
Abstract
A 49-year-old man with no significant past medical history received dexamethasone as part of his treatment for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection. Less than 3 weeks later, the patient developed acute respiratory distress syndrome. Radiological and serological testing led to a diagnosis of acute hypoxic miliary coccidioidomycosis. A 52-year-old man with a past medical history of chronic kidney disease (CKD) was treated with prednisone for focal segmental glomerulosclerosis (FSGS). Within 2 weeks, this patient developed bilateral lower extremity weakness. Radiology, serology, and lumbar puncture proved a diagnosis of reactivated coccidioidomycosis with miliary pattern and coccidioidomycosis meningoencephalitis with arachnoiditis. Whether treatment with glucocorticoids caused reactivation of coccidioidomycosis is discussed in this case series.
Keywords
Introduction
Glucocorticoids have been historically used for immune system modulation. Nonetheless, cell-mediated immunity is required for the control of coccidioidomycosis (CM) infection. Patients undergoing immunosuppressive therapy have a high risk of severe primary pulmonary infection, disseminated infection, or reactivated infection. In regions endemic to CM, there are no established guidelines for CM screening prior to initiating immunosuppressive therapy.
Methods
Approval was obtained from the Institutional Review Board of Kern Medical. A retrospective review of the patient’s record was performed. Literature search was conducted on PubMed, Google Scholar, and UpToDate. The following search terms were applied: coccidioidomycosis, glucocorticoid, immunosuppression, miliary coccidioidomycosis, reactivation of coccidioidomycosis.
Case Presentation
Patient 1
This patient is a 49-year-old Latinx male field worker with tobacco and alcohol abuse. He was in his usual state of health until he developed a nonproductive cough. He tested positive for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) by Abbott COVID-19 testing at an urgent care facility. He presented to our institution 1 day later. Chest x-ray (CXR) revealed bibasilar infiltrates (Figure 1). The patient was deemed stable, with SpO2 of 96%, and was discharged on supportive management.
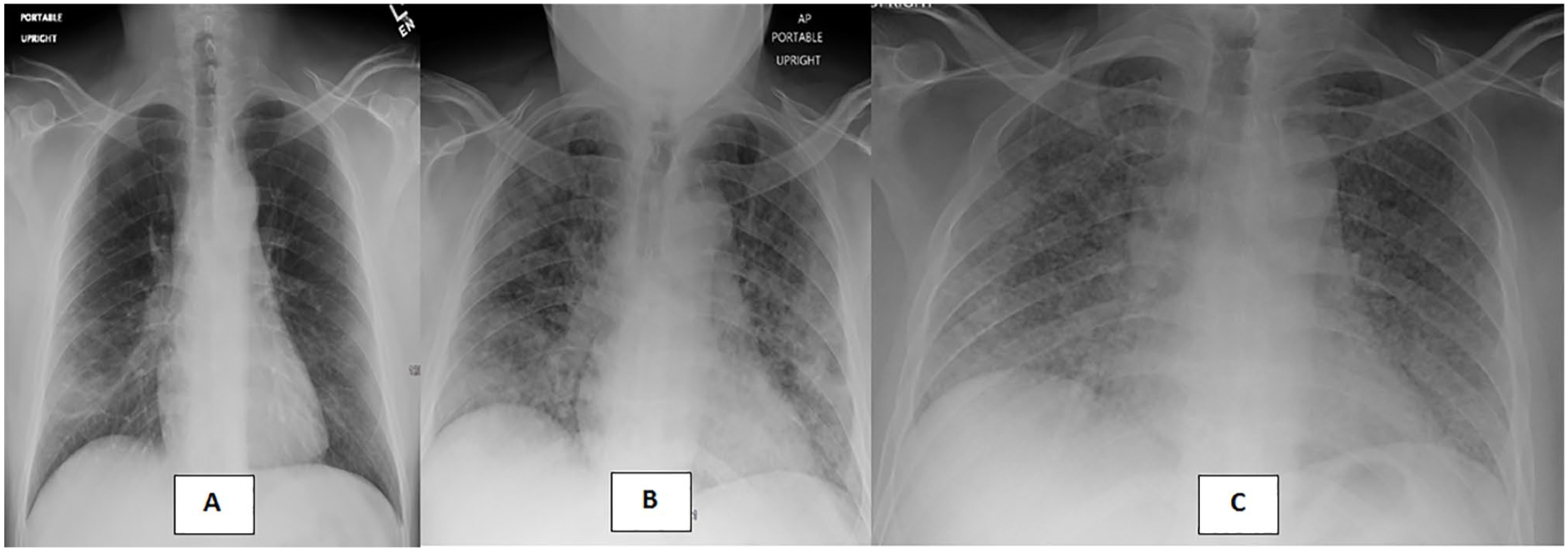
(A) First CXR (hospital visit 1) revealing segmental right mid to lower lung zone and subsegmental left mid to lower lung zone airspace disease; (B) second CXR (hospital visit 2) revealing diffuse infiltrates, consistent with viral infection; and (C) third CXR (hospital visit 3) day 28, demonstrating bilateral miliary lung nodules.
