
Abstract
Lemierre syndrome was first documented in the literature in 1936, and is defined as septic thrombophlebitis of the internal jugular vein. It is typically a result of oropharyngeal infection causing local soft tissue inflammation, which spreads to vasculature, and promotes formation of septic thrombi within the lumen, persistent bacteremia, and septic emboli. We present the case of a 24-year-old incarcerated man, who presented with leukocytosis and a right-sided tender, swollen neck after undergoing left mandibular molar extraction for an infected tooth. Computed tomography revealed a persistent thrombus in the transverse and sigmoid sinuses bilaterally, extending downwards, into the upper jugular veins. He was started on empiric intravenous vancomycin, zosyn, and heparin, but subsequently demonstrated heparin resistance, and was thus anticoagulated with a lovenox bridge to warfarin. Throughout his hospital course, hemocultures demonstrated no growth, so antibiotic treatment was deescalated to oral metronidazole and ceftriaxone. On discharge, the patient was transitioned to oral amoxicillin and metronidazole for an additional 4 weeks with continuation of anticoagulation with warfarin for a total of 3 to 6 months. This case report details a unique presentation of Lemierre syndrome with bilateral transverse sinus, sigmoid sinus, and internal jugular vein thrombosis that was presumably secondary to an odontogenic infectious focus.
Introduction
Lemierre syndrome (LS), also commonly referred to as human necrobacillosis and postanginal septicemia, 1 was first discovered in 1936. 2 LS is characterized by an oropharyngeal infection, with resulting metastatic septic emboli and internal jugular vein thrombosis. 3 The organism most commonly implicated (81% of cases) in the infection is the gram-negative oral flora anaerobe Fusobacterium necrophorum. 4 Symptoms typically correlate with the primary infection site and generally include local pain and sore throat (present in more than 80% of cases), fever, trismus, nausea, and odynophagia. 5
The highest incidence of LS is found in young, healthy adults, with 70% of cases occurring in patients aged between 16 and 25 years. 5 However, since the advent of antibiotics, LS has been commonly referred to as “the forgotten disease.” 6 Infection most commonly originates from the head and neck, with greater than 85% of cases being secondary to tonsillitis or pharyngitis. 1 Less commonly, odontogenic infections and mastoiditis account for 2% and 3% of LS cases, respectively. 5 The original publication on LS in 1936 described 18 out of 20 cases resulting in death. 5 With use of modern day antibiotics, mortality rates range from 4% to 12%. 5 The purpose of this case report is to document a rare and unique presentation of LS that presumably resulted secondary to an infectious odontogenic source.
Case
A 24-year-old incarcerated man with a history of pyruvate kinase deficiency requiring splenectomy presented to the emergency department with complaints of left lower tooth pain, right-sided neck pain, and swelling. He was diagnosed with odontogenic infection with reactive lymphadenopathy and discharged on clindamycin for 7 days. He then underwent a left-sided mandibular molar extraction and was given an additional 3 days of antibiotics. He returned to the emergency department 1 day post tooth extraction complaining of headache, right-sided neck pain, and swelling that was exacerbated with chewing, as well as a slightly muffled voice. In addition, he had tenderness to palpation of the right sternocleidomastoid muscle, which was erythematous and warm to touch. He remained afebrile throughout his hospital course, but had significant leukocytosis of 22.8 × 109/L on admission that peaked at 36.0 × 109/L. Patient also had significant thrombocytosis with an elevation as high as 1.29 × 1010/L.
Physical examination findings were significant for a left mandibular molar tender to palpation without surrounding gingival erythema, in duration, or fluctuance, right tonsillar grade 3 enlargement, without erythema or exudates, and left tonsillar grade 2 enlargement without erythema or exudates. Of note, the sublingual and submental regions were soft, without induration, and bilateral tympanic membranes were without air-fluid levels, bulging membranes, or erythema. He exhibited a slightly muffled voice due to the swelling. A week into his hospital stay, he began complaining of new-onset mild pain behind his right eye on extreme rightward gaze. Throughout the hospital course, the patient did not exhibit signs of respiratory distress such as tripoding or intercostal retractions, or signs of meningeal irritation.
A computed tomography (CT) scan of the neck/soft tissue with contrast demonstrated soft tissue thickening surrounding the thrombosed right jugular vein. Right-sided cervical adenopathy in both the suprahyoid and infrahyoid neck was present. There was no evidence of any frank abscesses. Notably, there was thrombosis extending from the right sigmoid sinus down into the right jugular vein in the mid neck. CT angiogram of the brain and neck with contrast demonstrated partial obstruction of the right transverse sinus with complete obstruction of the right sigmoid sinus and jugular vein (Figure 1). There was nonvisualization of the entire right jugular vein (Figure 1). Magnetic resonance imaging of the brain without and with contrast as well as magnetic resonance venography of the head with contrast demonstrated some dilatation of the right superior ophthalmic vein with diminished flow in the cavernous sinuses bilaterally. There was prominent collateral venous flow extending from the orbital regions down to the facial veins bilaterally. There was significant inflammatory signal in the right mastoid and middle ear. The most diagnostically significant finding was persistent thrombosis in the transverse and sigmoid sinuses bilaterally, extending down to the upper jugular veins (Figures 2 and 3).

