
Abstract
Aspergillus subramanianii is a very rare form of Aspergillus in section Circumdati. Aspergillus subramanianii has been rarely reported or ever published. IgG4 disease is an emerging disease entity that can be a diagnostic challenge. We report a critically ill patient who had invasive A subramanianii pulmonary aspergillosis and posthumous diagnosis of IgG subclass 4 interstitial lung disease.
Introduction
Aspergillus subramanianii is a very rare form of Aspergillus species in section Circumdati.
Only 6 confirmed cases of A subramanianii have been reported to date. Four cases were isolated from pathology samples sent to the Fungus Testing Laboratory, University of Texas Health Science Center in San Antonio, Texas. Isolates came from lung tissue, wound, foot, 1 and thoracic spine. 2 The additional isolate was found in Japan in a patient with onychomycosis after an earthquake evacuation. 3
Lymphoplasmacytic vasculitis is a histopathological finding most associated with IgG subclass 4–related diseases, of which autoimmune pancreatitis is pathognomonic but many organs can be affected. Diagnosis requires the identification of IgG4-positive plasma cells within affected tissues. Serum IgG4 is only elevated in 60% to 70% of patients.
We report a critically ill patient who had invasive A subramanianii pulmonary aspergillosis and posthumous diagnosis of IgG subclass 4 interstitial lung disease.
Case
A 58-year-old man with schizophrenia, restrictive interstitial lung disease for 7 years prior, and methamphetamine, marijuana, and alcohol abuse presented in the pre-COVID-19 era with sepsis, acute pancreatitis, acute kidney injury, and acute respiratory failure.
He was intubated and started on broad-spectrum antibiotics. Computed tomography (CT) of this chest showed diffuse lung infiltrates and bibasilar consolidation (Figure 1). His cultures from bronchoalveolar lavage (BAL) on hospital day (HD) 2 revealed Aspergillus species (Figure 3). Serum IgG subclass 4 was 15.4 mg/dL (4-86 mg/dL). Tracheal aspirate cultures HD 5 grew Stenotrophomonas maltophilia and Trichosporon asahii. He was found later to have Candida glabrata fungemia on HD 9 and Candida parapsilosis funguria on HD 25. He was placed on micafungin. Follow up chest imaging (Figure 2) was worse. Repeat BAL on HD 28 revealed Aspergillus species again and his antifungal changed to voriconazole. Serum galactomannan was eventually detected on HD 30.

HD 1. CT chest abdomen and pelvis without contrast. Diffuse lung infiltrates and bibasilar consolidation. Not visible at this level are cholelithiasis, left kidney cysts, colon wall thickening, and normal-appearing pancreas (Lipase 2152 on HD 1.).

HD 27. CT chest without contrast. Bilateral diffuse interstitial changes and patchy areas of consolidation with air bronchograms. Bilateral pleural effusions left greater than right and mediastinal adenopathy are not visible at this level.

HD 2. Bronchoalveolar lavage. Sabouraud Dextrose Agar. Aspergillus submaranianii.
Records from patient’s pulmonologist from 6 years prior were reviewed. Pulmonary function testing at that time suggested restrictive lung disease and the plan was to observe.
On HD 37, given the prior history of interstitial lung disease and failure to improve, the patient underwent a lung biopsy. Fungal cultures from biopsies obtained from the upper left lingual and left lower lobe revealed positive fungal slants and Aspergillus species on microscopy (Figures 4 and 5). Fungal identification and susceptibility performed at reference lab revealed A subramanianii (Voriconazole MIC 0.5 µg/mL) (U. Texas Health Science, San Antonio, Texas). Unfortunately, he remained dependent on mechanical ventilation via tracheostomy and did not recover. His code status was changed to comfort care, and he deceased.

HD 37. Left lung biopsy fungal slants.

HD 37. Left lung biopsy. 40× wet mount, lactophenol cotton blue stain, Aspergillus species. A subramanianii by phenotypic characterization and DNA sequencing at reference lab.
Posthumously, pathology revealed lymphoplasmacytic vasculitis with clusters of noninvasive fungal hyphae consistent with aspergillosis (Figures 6 and 7). Tissue invasion was not seen on the histopathology stains. Based on pathology findings, additional IgG and IgG4 immunohistochemistry stains of lung biopsy were performed and demonstrated an increase in relative percentage of IgG4 compared with IgG (50%) (Figure 8A-D).