The patient re-presented 6 days later with increased cough with shortness of breath and subjective fever. Upon admission, his vital signs showed a heart rate of 112 beats per minute (bpm), respiratory rate of 36 breaths per minute, and SpO2 of 90%. The CXR demonstrated increased infiltrates (Figure 1). He was treated with nasal oxygen, convalescent plasma, and dexamethasone 6 mg daily for 10 days. His oxygenation improved, and he was discharged on 2 L of nasal home oxygen on hospital day 5 to finish the dexamethasone course at home. Serum CM serology was ordered during this admission; however, results were obtained after discharge (Table 1). One week later, this serology was repeated in the clinic (Table 1).
Patient 1 Results.
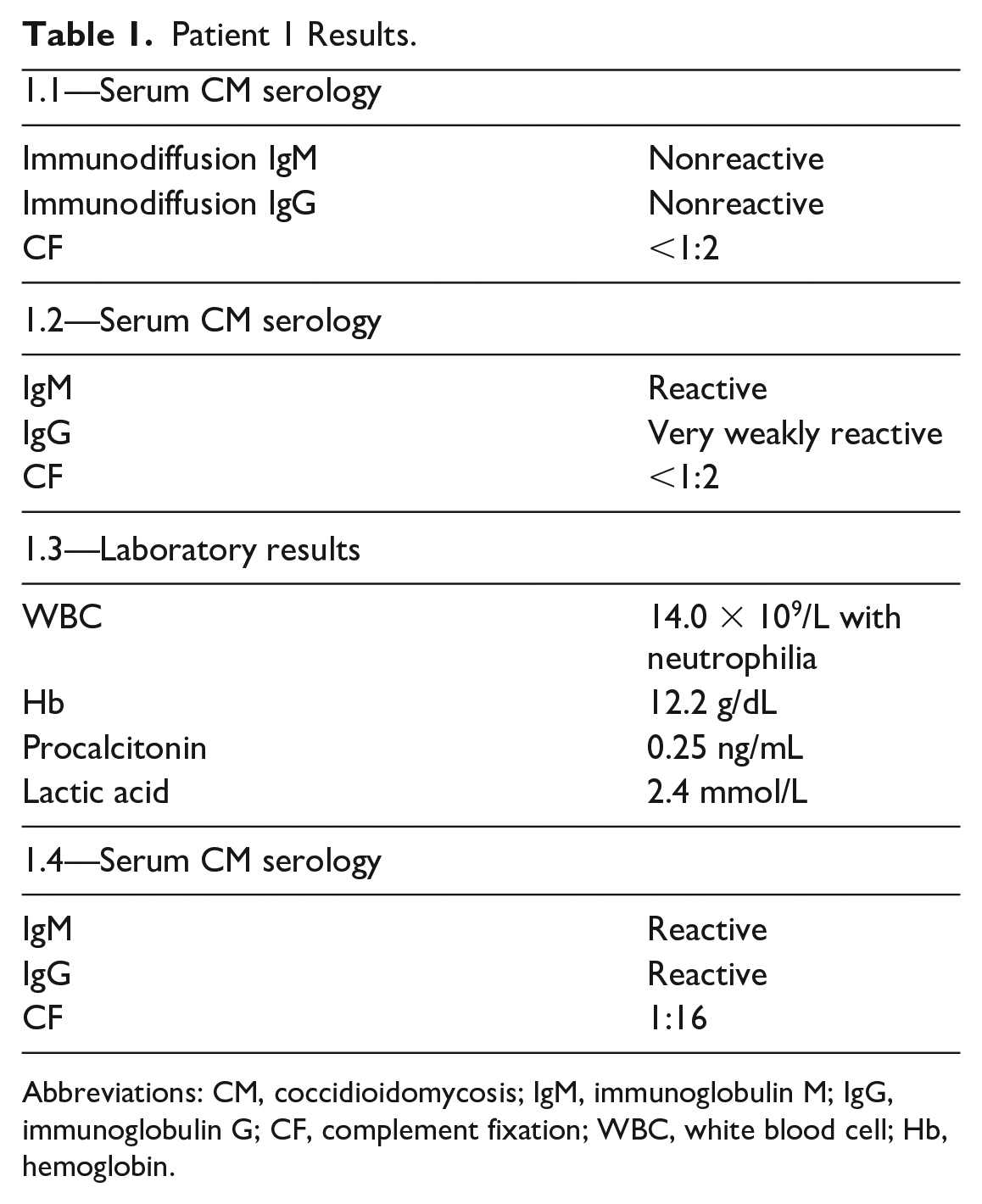
Abbreviations: CM, coccidioidomycosis; IgM, immunoglobulin M; IgG, immunoglobulin G; CF, complement fixation; WBC, white blood cell; Hb, hemoglobin.
The patient completed the dexamethasone and improved temporarily. However, 18 days after discharge, he re-presented with 2 days of increasing cough, shortness of breath, subjective fever, and night sweats. Vital signs revealed heart rate of 135 bpm, respiratory rate of 24 breaths per minute, and SpO2 of 89% on 2 L of oxygen via nasal cannula. Physical examination demonstrated labored breathing, decreased bronchovesicular breath sounds in the right lower lobe, and wheezes and crackles in the left lung base. Integumentary examination revealed 6 new 4 mm lesions, including 2 erythematous macules, 2 verrucous papules, and 2 nodules with eschars (Figure 2). Skin cultures of these lesions revealed rare Coccidioides immitis. Laboratory results are demonstrated in Table 1.

Integumentary examination: (A) Papule with eschar, (B) 2 erythematous macules, (C) papule with eschar, and (D) 2 verrucous papules.