Computed tomography angiography of the brain and neck with contrast demonstrated complete obstruction and nonvisualization of the entire right jugular vein. Yellow arrows indicate location of right and left jugular veins.
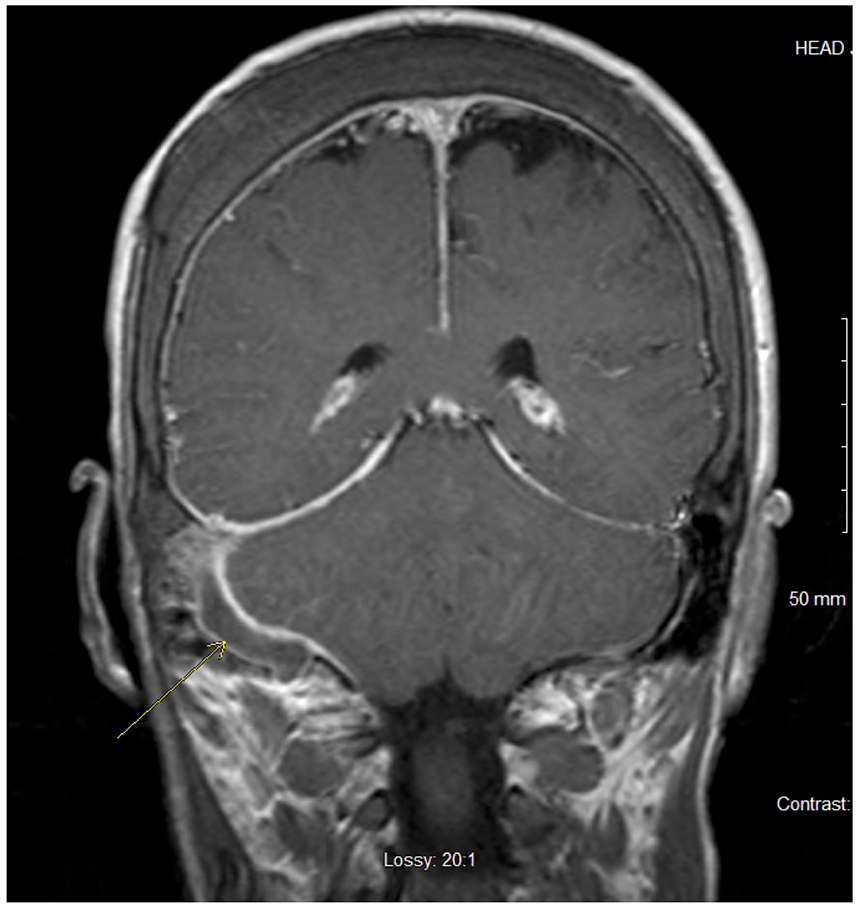
Magnetic resonance imaging of the brain with contrast: T1- and T2-weighted images demonstrate occlusion of the right sigmoid sinus indicated by yellow arrow.

Magnetic resonance imaging of the brain without contrast: T1- and T2-weighted images demonstrate occlusion of the right sigmoid sinus indicated by yellow arrow.
On admission, the patient was started on heparin drip of 18 units/kg/h. As partial thromboplastin time (PTT) level remained subtherapeutic, heparin drip was incrementally increased over the subsequent 4 days. On hospital day 4, the patient was receiving 38 units/kg/h, totaling 72 960 U 24 h−1, and multiple heparin boluses but PTT continued to be subtherapeutic. At this point, the patient was diagnosed with heparin resistance, which is defined as requiring 35 000 U 24 h−1 to prolong the PTT, 7 and the patient was switched to warfarin, bridged with lovenox. The patient reached the goal international normalized ratio of 2 to 3 after 7 days. He was discharged on warfarin 5 mg with a goal of 3 to 6 months of anticoagulation.
To address the leukocytosis at the time of admission, the patient was started on empiric IV vancomycin and zosyn. Blood cultures were negative for any growth, but the patient was empirically treated for F necrophorum given concern for LS. While in the hospital, the patient completed a 2-week course of IV metronidazole and ceftriaxone before being transitioned to oral metronidazole and amoxicillin for an additional 4 weeks.
On discharge, the patient’s thrombocytosis persisted, leukocytosis had decreased to 12.8 × 109/L and the only symptom that remained was a mild headache.
