
Abstract
Acute suppurative thyroiditis is a rare and potentially life-threatening cause of thyroid inflammation requiring prompt recognition and management. There are few reported cases of thyrotoxicosis due to acute suppurative thyroiditis. We are reporting the case of a 9-year-old boy who presented to the emergency room with fevers, neck pain and swelling, night terrors, and emotional lability. He was hemodynamically stable with initial lab work remarkable for neutrophilia without leukocytosis, elevated inflammatory markers, and hyperthyroidism. Imaging of the neck revealed a heterogenous collection in the region of the left thyroid concerning for suppurative thyroiditis and adenitis. He was admitted to the hospital and initiated on intravenous antibiotics. Given lack of significant improvement in pain, he was taken to the operating room for drainage on hospital day 4 with remarkable clinical improvement in pain. He was discharged on oral antibiotics. Lab work obtained on postoperative day 15 showed resolution of hyperthyroidism and decreasing inflammatory markers. Subsequent imaging following resolution of the acute illness did not reveal any anatomic abnormality that may have predisposed him to developing acute suppurative thyroiditis. Thyrotoxicosis as a complication of acute suppurative thyroiditis is a rare occurrence, and is thought to be due to the release of preformed thyroid hormone from damaged thyroid follicles. The thyrotoxic state is often transient and resolves with appropriate management of acute suppurative thyroiditis. This complication is important to recognize, as failure to appropriately diagnose and treat acute suppurative thyroiditis can lead to poor outcomes, such as airway compromise and death.
Introduction
Acute suppurative thyroiditis (AST) is a rare and potentially life-threatening form of thyroid inflammation. While most patients with AST are euthyroid, there are a handful of cases that report thyrotoxicosis as a complication of AST. To our best knowledge, this is the 6th documented case of AST complicated by thyrotoxicosis in a pediatric patient. It is important to recognize thyrotoxicosis as a complication of AST, as AST requires prompt recognition and management to prevent complications of worsening thyroid infection. The thyrotoxic state is typically transient and resolves with appropriate management of AST. However, questions remain regarding appropriate management of AST, with a more recent trend toward more conservative management with ultrasound-guided needle aspiration or percutaneous drainage to avoid surgical intervention. However, much of the evidence surrounding management of AST is anecdotal and documented in case reports with little if any evidence-based guidance for management, especially in the pediatric population. We felt it was important to document a case of successful surgical management of AST complicated by thyrotoxicosis in a pediatric patient.
Case Report
A 9-year-old boy presented to the hospital with a week of progressive fevers and anterior neck pain with decreased range of motion in his neck. Additional symptoms included night terrors, emotional lability, poor appetite, and headaches. One day prior to his presentation, his parents began to notice a change in his voice and swelling in his neck. On initial exam, he was afebrile and hemodynamically stable with a tender and firm anterior neck mass with limited range of motion in his neck. Initial diagnostic testing was remarkable for neutrophilia without leukocytosis, elevated inflammatory markers, and hyperthyroidism. His TSH was suppressed at 0.01 uIU/mL and Free T4 was elevated at 2.7 ng/dL (see Table 1, Figure 1). An ultrasound and subsequent computed tomography (CT) imaging of the neck were concerning for a heterogenous collection in the region of the left thyroid (see Image 1). Given his clinical presentation, lab results, and imaging findings, he was diagnosed with acute suppurative thyroiditis and adenitis.
Thyroid Function Tests.
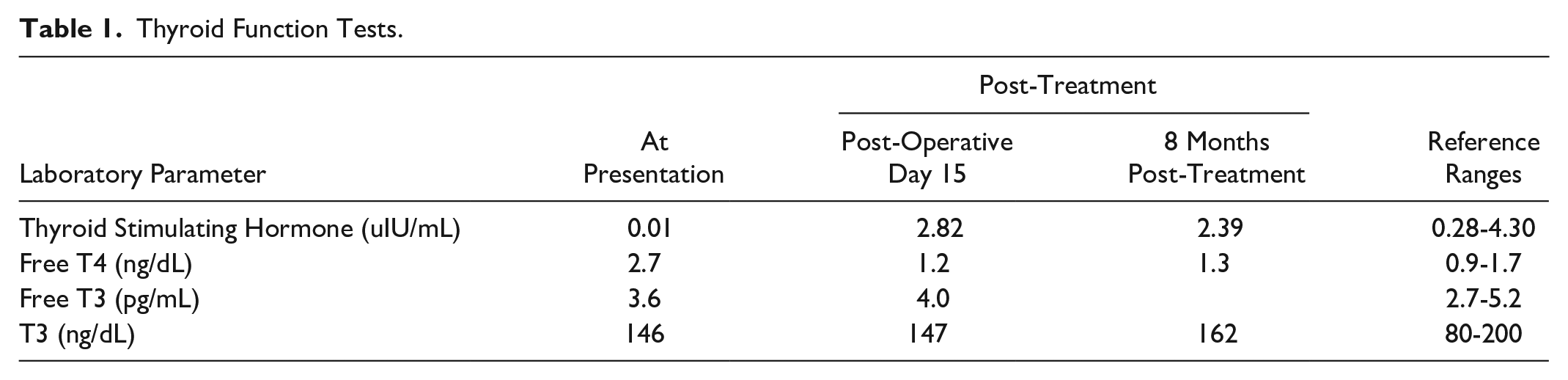

Thyroid function tests throughout the clinical course.