HD 37. Left lung biopsy. 10× Hematoxylin and eosin. Hyphae seen within intra-alveolar material (black arrow). Intra-alveolar pigmented macrophages in desquamative interstitial pneumonia pattern (red arrow) with scattered lymphoplasmacystic vasculitis (green arrow).

HD 37. Left lung biopsy. 40× Hematoxylin and eosin. Hyphae seen within intra-alveolar material (black arrow). Pigmented macrophages in desquamative interstitial pneumonia pattern (red arrow).
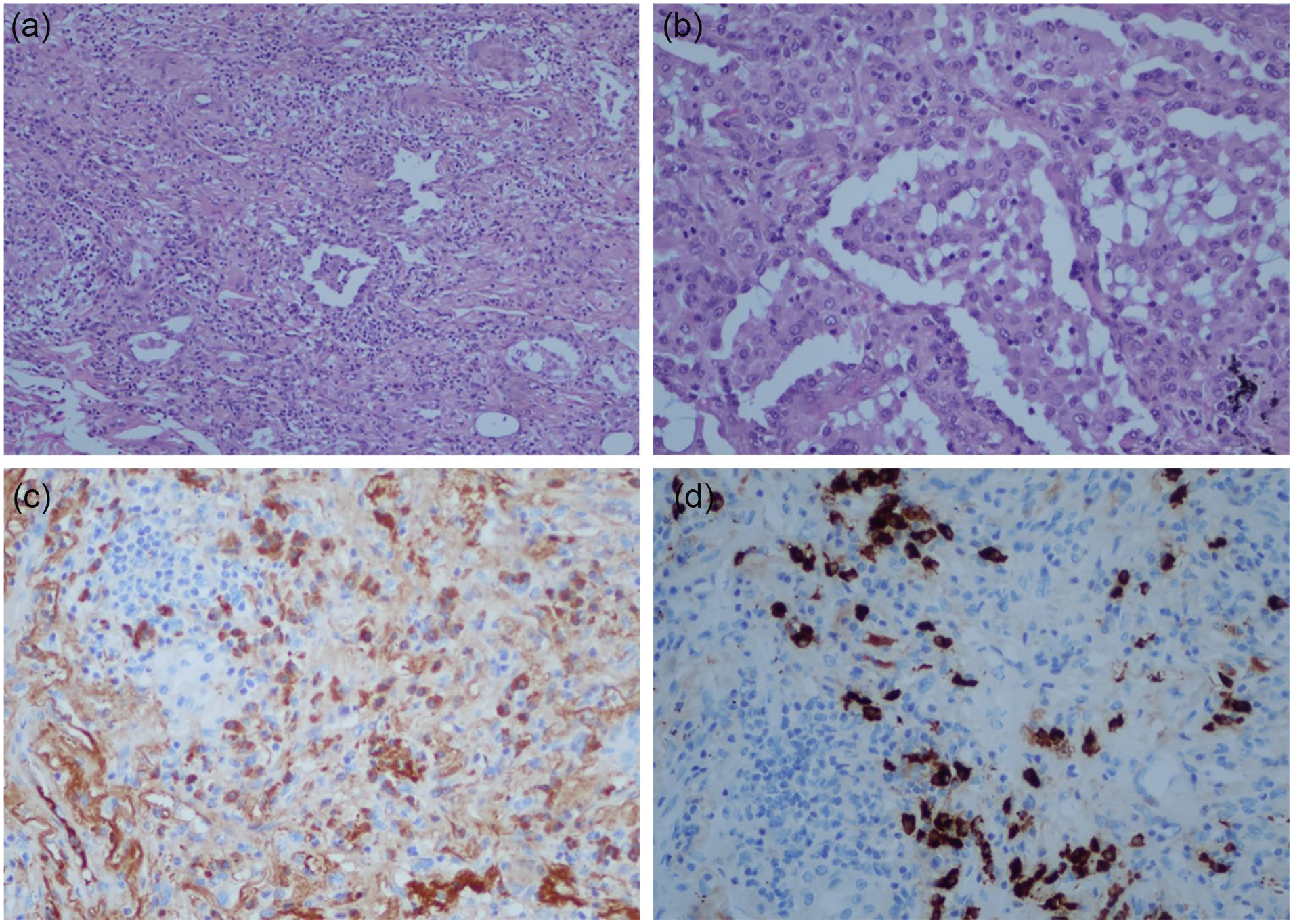
HD 37. Left lung biopsy. Hematoxylin and eosin, IgG and IgG4 staining. IgG4 stain was greater than 50% of background IgG, confirming IgG4 pulmonary disease. (A) Hematoxylin and eosin ×10 magnification. (B) Hematoxylin and eosin ×20 magnification. (C) IgG immunohistochemistry stain for background to compare with IgG4 staining (Figure 8D). (D) IgG subclass 4 immunohistochemistry stain shows greater than 50% intensity compared with IgG (Figure 8C) consistent with IgG4 infiltrative disease.
Methods Used
Fungal identification and susceptibility of A subramanianii performed at reference lab (U. Texas Health Science, San Antonio, Texas) by phenotypic characteristics and DNA sequencing of target TUB and CAL genes and CLSI broth dilution (M38-A2) method. Stenotrophomonas maltophilia identification and sensitivities and T asahii identification were performed with VITEK 2 (bioMerieux, Durham, North Carolina). Trichosporon asahii identification confirmation and sensitivities performed by Focus Diagnostics, Cypress, California.
Discussion
Aspergillus subramanianii has been reported 6 times in the literature to date.1-3 This case would be the seventh (Table 1).
Prior Aspergillus subramanianii Cases to Date.