The CXR revealed bilateral miliary nodules (Figure 1). Computed tomography (CT) of the chest with contrast confirmed this and demonstrated right middle lobe consolidation with central cavitation (Figure 3). Serum CM serology was ordered (Table 1), and sputum culture grew C immitis.

Chest CT with contrast (axial view) (hospital visit 3) revealing diffuse bilateral miliary reticulonodular opacities and right middle lobe consolidation with central cavitation.
The patient was diagnosed with acute hypoxic miliary CM. Treatment was initiated with amphotericin B 5 mg/kg intravenous (IV) daily and IV methylprednisolone tapered over 21 days, adopted from adjunctive corticosteroid treatment of pneumocystis in our institution for CM patients with hypoxemia. Despite a turbulent hospital course, vigorous treatment resulted in a hospital discharge with continued outpatient care for disseminated CM.
Patient 2
The second patient is a 52-year-old Latinx man with diabetes mellitus type II. He was found to have chronic kidney disease (CKD). He underwent kidney biopsy that showed focal segmental glomerulosclerosis (FSGS) and he was started on prednisone 60 mg daily by his nephrologist. Ten days after initiation of treatment, the patient presented to our institution with progressive bilateral lower extremity weakness. Vital signs were temperature of 36.5°C, blood pressure of 132/76 mm Hg, heart rate of 84 bpm, respiratory rate of 16 breaths per minute, and SpO2 of 97% on room air. Physical examination revealed paraplegia and the patient was admitted. Laboratory results are demonstrated in Table 2. Magnetic resonance imaging (MRI) of the axial skeleton without contrast revealed leptomeningeal enhancement of the entire spine.