CT neck showing heterogenous collection in the region of the left thyroid.
He was initiated on intravenous ampicillin-sulbactam with minimal clinical improvement. He was taken to the operating room for incision and drainage on day 4 of hospitalization, which resulted in a rapid clinical improvement in pain. Cultures of the drainage grew pan-sensitive Streptococcus anginosus, which is a bacterium commonly associated with oral flora. He was transitioned to amoxicillin-clavulanate to complete a 4-week course of antibiotics.
Several days following hospital discharge, the patient followed up with his pediatrician who noted resolution of the patient’s fevers and neck pain with improvement of his appetite, neck mobility, and other presenting symptoms, including emotional lability. On postoperative day 15, repeat lab work showed normalization of his inflammatory markers and resolution of his hyperthyroidism, now with a TSH of 2.82 uIU/mL and a free T4 of 1.2 ng/dL (see Table 1, Figure 1). Six weeks following hospital discharge, a magnetic resonance imaging (MRI) was performed that did not reveal any anatomical defect that could have predisposed him to developing acute suppurative thyroiditis, though it is important to note that the imaging modality chosen may not have been adequate to find a connecting tract. Thyroid function tests remained normal when checked 8 months following discharge from the hospital (see Table 1, Figure 1).
Discussion
Acute suppurative thyroiditis is a rare and potentially life-threatening diagnosis that if unrecognized can lead to complications such as tracheal compression and airway compromise, bacteremia, mediastinitis, or abscess rupture with extension into adjacent structures.1-6 Reviews of AST cases from the early 20th century report mortality rates up to 25%.2,7 A more recent review of AST cases reported in the literature in the late 20th century reports a much lower, but still significant mortality rate of 3.7% with deaths predominantly occurring in immunocompromised patients. 8 However, there is concern that cases with poor outcomes are underreported. 9 To our knowledge, there are a few hundred reported cases of AST, and only a few dozen of these cases were reported in pediatric patients, the youngest being 3 days of age.2,7,8,10-12
The thyroid gland is relatively resistant to infection given its encapsulated structure, high iodine content, and extensive blood and lymphatic supply.2-4,13-15 The responsible pathogens in most cases of AST are Gram-positive organisms (mainly Staphylococcus and Streptococcus species), though anaerobic bacteria have been implicated as well as several less common organisms, including Klebsiella, Escherichia coli, Haemophilus influenzae, Actinomyces, Mycobacterium tuberculosis, and others.1,3 Infection is thought to occur from one of several mechanisms, including contiguous spread, lymphatic or hematogenous spread, penetrating trauma, or from a congenital malformation, though the route of infection is not always obvious.1-4,7,13,15 Women and those with underlying thyroid disease (such as a goiter or adenoma) are at increased risk of developing AST.1-3,13 It is important to consider the presence of a congenital malformation, such as a pyriform sinus fistula (PSF), as this finding can predispose to thyroid infection and is a common route of infection in pediatric patients with AST.4,8,11,12,14,16,17 Discovery and obliteration of a PSF reduces the risk of recurrent thyroid infection.4,14,16 PSF tend to occur on the left side and historically, literature has overwhelmingly supported barium esophagography as the study of choice in diagnosing PSF after the acute infection has resolved.3,4,9,12,14,16,18 However, there are a few small PSF case series that report better sensitivity for diagnosis of PSF with laryngoscopy and hypopharyngoscopy for direct visualization (which provides the option of endoscopic cauterization if a PSF is found).9,19,20 Ultrasound, CT, and MRI are other options to look for a PSF, though these modalities are not as useful and may not demonstrate a PSF if present.19,21 With guidance from our otolaryngology colleagues, 6 weeks following the acute infection our patient had a neck MRI for potential surgical planning which did not reveal any congenital anomaly or tract, though it is important to note that an MRI alone may not be adequate to diagnose a PSF as mentioned previously. At the time of submitting this publication, our patient has not required further surgical intervention, and has not had recurrence of AST in the 8 months following his acute infection.
