
Abstract
Following the first report of COVID-19 infection in December 2019 as a respiratory illness, it has proven to be a multisystem disease. There are few reported cases of ischemic colitis with COVID-19 infection in the medical literature to date and we have limited understanding of its pathophysiology. We report 2 cases of ischemic colitis as the only manifestation of COVID-19. In addition, we review the current limited literature regarding COVID-19-associated ischemic colitis.
Introduction
In December 2019, the first case of coronavirus disease 2019 (COVID-19) caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was reported in Wuhan, China. 1 The infection rapidly spread across the world and was declared a pandemic by the World Health Organization (WHO) on March 11, 2020. 2 As of July 19, 2021, the Centers for Disease Control and Prevention (CDC) has reported >600 000 deaths due to COVID-19 infection in the United States. 3 Patients with COVID-19 infection predominantly have respiratory symptoms, but gastrointestinal (GI) symptoms such as nausea, vomiting, abdominal pain, and diarrhea have been reported in up to 60% of these patients.4-12 In this article, we are reporting 2 cases of ischemic colitis as the only manifestation of COVID-19.
Case Description
Case 1
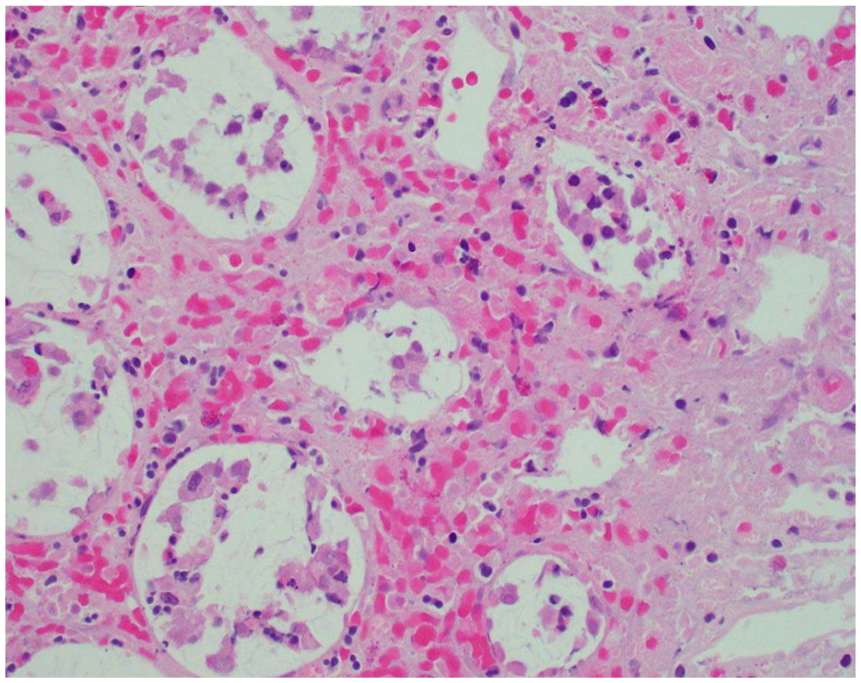
A 62-year-old man with hypertension, well-controlled type 2 diabetes, and gastroesophageal reflux disease presented to the hospital with multiple episodes of hematochezia for 1 day. He was hemodynamically stable and afebrile. He had mild left lower abdominal tenderness. Laboratory data revealed white blood cell count (WBC) 13 300/mm3, hemoglobin 13.2 g/dL, hematocrit 41.2%, and lactic acid 2.1 mmol/L. Stool culture and Clostridium difficile polymerase chain reaction (PCR) testing were negative. The SARS-CoV-2 PCR was positive. Patient did not have any respiratory compromise or hemodynamic instability throughout the hospitalization. Computed tomography (CT) of the abdomen and pelvis with intravenous contrast demonstrated inflammatory changes extending from the rectum to the splenic flexure with patent celiac, superior mesenteric, and inferior mesenteric arteries. Patient underwent flexible sigmoidoscopy that revealed severely edematous, ulcerated, friable mucosa extending 25 cm from the anal verge proximally to the splenic flexure (Figure 1). Colonic biopsies demonstrated small crypts, loss of goblet cells, hyalinization of lamina propria, and mucosal hemorrhage (Figure 2). Based on endoscopic and biopsy findings, he was diagnosed with ischemic colitis. He was given intravenous antibiotics. He was discharged home on day 3 of admission after resolution of leukocytosis and hematochezia.

Flexible sigmoidoscopy—severely edematous, friable, ulcerated descending colon.

Colonic biopsy—loss of goblet cells and hyalinization of lamina propria.
Case 2
A 66-year-old woman with well-controlled type 2 diabetes and hyperlipidemia presented to the hospital with left lower abdominal pain, intermittent hematochezia, and nonbloody emesis for 2 days. She was diagnosed with asymptomatic COVID-19 infection 3 weeks prior to presentation based on positive SARS-CoV-2 PCR. Patient was afebrile and hemodynamically stable. She had mild left lower abdominal tenderness and examination was otherwise normal. Laboratory data revealed hemoglobin 13.9 g/dL, hematocrit 42.8% and lactic acid 2.4 mmol/L, and negative stool culture, C difficile PCR, and SARS-CoV-2 PCR. CT of abdomen and pelvis with intravenous contrast demonstrated inflammatory changes extending from hepatic flexure to sigmoid with patent celiac and mesenteric arteries. Patient underwent flexible sigmoidoscopy and this revealed cratered, clean-based, nonbleeding ulcers with surrounding mucosal erythema, edema, and friable mucosa involving the sigmoid and descending colon (Figure 3). Colonic biopsies demonstrated crypts with loss of goblet cells, hyalinization of lamina propria, and focal hemorrhage (Figure 4). Based on endoscopic and biopsy findings, patient was diagnosed with ischemic colitis. She was administered antibiotics and managed conservatively. She was discharged home on day 4 of admission, after resolution of hematochezia.

