
Abstract
Ventricular fibrillation can lead to sudden cardiac death. Automatic implantable cardioverter defibrillator (AICD) devices have shown to be highly successful in the termination of these arrhythmias and are a first-line modality of treatment for the prevention of sudden cardiac death. We present the case of a 69-year-old female with a history of paroxysmal atrial fibrillation on anticoagulation with apixaban and rate controlled with metoprolol who presented from home with a chief complaint of hiccups. She had a prior admission to the hospital after she was found to have monomorphic ventricular tachycardia during a nuclear stress test. A cardiac work-up including cardiac catheterization and cardiac magnetic resonance imaging did not show any evidence of significant coronary artery disease or reversible cardiomyopathy. The patient underwent successful placement of a single chamber ICD and was discharged home. Twelve weeks after placement of the AICD, the patient was lifting furniture and experienced sudden onset of hiccups. A chest X-ray showed displacement of the AICD lead from the right ventricular apex to the superior vena cava. The patient underwent lead repositioning with complete resolution of her hiccups. The etiology hiccups was suspected to be secondary to irritation of the right phrenic nerve which travels along the anterolateral border of the superior vena cava. We present the case of hiccups following ICD lead displacement. This serves to highlight a rare complication of ICD displacement that healthcare providers should consider when patients with recently placed ICD devices complain of hiccups.
Introduction
Ventricular fibrillation, often preceded by ventricular tachycardia, can lead to sudden cardiac death. Automatic implantable cardioverter defibrillator (AICD) devices have shown to be highly successful in the termination of these arrhythmias and are used as a first-line modality of treatment for the prevention of sudden cardiac death. 1 Herein, we present an unusual complication of AICD placement that is important to recognize early during presentation.
Case Presentation
We present the case of a 69-year-old female with a history of paroxysmal atrial fibrillation on anticoagulation with apixaban and rate controlled with metoprolol who presented from home with a chief complaint of hiccups.
Of note, the patient had a prior admission to the hospital 3 months before this presentation. At the time, she had been in the process of undergoing a nuclear stress test and developed shortness of breath. She was also found to have monomorphic ventricular tachycardia, which was treated with amiodarone. She was admitted to the cardiac intensive care unit (CICU) for further evaluation. She underwent a cardiac catheterization which showed insignificant coronary artery disease. A cardiac magnetic resonance imaging (MRI) study was performed which showed septal hypertrophic cardiomyopathy and 2 focal areas of hyperintense signal within the thickened interventricular septum on delayed but not post-contrast T1 mapping. The electrophysiology team was consulted. The patient underwent successful placement of a single chamber Medtronic DVPA2D4 ICD. She tolerated the procedure well and she was discharged home.
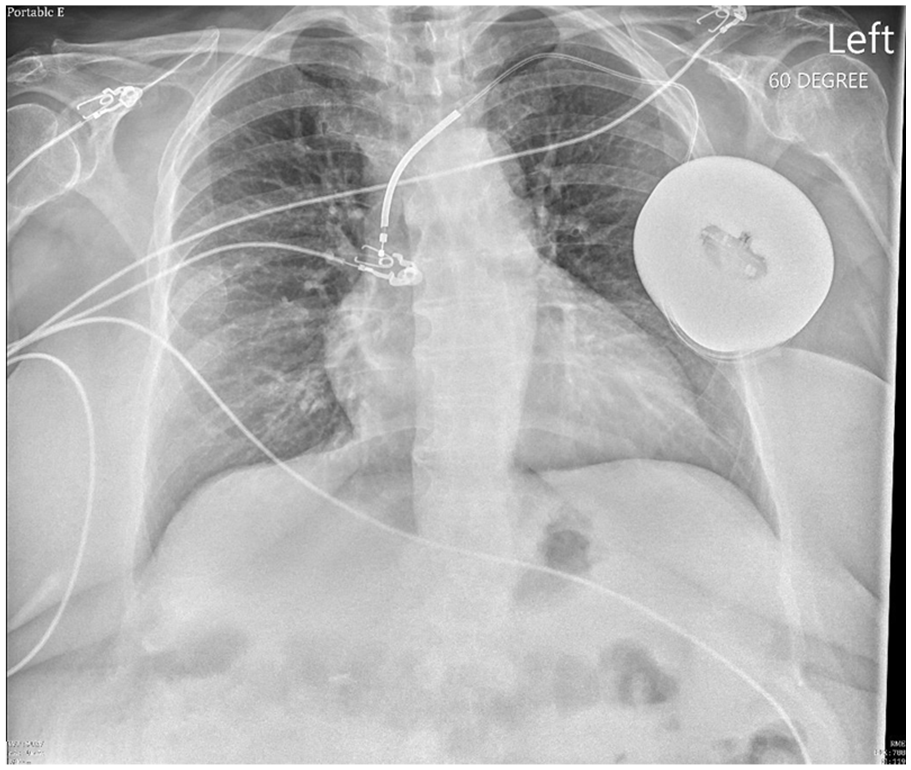
Chest X-ray showing AICD lead in the superior vena cava.
