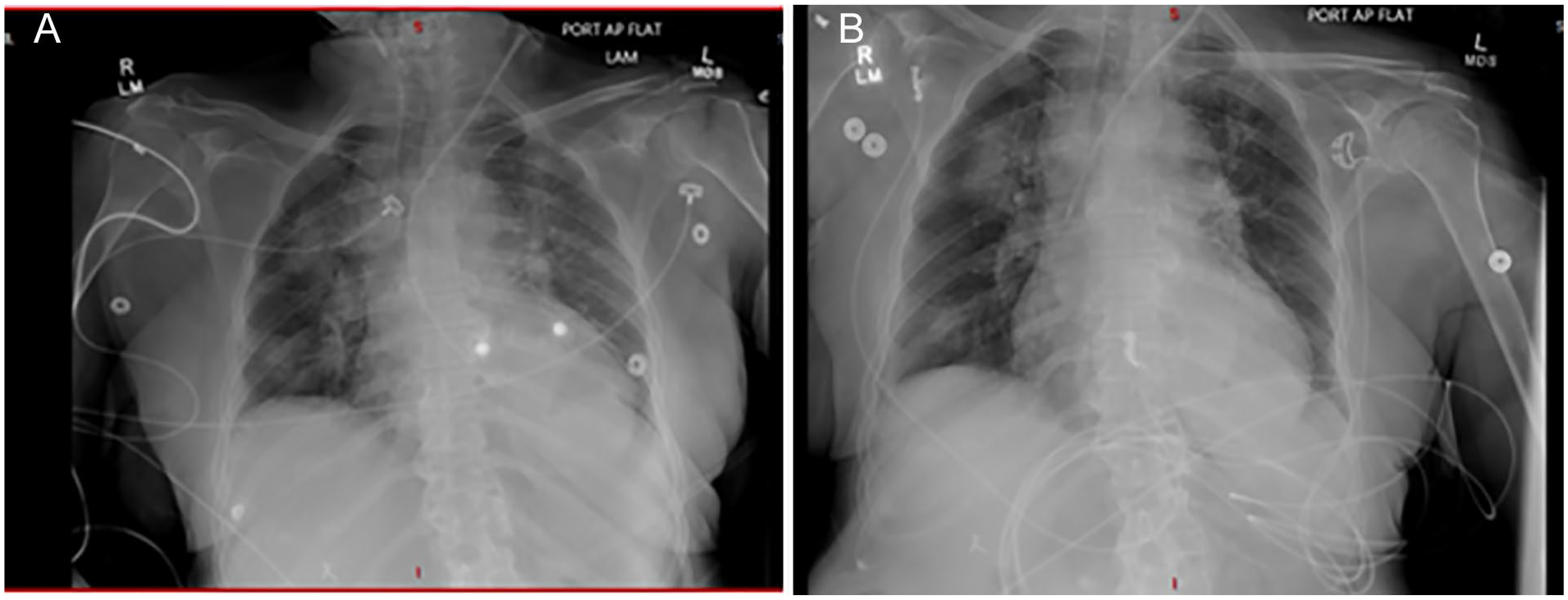
Post-CVC placement chest radiographs, with (A) excessively advanced CVC and (B) CVC after 6-cm pullback (arrows show catheter tips).
A few hours later, the patient developed altered mental status, left-sided weakness, and chest discomfort. Electrocardiogram (ECG) at this time showed new anterolateral ST elevation that was absent on the admission ECG (Figures 2 and 3). Troponins were elevated and trended upward in acute coronary syndrome (ACS) fashion peaking at 1583 pg/mL (reference range, 5-58 pg/mL). Echocardiogram showed a newly reduced ejection fraction (EF) of 45% and hypokinesis in the mid-inferior septal and apical septal left ventricular wall segments. Computed tomography (CT) of the head showed no acute bleed. Computed tomography angiography (CTA) of the head and neck incidentally identified a CVC catheter within the left common carotid artery, with the tip lying within the ascending aorta (Figure 4). Vascular surgery was emergently consulted, and the central line was removed with only manual pressure applied. Cardiology was consulted. It was presumed that direct infusion of vasopressors into the coronary arteries induced vasospasm and led to the patient’s STEMI and subsequent cardiomyopathy. Cardiac catheterization was therefore not pursued, and the iatrogenic nature of the complication was explained to the patient’s family.

