
Abstract
Small bowel obstruction is a common surgical emergency and frequent cause of hospitalization. Internal hernias account for less than 6% of all small bowel obstruction cases. Less frequently, hernias through the broad ligament of the uterus can occur and account for only 4-7% of total internal hernia cases. We report a case of a small bowel hernia through broad ligament of the uterus in a young female. Multiple diagnostic modalities suggested a ruptured ovarian cyst as the most probable cause for her abdominal pain. However, her symptoms were much more severe than an ovarian cyst would normally produce. Therefore, a diagnostic laparotomy was performed, which found a small intestine hernia through the left broad ligament of the uterus. The diagnosis of intestinal hernias, specifically through the broad ligament, is often delayed due to the infrequent occurrence, varied presentation, and difficulty of confirmation on computed tomography (CT) scan. Surgery is the gold standard for the diagnosis and treatment of internal hernias. This article draws attention toward a rare and potentially life-threatening cause of abdominal pain.
Introduction
Small bowel obstruction is a common surgical emergency and a frequent cause of hospitalization. Intraperitoneal adhesions account for the majority of small bowel obstructions, followed by complicated hernias, and then intestinal tumors. 1 Whereas abdominal wall hernias constitute the majority of hernias, internal hernias account for only 0.6-5.8% of small bowel obstructions. 2 Moreover, herniation through a defect in the broad ligament is even rarer. This is only seen in 4-7% of total internal hernias. 3 Hernias through the broad ligament are more commonly seen in multiparous, middle-aged females who have undergone previous abdominal surgery.
We describe a case of a female who came to the emergency room for abdominal pain, nausea, vomiting, and was unable to tolerate diet. Initially, it was suspected that she had a ruptured ovarian cyst. Multiple diagnostic tests failed to suggest an alternative diagnosis. Laparoscopy revealed a left broad ligament hernia of the small intestine.
Case Report
A 32-year-old G1P1 African American female presented to the emergency room with abdominal pain. She reported a previous surgical history of an uncomplicated cesarean section about 7 years ago. The symptoms started 2 days ago. Initially, the pain was localized in the lower abdomen and then migrated to the epigastric area. She reported her pain to be 10 out of 10, sharp, associated with nausea, vomiting, and unable to tolerate any oral intake. The work-up done in the emergency room consisted of a computed tomography (CT) scan of the abdomen and pelvis with intravenous (IV) contrast. It revealed a ruptured right ovarian cyst. The patient was discharged home. She saw her gynecologist the next day in the office. Her symptoms continued to worsen, and she returned to the emergency room the next day. On examination, her vital signs were stable, there were signs of mild dehydration, and nonfocal abdominal tenderness with normal bowel sounds on auscultation. Significant laboratory findings included: sodium 133 mmol/L, white blood cell count (WBC) 14 400, and urinalysis was unremarkable. The patient underwent another CT scan of the abdomen and pelvis. This again showed findings suggestive of a ruptured right ovarian cyst. The patient also received a pelvic and transvaginal ultrasound, which failed to demonstrate any alternate diagnosis.
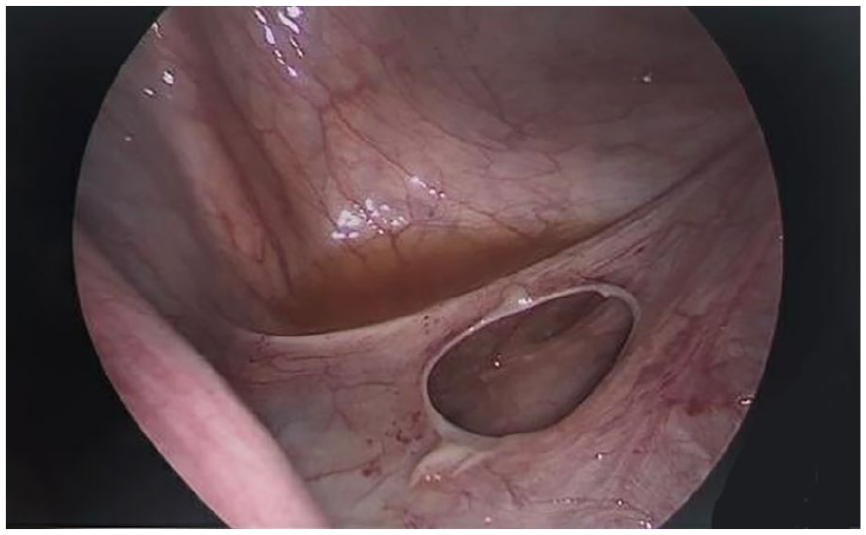
The patient was admitted to the hospital for symptom control and serial abdominal examinations. She was started on conservative management with IV fluid, pain control with nonsteroidal anti-inflammatory drugs (NSAIDs), and narcotics. The patient had minimal relief with conservative management. A gynecologist was then consulted, and a diagnostic laparoscopy was performed. Intraoperative findings noted an incarcerated small bowel within a 2 cm (about 0.79 inch) defect in the left broad ligament of uterus (see Images 1 and 2). A general surgeon was consulted for intraoperative evaluation. The small intestine wall was meticulously evaluated, noting edema and erythema. Fortunately, no signs of irreversible ischemia were noted, and no bowel resection was performed. The defect in the broad ligament was repaired with 2 interrupted figure-of-8 Vicryl sutures. The patient had a return of bowel function the following day and had an otherwise uneventful hospital course.