Patients with AST typically present with acute onset fever and painful neck swelling with or without compressive symptoms such as dysphagia and hoarseness, and some cases are preceded by an upper respiratory illness.1,2,22 Laboratory findings in AST can include leukocytosis, elevated inflammatory markers, and elevated thyroglobulin, though the utility of measuring thyroglobulin and inflammatory markers has been questioned.3,9 The majority of patients with AST are euthyroid, though both thyrotoxicosis and hypothyroidism have been reported.1-3,8,13,23,24 Diagnosis of AST typically involves imaging with neck ultrasound revealing a heterogenous, hypoechoic area within the thyroid.3,7,13,17,25 In cases of uncertainty, sometimes CT scans of the neck are obtained to confirm the presence of an abscess.4,8,14 In our patient, a CT neck was obtained to further characterize the lesion visualized on ultrasound, especially given the presence of hyperthyroidism on initial lab work. Though nonspecific and unnecessary to confirm the diagnosis, thyroid scans typically show decreased uptake in the area of thyroid involvement.4,23,26 Ultimately, fine needle aspiration with Gram stain and culture helps confirm the diagnosis and provides information on the causative organism and antibiotic susceptibility.1,3,4
There are only a handful of cases that report thyrotoxicosis as a complication of AST in adults.13,14,24,26-31 To our knowledge, there have only been 5 reported cases in pediatric patients.12,17,32 The mechanism is thought to be due to the release of preformed thyroid hormone from the destruction of thyroid follicles.1,13,17,26 In these instances, patients can present with a variety of hyperthyroid symptoms, including anxiety, anorexia, palpitations, diaphoresis, tremors, weight loss, diarrhea, insomnia, and irritability.1,14,17,26 It is important to recognize thyrotoxicosis as a complication of AST because the presentation can be similar to that of subacute thyroiditis; however, the management of AST requires prompt initiation of empiric antibiotics to prevent complications of worsening thyroid infection.1,3,24,30 These diagnoses can typically be differentiated by ultrasound, with subacute thyroiditis demonstrating diffuse heterogeneity and low vascularity and AST demonstrating a heterogenous area in the thyroid concerning for an abscess. 9 Additionally, fine needle aspiration can help differentiate between the 2 entities with AST producing frank pus or purulent material with neutrophils and cellular debris and subacute thyroiditis demonstrating multinucleated giant cell granulomas and mononuclear cell infiltration.9,14,25 In those reported cases of thyrotoxicosis due to AST, the thyrotoxic state is typically transient and resolves with appropriate treatment of AST, though few reported cases in adults have required medications to treat the thyrotoxic state.13,24
Management of AST has traditionally involved a combination of broad antibiotics that are then narrowed based on culture results and surgical drainage.2,3,7,13 A minority opinion is that not all cases require surgical intervention and resolve with antibiotics alone, though if antibiotics fail to control the infection as evidenced by continued pain, fever, and leukocytosis, then surgical drainage is indicated.3,4,14 More recent literature has been in favor of more conservative management for stable patients that involves ultrasound-guided needle aspiration (sometimes with injection of antibiotics into the abscess cavity) or percutaneous drainage as opposed to more invasive measures such as surgical excision or incision and drainage.7,9 In some cases, multiple aspirations are required to achieve clinical benefit. 13 Paes et al 9 published a clinical review and guide to management in 2010 that is largely based on expert opinion given lack of sufficient evidence-based studies of optimal management. In alignment with more recent case reports, they also encourage a less invasive approach to management that involves consideration of recurrent fine needle aspiration of the thyroid rather than surgical management based on clinical presentation. 9 However, these recommendations have been developed largely based on AST case reports in adults. In our opinion, given the low risk of generalized anesthesia and surgical intervention in the pediatric population, we felt that surgical management was a reasonable option. In the case of our patient, this resulted in rapid clinical improvement, and he did not require a second procedure (which may have been necessary if we had approached management with needle-guided aspiration).
Conclusion
Acute suppurative thyroiditis is a rare form of thyroid inflammation in children, and few cases with associated thyrotoxicosis have been documented. It is important to recognize thyrotoxicosis as a complication of AST, as AST requires prompt recognition and management to prevent complications of worsening thyroid infection. Questions still exist regarding the appropriate management of this condition with a recent trend toward more conservative management with ultrasound-guided needle aspiration or percutaneous drainage rather than surgical management. However, given lack of strong evidence, especially in the pediatric population, we felt it was important to document a case of successful surgical management of a pediatric patient with this rare and potentially life-threatening condition.
Footnotes
Authors’ Note
Prior Presentation of Abstract Statement: Abstract presented at virtual ESPR/AFMR 1st Annual Eastern Medical Research Conference March 11 2022.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Pediatric Endocrinology department at University Of Rochester, New York provided financial support for article processing charges involved in the publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Informed consent for patient information to be published in this article was not obtained because our case report does not contain any protected health information (PHI), hence informed consent was exempted by the Research Subjects Review Board (RSRB) at University of Rochester Medical Center.