This Aspergillus species is the fastest grower in vitro at 37°C on Czapek yeast autolysate agar at 7 days out of all 6 known species of Aspergillus species in section Circumdati that were tested. 1 This growth characteristic and the deep tissue origins of isolates highlight the potential for human infections. It is virtually morphologically identical to other Aspergillus species using macroscopic and microscopic identification methods. Genetic sequencing is required to speciate. Antifungal susceptibilities also can vary by isolate tested though further standardized testing among isolates is required (Table 2).
Comparison of Aspergillus subramanianii Susceptibilities Reported in Literature.
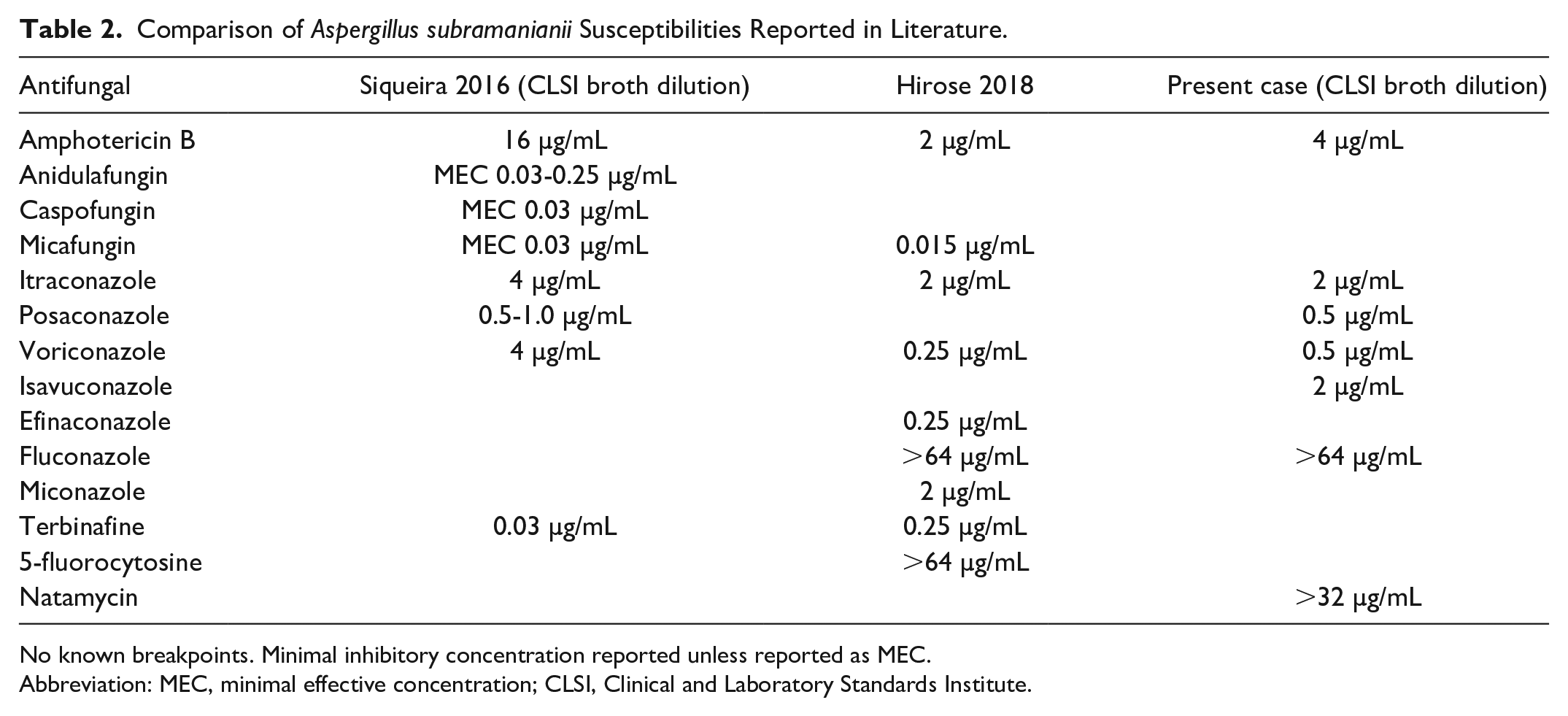
No known breakpoints. Minimal inhibitory concentration reported unless reported as MEC.
Abbreviation: MEC, minimal effective concentration; CLSI, Clinical and Laboratory Standards Institute.
Some species in the section Circumdati can produce a mycotoxin, ochratoxin A, which is a known nephrotoxin. Aspergillus subramanianii produces ochratoxin A inconsistently and/or only in trace amounts. 4 Ochratoxin, a biosynthetic cluster, differs widely among Aspergillus section Circumdati species as well. 5
In hindsight, the antifungal choice of voriconazole in this patient was fortunately appropriate given the MIC values from this strain of A subramanianii in this patient; however, other published strains had higher MIC values. The sensitivity to micafungin of this strain is unknown, but the other strains tested by Texas fungal lab had low MICs. Sensitivities and resistance cutoff points have not yet been determined.
The pathology of lymphoplasmacytic vasculitis only became available after the patient had expired. Serum IgG4 was not elevated in this patient at presentation; however, it could be possible that this patient was one of the 30% to 40% of patients without elevated serum IgG4 levels. Immunohistochemistry of lung biopsy showing an increase in relative percentage of IgG4 compared with IgG confirms pulmonary IgG4 disease (Figure 8A-D). Together with initial CT imaging, the patient likely had underlying IgG subclass 4 interstitial lung disease.
It is difficult to say, if the diagnosis of IgG4 interstitial lung disease was made earlier, would the patient have benefited from corticosteroids given early Aspergillus bronchoscope cultures. Serum galactomannan was detected eventually, suggestive of eventual invasive pulmonary Aspergillus, despite lack of pathological evidence of fungal invasion on biopsy.
