
Abstract
Hypotension is the main finding in patients admitted to an intensive care unit (ICU) with the diagnosis of septic shock and it is related to worse outcomes. In these patients, several underlying causes of hypotension may co-exist, including vasoplegia, hypovolemia, drug-mediated venodilation, or myocardial dysfunction. Nowadays, echocardiography has been positioned as an essential tool in any ICU set to assess fluid status, ventricular ejection fraction, or any other myocardial complications. The high sympathetic tone in severely ill patients, in addition to high doses of adrenergic drugs often needed, may provoke a hypercontractile cardiac state. In the basis of our experience, we present a case of a patient with refractory septic shock and severe hemodynamic collapse, refractory to vasopressors with concomitant respiratory deterioration due to dynamic left ventricular outflow tract obstruction (LVOTO). Transesophageal echocardiography (TOE) was used to assess hemodynamic status and to guide treatment. A critical response to intravenous β-blockers was seen, with a dramatic decrease in vasopressor dosage and respiratory support.
Case Presentation
A 40-year-old man (height 175 cm; weight 90 kg) was admitted to tertiary hospital’s intensive care unit (ICU) due to acute ischemic stroke. He had prior history of type 1 diabetes mellitus and kidney transplant due to diabetic kidney disease 10 years ago. He required mechanical ventilation (MV) because of agitation during percutaneous thrombectomy. On second day of ICU, he experienced rapid deterioration from an aspiration pneumonia that evolved into septic shock. Increasing vasopressors requirements and respiratory support were needed.
A transthoracic echocardiography was performed due to new onset heart systolic murmur. Previous echocardiography 5 months ago had revealed a hypertrophic left ventricle with no other pathological conditions. The main finding was a dynamic left ventricular outflow tract obstruction (LVOTO), with severe mitral regurgitation (MR) due to systolic anterior motion (SAM) of the mitral valve. At this point, the patient had a mean arterial pressure (MAP) of 65 mmHg with 1.8 μg/kg/min of norepinephrine and was non-fluid responsive. He was on control assisted ventilation with an inspired fraction of O2 (FiO2) = 100% and a positive end-expiratory pressure (PEEP) of 15 mm Hg on pressure ventilation mode. As he had a suboptimal transthoracic window, transesophageal echocardiography (TOE) was done to better assess LVOTO, SAM, and MR. A hypertrophic septum (17 mm) with dynamic LVOTO due to hypercontractile status was confirmed, with a maximum intraventricular gradient of 165 mm Hg. Severe eccentric MR directed posteriorly and laterally, caused by SAM of anterior and posterior leaflets of the mitral valve, was also observed (Figure 1A and B; Figure 2A and B).
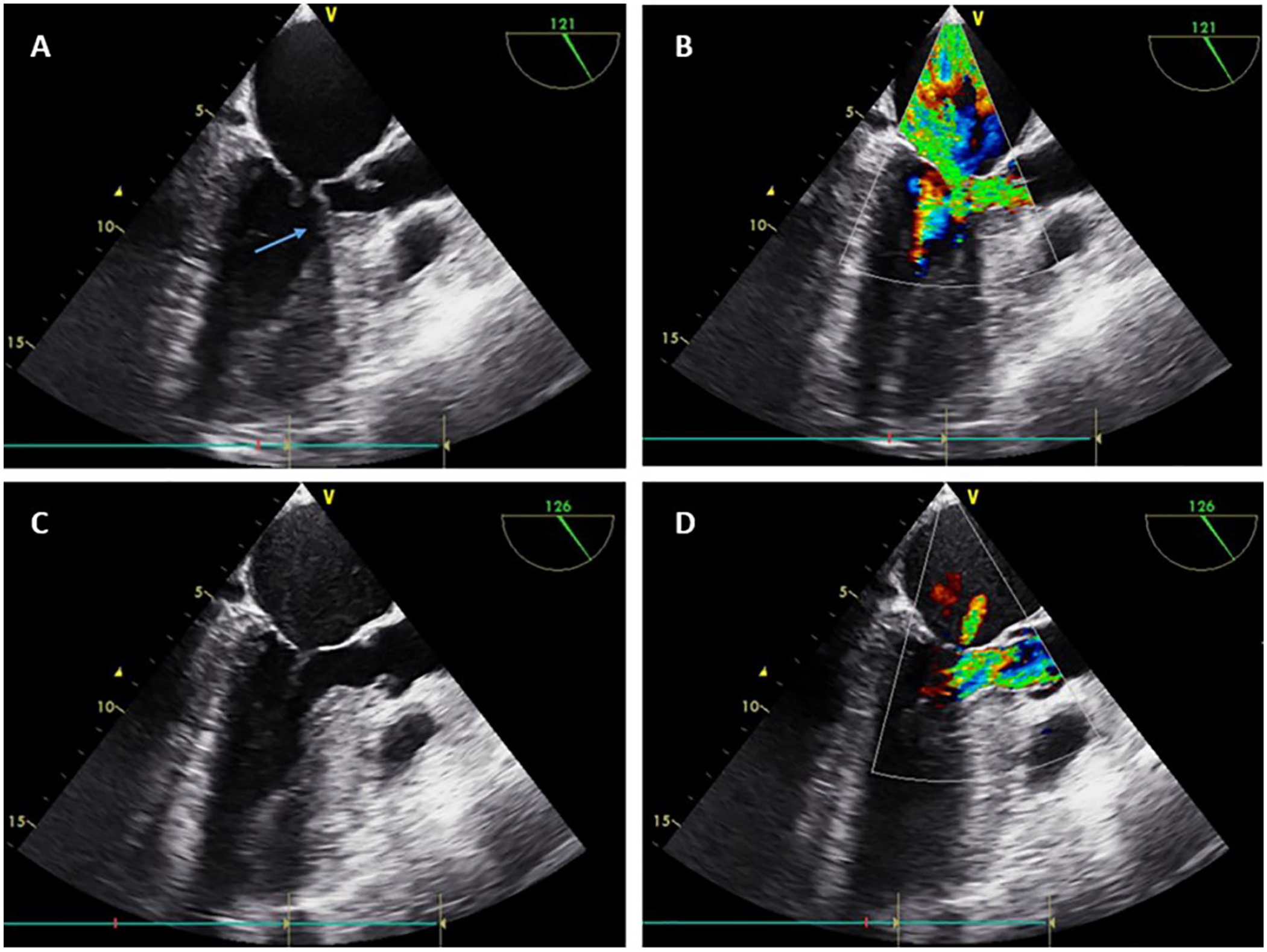
Three-chambers view: (A) Pre-β-blocker administration without color doppler. (B) Pre-β-blocker administration with color doppler. (C) Post-β-blocker administration without color doppler. (D) Post-β-blocker administration with color doppler. Arrow: systolic anterior motion of mitral leaflet. In pre-β-blocker echocardiography, severe eccentric mitral regurgitation can be seen due to systolic anterior motion of the mitral valve.