Patient 2 Results.

Abbreviations: BUN, blood urea nitrogen; CSF, cerebrospinal fluid; WBC, white blood cell; CM, coccidioidomycosis; IgM, immunoglobulin M; IgG, immunoglobulin G; CF, complement fixation.
The patient developed fever to 39°C, nuchal rigidity, and disorientation. The MRI of the brain without contrast demonstrated punctate foci in the bilateral mesial temporal lobes, peripheral right cerebellar hemisphere, and left midbrain cerebral peduncle. Subsequent lumbar puncture was performed (Table 2). Cerebrospinal fluid fungal culture grew C immitis.
Pulmonary imaging was compared with prior studies (Figures 4 and 5). The CXR demonstrated new diffuse miliary nodular densities throughout both lungs (Figure 4). The CT demonstrated bilateral miliary nodules (Figure 5). Serum CM was obtained (Table 2).

(A) CXR 4 months prior to presentation revealing slight basilar atelectasis and (B) CXR upon presentation demonstrating diffuse miliary nodular densities throughout both lungs with superimposed subsegmental linear airspace disease in the left lower lung zone.

(A) Chest CT 4 months prior to presentation demonstrating normal lung parenchyma however a cavitary mass as shown in the left lower lobe and (B) chest CT upon presentation demonstrating bilateral miliary lung nodules.
The patient was diagnosed with CM with miliary pattern and CM meningoencephalitis with arachnoiditis, resulting in his bilateral lower extremity weakness. Empiric treatment was initiated with fluconazole 1000 mg IV daily, amphotericin B 5 mg/kg IV daily, along with dexamethasone for 15 days (20 mg daily for days 1-7, 16 mg daily for days 8-9, 12 mg daily for days 10-11, 8 mg daily for days 12-13, and 4 mg daily for days 14-15). The patient was receiving intermittent hemodialysis for acute CKD. His hospital course became complicated with an episode of sepsis and admission to the intensive care unit. After a 42-day tempestuous hospital course, the patient was unable to be weaned off mechanical ventilation and he was placed on comfort care and passed away.
Discussion
The CM causes asymptomatic disease in most patients, yet it often leaves behind an immunological footprint. 1 With advancement in biomedical technologies, serological testing has allowed for CM detection in nearly all affected individuals. 1 The CM serology is a staple laboratory order for symptomatic disease in endemic areas; yet, asymptomatic patients are rarely screened. A challenge arises: when should asymptomatic screening be a requisite.
Both patients in this case series had an unknown history of CM infection. Each of these individuals was placed on a glucocorticoid regimen for their respective comorbid diseases, SARS-CoV-2, and FSGS. The first patient received dexamethasone 6 mg daily for 10 days, per COVID-19 management described by the RECOVERY trial. 2 The second patient was started on prednisone 1 mg/kg daily, receiving the maximum dose of 60 mg daily for FSGS.3-5 A robust type 2 immunity and a weak type 1 immunity response facilitate the spread of disseminated disease; this was proven by a case of disseminated CM that was treated successfully by administration of interferon-γ (IFN-γ) to the patient. T helper 1 (Th1) cells produce IFN-γ that facilitates macrophagic engulfing of CM. There is a direct correlation between levels of IFN-γ to disease spread of CM. 6 On the other side, interleukin 4 (Il-4) plays a major culprit in the dissemination of CM as it directly suppresses Th1 cell development leading to decreased functioning of neutrophils and macrophages that are responsible for fungal elimination. 6 This balance can be skewed further with the administration of glucocorticoids that have been studied and proven to decrease the production of IFN-γ and Th1 cells and augment the production of IL-4 and T helper 2 (Th2) cells. 7
Pathogen-Associated Molecular Pattern Detection
The initial immune response to CM infection begins with the innate immune system. Pattern recognition receptors (PRRs) detect the pathogen-associated molecular patterns (PAMPs). 8 Of the multiple subsets of PRRs, 2 have been identified to play a role in control of CM infection: toll-like receptors (TLRs) and C-type lectin receptors (CLRs). As these PRRs recognize components of the spherule wall, they activate the innate immune system response and the subsequent adaptive immune system response. 9 This begins with the complement system, which produces chemotactic factors that recruit macrophages and neutrophils. 10