Furthermore, infections associated with IgG4-related disease have been reported with tuberculosis, 6 Necator americanus, 7 Helicobacter pylori, 8 and Paragonimus westermani. 9 It is unclear in this case if IgG4-related pulmonary disease was triggered by A subramanianii infection, or if IgG4-related disease came first, and A subramanianii infection was an infectious sequalae.
Coexisting acute pancreatitis at presentation suggests either undiagnosed autoimmune IgG4-related disease or being secondary to polysubstance abuse. The authors hypothesize that pancreatitis likely triggered his decline and subsequent complications of multi-organ failure. Furthermore, a deep pulmonary A subramanianii infection and his multiple comorbidities may have affected his ability to recover despite intensive diagnostic and therapeutic interventions.
Footnotes
Acknowledgements
The authors wish to acknowledge Dr Gian Yakoub and the Kern Medical Department of Pathology for their assistance with obtaining additional histology results posthumously. This case report was presented as a poster presentation at the American College of Physicians Southern California Chapter Scientific Meeting, Marina del Rey, CA in September 2017. It was also presented as an oral presentation at the American Federation of Medical Research Western Medical Research Conference in Carmel, CA in January 2018, where it received an Honorable Mention for Outstanding Oral Presentation. Many thanks to Dr. Kevin Deane from University of Colorado for his review of the case.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval to report this case was obtained from Kern Medical Institutional Review Board (Study #17036).
Informed Consent
Informed consent for patient information to be published in this article was not obtained because patient or legal representative was not available in time for publication. The information in the investigator’s written request for “Waiver of Consent” coupled with the written research proposal disclosing the data use plan was reviewed by Kern Medical Center Institutional Review Board to determine that under the conditions of study approval, there should be minimal or less risk for exposure of patient identity. Kern Medical Center Institutional Review Board approved the request for the Waiver of Consent as part of its ethics approval of the study.
Disclaimer
Views expressed in this article are our own and not the official position of the institutions listed.