
Abstract
The majority of acute coronary syndromes are caused by coronary artery thrombotic occlusions secondary to atherosclerotic plaque erosion or rupture. Coronary embolism is an important yet forgotten underlying cause of acute coronary syndrome. We present a case of a young patient who presented with ST elevation myocardial infarction suspected to be secondary to coronary embolization originating from a left ventricular thrombus.
Background
A left ventricular thrombus is a serious complication of both ischemic and non-ischemic cardiomyopathy in the presence of severe left ventricular systolic dysfunction. It can occur after an acute myocardial infarction (AMI), specifically in patients with large anterior ST-elevated myocardial infarction (STEMI) complicated with anteroapical aneurysms. Nonetheless, a STEMI associated to a migrating left ventricular thrombus has rarely been reported. 1 We present a case of a young patient who presented with STEMI associated to a left ventricular thrombus without significant coronary artery disease. The aim is to increase the awareness of coronary embolism (CE) as a possible cause of acute coronary syndrome in patients with heart failure with reduced ejection fraction.
Case Presentation
A 33-year-old female presented to the emergency room with acute onset substernal pressure-like chest pain that started 30 minutes prior to her arrival. Chest pain was associated with lightheadedness, nausea, and radiated to the left arm. The patient had a medical history of heart failure with reduced ejection fraction secondary to non-ischemic cardiomyopathy associated with active methamphetamine use, she referred no adherence to home medications (carvedilol, losartan, and furosemide). The patient was hemodynamically stable, heart rate of 87 beats per minute, and blood pressure of 156/123 mmHg. Physical examination demonstrated clear lungs, point of maximal impulse displacement and lower extremity edema. From the initial information, it was suspected that the patient most likely had acute coronary syndrome from vasospasm or plaque rupture. Other considerations included coronary dissection, or an embolic thrombus.
Initial electrocardiogram showed anteroseptal T wave inversions, which are secondary to right bungle branch block, and 40+ms Q wave in V1-V2, which demonstrated anterior ischemia (Figure 1A). Repeat electrocardiogram after 15 minutes showed the same findings as the initial electrocardiogram, in addition to a new ST elevation in V4-V6 (Figure 1B), which was not present in the original or one done 8 weeks before (Supplementary Figure 1). Laboratories revealed brain natriuretic peptide level of 6,492 pg/mL, and troponin T high sensitivity of 51.8 ng/L, within 30 minutes of chest pain onset. Urinary drug sample was negative for amphetamines, barbiturate, benzodiazepine, cannabinoids, cocaine, and opiates. Pont of care cardiac ultrasound showed a severely depressed left ventricular ejection fraction without wall motion abnormality and left ventricular apical thrombus. The patient was diagnosed with STEMI and was taken emergently to the cardiac catheterization laboratory. Thrombotic occlusion of the proximal section of the left anterior descending artery was found (Figure 2, Supplementary Video 1), and successful mechanical aspiration was done (Figure 3, Supplementary Video 2) after 35 minutes of arrival to the hospital. No identifiable coronary artery disease was noted. After reperfusion, troponin was 36 203 ng/L measured 6 hours from arrival to the hospital. A transthoracic echocardiogram was done; it demonstrated a left ventricular ejection fraction lower than 20% and two left ventricular thrombi, one thrombi of 2.6 × 1.3 cm was attached to the anterior wall and the other of 1.2 × 0.89 cm was attached to the inferolateral wall (Figure 4, Supplementary Video 3). Follow-up transesophageal echocardiogram was done 19 days after the STEMI, and it demonstrated persistence of severely depressed ejection fraction (<20%) and of the two left ventricular thrombi (Figure 5, Supplementary Video 4). The patient was discharged after 21 days on guideline-directed medical therapy for heart failure with reduced ejection fraction and anticoagulation for left ventricular thrombi.

(A) Initial electrocardiogram showed anteroseptal T wave inversions, which are secondary to right bungle branch block, and 40+ms Q wave in V1-V2, which demonstrated anterior ischemia (B) Repeat electrocardiogram after 15 minutes showed the same findings as the initial electrocardiogram, in addition to a new ST elevation in V4-V6.

Coronary angiogram showing thrombotic occlusion of the proximal section of the left anterior descending artery.

Coronary angiogram demonstrating successful mechanical aspiration of the thrombotic occlusion found on left anterior descending artery.