Discussion
Small bowel obstruction is a common surgical emergency and a frequent cause of hospitalization. Intraperitoneal adhesions cause the majority of small bowel obstructions, followed by complicated hernias and intestinal tumors. 1 Abdominal hernias can be broadly categorized as external hernias and internal hernias. Most abdominal hernias are external hernias, where visceral contents prolapse through a defect in the abdominal or pelvic wall. Internal hernias are defined as loops of the intestine, which prolapse through normal or abnormal defects in the peritoneum or mesentery. Internal hernias are classified by Meyers using historical data into the following groups: (1) paraduodenal (53%), (2) foramen of Winslow (8%), (3) pericecal (13%), (4) intersigmoid (6%), (5) transmesenteric and transmesocolic (8%), and (6) retroanastomotic (5%). 4
Defects in the broad ligament of the uterus make up 4-7% of internal hernias and are acquired or congenital. 3 Trauma resulting from pregnancy, surgery, pelvic inflammatory disease, or spontaneous rupture of cystic structures within broad ligament of the uterus can lead to a defect. 5 Robert Cilley provided classification of broad ligament hernias. Type 1 defects are located caudal to the round ligament. Type 2 defects are located superior to the round ligament. Type 3 defects are located in-between the round ligament and the remainder of the broad ligament, through the meso-ligamentum teres. 6
Clinically, internal hernias can remain asymptomatic or present with nonspecific and intermittent symptoms. These symptoms depend on the location and spontaneous reducibility of the hernia. Symptoms can range from intermittent digestive complaints, epigastric pain, and periumbilical colic to symptoms of partial or complete bowel obstruction. 7 The most common symptoms of small bowel obstruction are acute onset of abdominal pain, tenderness, nausea, vomiting, and abnormal bowel sounds. Untreated strangulated internal hernias have a mortality rate greater than 50%. 8
Internal hernias are rarely diagnosed preoperatively. Most patients present with some degree of small intestinal obstruction or intestinal ischemia. Imaging studies may be unremarkable during asymptomatic intervals due to the spontaneous reducibility of hernias. 9 Studies have shown that a CT scan with contrast has a sensitivity of 94-100% and a specificity of 90-95% in identifying small bowel obstructions. However, CT scans have a lower diagnostic sensitivity and specificity diagnosing internal hernias, for the reasons noted above. Multidetector CT (MDCT) scans are currently being used to detect internal hernias because they create 3-dimensional imaging that can better visualize the defect. 10 This imaging modality has shown to be better at detecting internal hernias than traditional CT scans; however, surgery remains the gold standard for diagnosis and treatment of internal hernias.
At first, our patient presented with mild and nonspecific symptoms. Imaging suggested a ruptured ovarian cyst. Repeated imaging failed to show any signs of an internal hernia or early bowel obstruction. However, the use of oral contrast with the CT scan might have increased the probability of preoperative diagnosis. Thus, laparoscopic evaluation was done which discovered the incarcerated small bowel hernia.
There are no cases reported for multiple internal hernias. The recurrence of internal hernias has rarely been reported. In a case study reported by Zemour et al, 11 an internal hernia through the left broad ligament of the uterus was repaired, and a year later, an internal hernia through the right broad ligament of the uterus occurred.
Conclusion
Broad ligament hernias are a very rare cause of small bowel obstruction. The clinical presentation can vary from being asymptomatic to an acute abdomen due to the intermittent reducibility of the hernia. Preoperative diagnosis is difficult with a standard CT scan. Surgical exploration is required for diagnosis and definitive therapy. Suspected broad ligament hernias require emergent surgical intervention to prevent bowel necrosis and decrease mortality.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval was obtained from the institutional review board.
Informed Consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.