Despite favorable application in multiple disease processes, glucocorticoids are known to cause immunosuppression through pleiotropic means. 11 Glucocorticoids act on neutrophils, preventing adhesion and favoring detachment, resulting in increased circulating neutrophils. Studies have shown glucocorticoid suppression of chemotaxis on supra-pharmacological concentrations; however, some studies show contradictory results. 12
Innate Immunity
Neutrophils play a vital role in the phagocytosis of arthroconidia, endospores, and immature spherules, yet they fail to engulf mature spherules, given their large size. 13 Macrophages have also been found to be crucial in pathogen clearance. Once macrophages have been recruited to inflammatory sites, they develop into their subsets for specific microbial modulation. Both IFN-γ and IL-4 allow for speciation into M2 and M2 macrophage subsets. 14 Both IFN-γ and tumor necrosis factor α (TNF-α) are essential for phagolysosome formation; yet in the absence of these factors, endospores can inhibit phagolysosome formation. 15 Phagocytic cells destroy engulfed fungal components via respiratory burst. 16
Glucocorticoids have inhibitory effects on phagocytosis and intracellular pathogen destruction via modulation of respiratory burst. 17 Steroid administration is associated with reduced mRNA expression of various cytokines, among which is TNF-α. 18
Adaptive Immunity
Adaptive immunity contributes to CM defense. CD4+ T helper cell differentiation allows specified cytokine production. Differentiation to Th1 (under interleukin 12 [IL-12] influence) and T helper 17 (Th17) (under interleukin 6 [IL-6] and transforming growth factor β [TGF-β] influence) has been proven to reduce fungal burden. 19 Nonetheless, studies have shown that mice with low Th17 levels or decreased interleukin 17 (IL-17) immunity have higher CM susceptibility.8,20 Additional cytokines also play a role in CM infection control (ie, IL-12, interleukin 22 [IL-22]) and more are continually discovered with ever-increasing research. 8
Although adaptive immunity is crucial for microbial defense, excess or abnormal activation causes inflammatory conditions (Table 1). Glucocorticoids have been used in the management of these disease settings, which has led to a deep understanding of their effects on the adaptive immune system. 21 T helper 1 cells have been shown to be sensitive to inhibition by glucocorticoids, whereas Th17 cells have shown inconclusive sensitivity to glucocorticoid suppression. 21
It has been long known that glucocorticoids cause a high-risk state for fungal infections. Nonetheless, a close review of the immune system response to CM infection and to glucocorticoid administration reveals the extensive overlap of their respective biochemical effects (Table 3). Yet, no definite measures are in place for CM screening prior to glucocorticoid administration in endemic regions.
Immune response to coccidioidomycosis and glucocorticoid effects on immunity.

Abbreviations: TNF-α, tumor necrosis factor α; IFN-γ, interferon-γ ; Th1, T helper 1; Th17, T helper 17.
Conclusion
Glucocorticoids are a double-edged sword. In high doses, they demonstrate a broad spectrum of immune suppression. This may advantage patients with an excessive immune response. Moreover, they may contribute to the treatment of acute, severe CM. However, immune suppression unopposed by antifungal therapy may lead to severe reactivation of CM. In our patients, glucocorticoids were part of the treatment for SARS-CoV-2 and FSGS. However, lack of CM screening led to acute hypoxic miliary CM in one patient and miliary CM with meningoencephalitis and arachnoiditis in the other. Our hypothesis is that immunosuppression without antifungal therapy led to reactivation of underdiagnosed CM in these 2 cases. We suggest screening for CM prior to immunosuppressive treatment in regions endemic regions to CM.
Footnotes
Acknowledgements
The case report was presented as a poster presentation at the San Joaquin Valley Research Forum in Bakersfield, California, on June 4, 2021. This case report was also presented as an oral presentation at the Coccidioidomycosis Study Group Conference in Tucson, Arizona, on April 16, 2021.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval to report this case was obtained from the Kern Medical Institutional Review Board (Approval ID: 21008).
Informed Consent
Informed consent for patients’ information to be published in this article was obtained.