Transthoracic echocardiogram demonstrating 2 left ventricular thrombus, one thrombi of 2.6 × 1.3 cm was attached to the anterior wall and the other of 1.2 × 0.89 cm attached to the inferolateral wall.
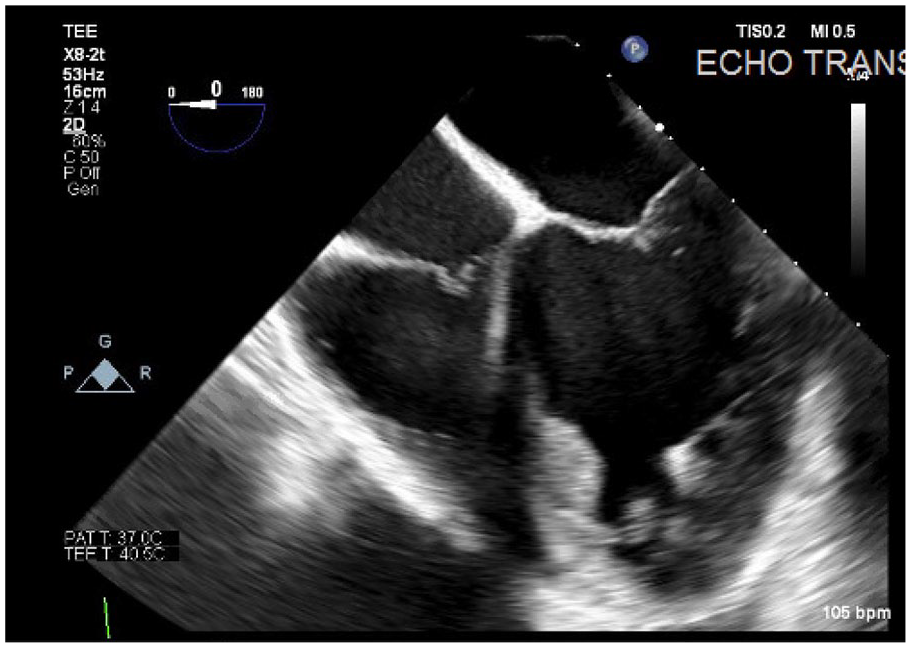
Transesophageal echocardiogram in mid esophageal 4-chamber view demonstrating the persistence of 2 left ventricular thrombus.
Discussion
The majority of AMI are caused by coronary artery thrombotic occlusions secondary to atherosclerotic plaque erosion or rupture. Acute myocardial infarction in the absence of obstructive coronary atherosclerosis is characterized by clinical evidence of myocardial ischemia with normal or near normal coronary arteries on angiography, and the presence of either coronary vasospasm or CE.
Coronary embolisms are an understudied and underdiagnosed cause of AMI,1,2 with previous studies showing that 4% to 7% of AMI patients had non-atherosclerotic coronary arteries based on coronary angiography or autopsy findings.3,4 The most common causes of CE are valvular heart disease, followed by dilated cardiomyopathy, chronic atrial fibrillation, and coronary atherosclerosis.5,6 Classically, the pathophysiologic mechanisms behind CE can be divided into 3 subtypes. First, a paradoxical coronary emboli, which refers to a thrombus that originates from either a deep vein thrombosis or a foreign body in the venous circulation that gains access to the coronary arteries by passing through a patent foramen ovale or atrial septal defect. Second, iatrogenic, this refers to an embolism of surgical material into the coronary arteries that may have occurred at the time of cardiothoracic surgery or during any coronary intervention. Last, and fitting to our case description, is direct CE, that results from a thrombus originating from any of the left cardiac chambers, meaning from the pulmonary veins, endocarditis of the aortic or mitral valve or rarely, cardiac tumors.7,8 As described in our case, CE may also potentially originate from a mural thrombus within the left-sided cardiac chambers.
We hypothesize that the patient’s AMI was secondary to an embolic phenomenon from the left ventricular thrombus, most likely associated with their dilated cardiomyopathy. More specifically, heart failure with reduced ejection fraction offers a suitable terrain for chronic thrombus formation by the 3 mechanisms described by Virchow. 9 First, a hypercoagulable state, heart failure with reduced ejection fraction causes an increase in platelet activation, plasma viscosity, and fibrinogen.9,10 Second, the stasis of blood flow, caused by low cardiac output, dilated cardiac chambers, ventricular aneurysms, and poor contractility. Last, endothelial dysfunction caused by the chronic inflammation secondary to heart failure. Conditions that increase the risk for systemic left ventricular thrombus embolization include severe congestive heart failure, diffuse left ventricular dilation, systolic dysfunction, previous embolization, advanced age, and the presence of a left ventricular protruding or mobile thrombus. 11
There are no current guidelines for the management and diagnosis of acute coronary syndrome secondary to CE, but overall, the presentation of CE is difficult to distinguish from atherosclerotic acute coronary syndrome before the angiographic evidence of coronary artery embolism. Shibata et al proposed criteria for the clinical diagnosis of coronary artery embolism that includes 3 major and 3 minor criteria. Weighted scoring of the criteria is used to differentiate between definitive and probable CE in patients with AMI. There are also no recommendations for management, but thrombus aspiration devices have been shown to be a feasible and effective strategy for the treatment of STEMI patients with coronary angiographic evidence of thrombus.1,12
Conclusion
Coronary embolism can occur in the presence of a left ventricular thrombus and present as a STEMI. Direct thrombus aspiration has been shown to be an effective therapy.
Supplemental Material
sj-png-1-hic-10.1177_23247096221078704 – Supplemental material for Acute Myocardial Infarction Associated With a Mobile Left Ventricular Thrombi
Supplemental material, sj-png-1-hic-10.1177_23247096221078704 for Acute Myocardial Infarction Associated With a Mobile Left Ventricular Thrombi by Gaspar Del Rio-Pertuz, Cristina Morataya, Marina Iskandir and Erwin Argueta-Sosa in Journal of Investigative Medicine High Impact Case Reports
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this article
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.