The patient stated that after she went home, she did not have any further episodes of palpitations, chest pain, or shortness of breath. She stated that the night before presentation, she was helping her husband get into bed by lifting him and she noticed that shortly after lifting him, she began to experience the sudden onset of hiccups. She stated that she could feel the hiccups originating from the right side of her body. She states that she tried holding her breath and drinking water, without resolution of the hiccups. This prompted her to come into the emergency room.
On presentation to the emergency room, the patient was hemodynamically stable and afebrile. She had a chest X-ray which showed that her AICD lead tip had been pulled back from the expected position in the right ventricular apex into the superior vena cava. The electrophysiology team was consulted. The patient underwent lead revision. A repeat chest X-ray showed interval revision of AICD device which was now in the right ventricular apex. The patient’s hiccups resolved after revision of the lead. She was discharged home with weight-lifting precautions.
Discussion
AICD placement is indicated in for both primary and secondary prevention of sudden cardiac death (SCD). In primary prevention, AICD devices are placed due to an increased risk of life-threatening arrythmias, whereas in secondary prevention, they are used in patients with a history of ventricular fibrillation or sustained ventricular tachycardia.2,3

Chest X-ray after AICD lead revision with the lead now in the right ventricular apex.
In our patient’s case, the AICD was placed for primary prevention of SCD, given her history of previous monomorphic ventricular tachycardia. Prior to AICD therapy, it is essential to evaluate the patient for possible reversible causes of arrhythmia. 4 This can include derangements in electrolytes, including potassium and magnesium. This can also include arrythmias related to drug-use which could be managed by cessation of the offending agent. A thorough review of our patient’s bloodwork showed no electrolyte abnormalities that could be acted on. Her medication list did not show any agents that may have provoked arrythmia. Structural heart disease and reversible coronary artery disease were also ruled out through evaluation with cardiac catheterization.
Complications in patients with ICD therapy can be further classified into procedure-related complications, generator-related complications, and lead-related complications. In an institutional review of ICD placement and subsequent complications, Alter et. al found that the most common perioperative complications included postoperative fever, side effects of antibiotic prophylaxis, pocket hematoma. 5 Other complications related to the procedural insertion of the ICD include pneumothorax following subclavian vein puncture, perioperative myocardial infarction, perioperative ischemic attack, and thrombosis. 5 Generator-related complications include inappropriate shock therapy, often triggered by supraventricular tachyarrhythmias or artifacts.
In the above study, it was found that 52 patients (12% of the total population reviewed) had ICD lead-related complications. This was further classified into 6% of patients having lead dislodgement. 5 After placement of an ICD, patients are recommended to avoid strenuous activity, especially lifting related to the upper body, avoid traumatic contact to the implant site, and limit arm movements for a period following the procedure.
Our patient performed heavy lifting following the placement of her AICD. This led to displacement of the ICD lead from the right ventricular apex to the superior vena cava. The right phrenic nerve travels along the anterolateral border of the superior vena cava. Due to the proximity of the displaced ICD lead to the right phrenic nerve, our patient presented with a chief complaint of sudden and persistent hiccups.
Saarel et al. 6 present a similar case of hiccups as the warning sign for an ICD lead-related complication. They present the case of an 8-year-old boy who presented to the hospital after ventricular fibrillation cardiac arrest who underwent single-chamber ICD placement with a St. Jude Durata 7122Q lead. The lead was placed 5 days after the cardiac arrest. The ICD implantation was suspected to be uncomplicated, and the patient was discharged home. However, 1 month after ICD placement, the patient presented to the hospital with the complaint of intermittent hiccups. The lead was found to have perforated the right ventricular myocardium requiring surgical lead removal.
Conclusion
We present the case of hiccups following ICD lead displacement and highlight another case documented in the literature of hiccups following perforation of the myocardium. In both cases, the patients underwent lead revision. This report highlights a rare complication of ICD lead displacement that physicians and healthcare providers should consider when patients with recently placed ICD devices complain of hiccups.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.