Admission electrocardiogram with no acute ischemic changes.

Electrocardiogram showing anterolateral ST elevation.

Computed tomography angiography of the head and neck showing central venous catheter tip in the carotid (arrow).
The patient’s mentation continued to deteriorate. A repeat CTA showed trace left frontal SAH. She also had renal dysfunction requiring intermittent hemodialysis. Her Glasgow coma scale at this point was 3. She also developed seizures that were controlled with levetiracetam and valproic acid. Unfortunately, the patient did not fully recover neurologically and was discharged to hospice care following a discussion of goals of care with the patient’s family. Her case was discussed in morbidity and mortality and brought to practice performance and review. This allowed case analysis to be performed using root cause analysis to close the loop so that no future incidents like this occur.
Discussion
More than 15% of CVC placements are associated with some degree of complication, including pneumothorax and arterial puncture.1,5 Risk factors that increase likelihood of CVC misplacement include obesity, short neck, hypotension, and inexperience on the part of the proceduralist. 4 Hypotension has been associated with an increased risk due to the decrease in pulsatile backflow that otherwise aids in identifying inadvertent arterial cannulation.4,6 Our patient’s shock state could have contributed to the difficulty of identifying an accidental arterial puncture during her CVC placement.
The incidence of accidental arterial puncture varies and is dependent on technique. Using landmark techniques, between 1.0% and 9.4%1,2 of attempted CVC placements result in arterial puncture and between 0.1% and 0.5%7,8 result in arterial catheter placement. These numbers improve with ultrasound guidance. One systematic report identified a 70% reduction in advertent arterial puncture using sonographic guidance. 7 Overall, accidental arterial puncture has been reported to constitute about 5% of all complications. 1 The risk of hematoma, stroke, or neurologic injury approaches 30% once the catheter has been arterially placed.7,9 The risk of thrombus, neurologic deficits, and eventual stroke increases with prolonged arterial catheterization time. Therefore, timely diagnosis through radiography, arterial waveform transduction, or analysis of blood gases is critical to preventing a poor patient outcome. 7
The risks of these complications are increased even further when patients receive vasopressors through the arterial cannulas as in our patient. The role of catecholamines and pressors in inducing coronary ischemia has been previously reported.8,9 For example, post–return of spontaneous circulation ST-segment elevation was reported following vasopressor infusion in a patient without underlying obstructive coronary artery disease.9-11 The excessive catecholamine infusion stimulates vasospasm causing widespread ischemia of the affected arteries. Our patient developed STEMI following accidental cannulation and infusion of vasopressors through the coronary ostia. Apart from the direct vasospastic effects of catecholamines, some studies reported the development of contraction band necrosis in patients with catecholamine excess as a possible pathologic basis. 12
Prompt detection of arterial cannulation significantly decreases the risk of complications such as hematoma and stroke. 4 Our patient developed SAH which has been associated with increased sympathetic activity and further independent induction of myocardial damage and cardiac dysfunction. This may have further contributed to the myocardial infarction that our patient developed. 12
It is important to consult vascular and endovascular specialists following accidental arterial cannulation to determine the safest method of catheter extraction that minimizes patient risk. 7 Potential options include removal of the catheter and manual compression, utilization of endovascular treatment modalities including percutaneous closure devices and stent grafts, embolization, and removal through open surgery.7,13 We consulted vascular surgery who removed the CVC without any further surgical intervention. Treatment options depend on the unique circumstances of the case, including the vessel that was injured and patient comorbidities, bleeding diathesis, and vessel thrombosis. 7 If the CVC is removed early enough, there may be complete recovery. Our patient, unfortunately, had unfavorable outcomes including SAH, ACS, and cardiomyopathy. This is, to the best of our knowledge, a previously undescribed case of STEMI and acute heart failure complicating inadvertent arterial CVC placement and subsequent vasopressor infusion.
Conclusion
Inadvertent arterial catheterization is a catastrophic complication that can transform CVC from a lifeline to a line that brings morbidity, disability, or even death. It is imperative to implement safety measures to avoid accidental arterial catheterization and to ensure early recognition of arterial puncture. It is also crucial that a central line not be used until its exact position can be assured.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Informed consent for patient information to be published in this article was obtained.
Prior Presentation of Abstract Statement
Abstract has not previously been presented.