Four-chambers view: (A) Pre-β-blocker administration without color doppler. (B) Pre-β-blocker administration with color doppler. (C) Post-β-blocker administration without color doppler. (D) Post-β-blocker administration with color doppler. Arrow: systolic anterior motion of mitral leaflet. In pre-β-blocker echocardiography, severe eccentric mitral regurgitation can be seen due to systolic anterior motion of the mitral valve.
We first tried to diminish pressure gradient by progressive decreasing PEEP from 15 to 5 cm H2O to improve cardiac preload, but it was not responsive. In fact, a deterioration in oxygen saturation made us stop the maneuver. Pulmonary congestion and previous volume unresponsiveness anticipated that fluid bolus would not be effective, so it was avoided at this moment. Then, we administered an esmolol bolus (500 μg/kg, 4500 μg) to evaluate the pressure gradient after a decrease in cardiac inotropism. We carefully monitored hemodynamic, respiratory, and echocardiographic response. An evident improvement in hemodynamic state within the first minutes was observed, with an increase in MAP from 65 to 85 mm Hg which enabled us to reduce norepinephrine dose from 1.8 to 0.9 μg/kg/min. Oxygen needs maintained equal initially. The TOE recorded 2 minutes after the esmolol administration showed a critical reduction in intraventricular gradient and in SAM of the mitral valve (Figure 1C and D; Figure 2C and D), which in turn resulted in MR improvement.
Having proved the benefit of β-blockade on this patient, an esmolol perfusion was started with a starting dose of 50 μg/kg/min. The TOE-based guidance was used to titrate esmolol dose to the minimum effective dose while also maintaining adequate blood pressure. In the following hours, norepinephrine was reduced to 0.4 μg/kg/min (for an MAP of 65 mm Hg) and FiO2 was also reduced from 100% to 50%. Venous oxygen saturation augmented and lactate levels decreased. Despite achieving such an improvement in hemodynamic and respiratory state, 12 days after ICU admission the patient experienced hemorrhagic transformation of his previous stroke and died due to neurological deterioration. The chronology and hemodynamic results of the intervention are summarized in Figure 3.

Chronology and results.
Discussion
Dynamic LVOT is classically described in asymmetric hypertrophic cardiomyopathy, 1 but it has been also described in a number of different cardiac conditions such as myocardial infarction, 2 following mitral valvuloplasty, or during dobutamine stress tests. 3 However, it is not only related to heart conditions, as it can also be found in normal heart during hypercontractile state and hypovolemia.4,5 Both conditions are common among patients admitted to ICU with septic shock. On literature, a few studies analyzing the incidence of dynamic LVOTO in patients with septic shock can be found. The incidence is probably higher than expected, ranging from 20% to 30%.6,7 Dynamic LVOTO is related to higher mortality 8 and fluid responsiveness. Hypovolemia is 1 of the main etiological factors, that is, why dynamic LVOTO usually is fluid-responsive. In literature, most of the cases reported are treated just with fluids, and β-blockers are rarely evaluated. However, understanding the physiological mechanism is essential to adequately treat unusual presentations. In non-fluid responsive patients, reducing the PEEP may help to improve preload and diminish dynamic LVOTO. Treatment with β-blockers in this scenario must be really well pondered and it should be guided by echocardiography and perfusion measurements. If vasopressors are needed in this scenario, phenylephrine has been used with good results, due to low inotropic properties. 9
With this rare case presentation, we want to highlight some points. First of all, dynamic LVOTO is more common among patients with septic shock that we would believe otherwise, and we must keep that in mind when treating hypotensive patients, as it usually improves with fluid resuscitation. Second, we must realize that dynamic LVOTO worsens septic shock prognosis and echocardiography is a resourceful tool for diagnosis and treatment of critical patients. Finally, a better comprehension of the underlying disease pathophysiology may help in the treatment of rare presentations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Instituto de Ciencias del Corazón (ICICOR).
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.