Flexible sigmoidoscopy—cratered, clean-based, nonbleeding ulcer in the descending colon.
Colonic biopsy—loss of goblet cells, hyalinization of lamina propria and focal hemorrhage.
Discussion
With the evolution of the COVID-19 pandemic and growing recognition of various manifestations of the disease, there are an increasing number of reports in the medical literature about the rare and lesser understood extrapulmonary manifestations of the disease. One of the less frequently encountered GI manifestations of COVID-19 infection is ischemic colitis.
We searched the medical literature for reports of COVID-19-associated ischemic colitis and identified 15 patients from 9 publications with COVID-19-associated ischemic colitis and their characteristics are summarized in Table 1.13-21 Among the 15 patients, the outcome of 1 patient was not reported, 13 8 patients died, and 6 patients survived the illness. Among the survivors, 2 patients were managed medically19,20 and 4 patients required surgical management. We excluded 4 patients with ischemic enteritis,16,20,22 2 patients with incidentally found pneumatosis intestinalis,23,24 and cross-sectional studies published by Vanella et al and Bhayana et al on mucosal damage (6 patients with left-sided and 3 patients with diffuse ischemic colitis) and abdominal imaging findings in COVID-19 patients, respectively, due to limited availability of patient information (age, sex, preexisting condition[s], GI symptom[s], vasopressor requirement, presence of intravascular thrombus, treatment, and outcomes).25,26
Summary of COVID-19-Associated Ischemic Colitis Cases Reported in the Medical Literature.

Abbreviations: GI, gastrointestinal; NA, not available; CT, computed tomography; HTN, hypertension; DM, diabetes; PI, pneumatics intestinalis; COPD, chronic obstructive pulmonary disease; ESRD, end-stage renal disease; GERD, gastroesophageal reflux disease.
Both cases 1 and 2 reported by us do not have any risk factors for intestinal ischemia but had clinical features consistent with ischemic colitis. Neither of the 2 patients had hemodynamic instability or imaging evidence of intravascular thrombosis. Case 1 had positive COVID-19 PCR during the admission, whereas case 2 had recent asymptomatic COVID-19 infection preceding the admission for ischemic colitis. There is no definitive proof of causation; however, given the diagnosis of ischemic colitis during/recent infection with COVID-19, we diagnosed both patients with COVID-19-associated ischemic colitis.
Human-to-human transmission of COVID-19 infection is mainly through respiratory droplets. The hallmark of COVID-19 infection is severe respiratory illness; however, other organs, including GI tract, are also affected. Angiotensin-converting enzyme 2 (ACE2) receptor that plays a key role in the viral entry is expressed in the gastric, duodenal, and rectal epithelia. 27 The most common GI symptoms are diarrhea (34%), nausea (27%), vomiting (16%), and abdominal pain (11%). 28 In a retrospective study conducted by Laszkowska et al, patients with GI symptoms had an indolent course with lower rates of intubation and death. 29
In patients with COVID-19, coagulopathy is suspected to be related to the high inflammatory state and is associated with increased mortality and morbidity.30,31 Most common thromboembolic complications are pulmonary embolism, deep vein thrombosis, and, rarely, mesenteric ischemia. Acute mesenteric ischemia is associated is very high morbidity and mortality. Following prompt diagnosis, patients with mesenteric ischemia should be treated with fluid resuscitation and surgical resection of necrotic bowel with restoration of blood flow to the ischemic intestine.14,15
The reduced blood flow state in colonic ischemia (CI) is insufficient to maintain cellular metabolic function. 32 The CI is the cause of 9% to 24% of all hospitalizations for acute lower GI bleeding.33-35 There is higher incidence of CI after age 49 and has a female predilection.36,37 CI results from alterations in the systemic circulation or from anatomic or functional changes in the mesenteric vasculature. 32 Typical clinical presentation is sudden onset abdominal pain, urge to defecate, and rectal bleeding within 24 hours. 37 These symptoms resolve in 2 to 3 days and colon usually heals in 1 to 2 weeks. 32 Left colon is most commonly affected and includes the watershed areas—splenic flexure and sigmoid colon. Early colonoscopy (less than 48 hours) with minimum insufflation is recommended in suspected cases to confirm the diagnosis.38-40
The pathophysiological mechanism in COVID-19 resulting in ischemic colitis is poorly understood. None of the patients with COVID-19 ischemic colitis had mesenteric arterial occlusion detectable in imaging, but 2 patients had microthrombi in pathology specimen.14,21 Patients with severe COVID-19 infection have nonocclusive CI due to intense vasoconstriction and decreased mesenteric blood flow secondary to hemodynamic compromise and use of inotropic agents. 14
In cases 1 and 2, there was no hemodynamic instability or radiographic evidence of thrombosis. We suspect that our patients developed ischemic colitis, most likely due to SARS-CoV-2-induced endotheliitis or direct bowel damage due to expression of ACE-2. Given the limited information available on COVID-19-associated ischemic colitis, further research is needed to better understand this condition.
Footnotes
Author Contributions
Each author contributed substantially to the work, worked on the drafting of the manuscript, and was involved in its final approval.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patients for their anonymized information to be published in this article.