Discussion
LS had a mortality rate of 90% when data were first published in 1936. 5 With modern antibiotics, mortality rate ranges from 4% to 12%. 5 Interestingly, there were many reported cases in the early 1900s, but the number of reported cases dropped from the years of 1955 to the 1980s. 5 Riordan hypothesizes that this may have been due to the popularity of using antibiotics to treat infections of the oropharynx during this time.5,8 Of note, there has been an increase in the reported incidence of LS in the last 30 years, possibly explained by an increase in antibiotic resistance and/or more hesitancy to use antibiotics for treatment of oropharyngeal infections. 5
Although the criteria to provide a definitive diagnosis of LS is still contentious, the most agreed upon criteria for diagnosis are the following findings: recent pharyngeal illness, complicated by septic emboli, as well as either thrombosis of the internal jugular vein or findings of F necrophorum in blood cultures. 6 The case presented in this article met only 2 of these criteria: recent odontogenic infection, and extensive thrombosis of the bilateral upper internal jugular veins, transverse sinuses, and sigmoid sinuses. We believe that the dramatic leukocytosis and lack of hemoculture growth in our patient could be explained by containment of infection within the thrombus.
A systematic review found that 95% of cases of LS were diagnosed with CT scans. 6 CT is favorable in that it is cheaper and available in most hospitals compared with magnetic resonance imaging. Ultrasound may also play a role in imaging, but is limited due to its low sensitivity for newly formed thrombosis, as well as impaired visualization of deeper tissues and structures. 6
Due to the rarity of LS cases, a clear consensus on the role of anticoagulation and antibacterial treatment has yet to be established. A review by Riordan 8 suggests that carbapenems, a combination of penicillin/B-lactamase inhibitor, or metronidazole are the best candidates for the treatment of LS. Armstrong and colleagues 9 reported that in the literature, the most frequently used agent was metronidazole. The popularity of metronidazole use in treatment of LS is explained by its high oral availability, its activity against all strains of Fusobacterium spp, and its penetration into tissues. 8 In addition, the literature also suggests treating LS with metronidazole in combination with a penicillin to cover oral streptococci. 8 Riordan details in his review that most cases should undergo IV therapy for 2 to 3 weeks, with transition to 3 to 4 weeks of oral therapy for a total treatment of 6 weeks duration. 8
The role of anticoagulation in the treatment of LS remains to be elucidated. However, anticoagulation is more frequently used in patients who have received 2 to 3 days of antimicrobial therapy with no signs of improvement, underlying thrombophilia, progression of thrombosis, or retrograde extension of cavernous sinus thrombosis. 10 A study by Jaremko and colleagues 11 suggests that anticoagulation likely decreases the risk of clot extension, and has the potential to shorten recovery times. 8 If anticoagulation therapy is clinically indicated, optimal duration is unclear and has been reported to range from 4 weeks to 6 months. 10 In our case, imaging demonstrated extensive thrombosis involving the transverse and sigmoid sinuses bilaterally extending down to the upper jugular veins (Figures 2 and 3). Due to the large size of this thrombus, in addition to the patient’s inherent hypercoagulable state, we opted to treat with anticoagulation, as suggested by the limited literature.
Review of the literature suggests that hypercoagulability may be a predisposing risk factor for the development of LS. Hope and colleagues detailed a case of LS with reduced antithrombin 3 levels.8,12 Klinge and coleagues presented a case of thrombosis of the internal jugular vein (IJV) and sigmoid sinus in a patient with Factor 5 Leiden mutation.8,13 Another case series reported 7 children with mastoiditis and sinus thrombosis, of which 5 had accompanying prothrombotic disorders.8,14 However, a case series of 9 pediatric cases of septic jugular venous thrombosis secondary to oropharyngeal infection reported that 7 children had thrombophilia including 3 with APLA, 4 with raised factor VIII levels, and 1 with factor V Leiden. Six months later, APLA was no longer present in 2 patients, and factor VIII levels returned to normal, suggesting that these thrombophilic conditions were a possible result of the acute inflammatory state rather than true persistent thrombophilia.8,15 Due to the rarity of LS, 1 person per million per year, it is less likely to be a random association between LS and hypercoagulable states, but instead that hypercoagulability may serve as a risk factor for development of LS. 16 In addition, an analysis of 712 patients with LS found that there was a substantial risk of new thromboembolic complications after initial infection. 17 Our case favors the hypothesis that an intrinsic prothrombotic state, such as in our case of hemolytic anemia and splenectomy, may be a risk factor for the development of LS.
This case is unique in that the patient was in a hypercoagulable state prior to developing LS. His chronic hemolytic anemia requiring splenectomy secondary to pyruvate kinase deficiency explains his baseline thrombocytosis. Both chronic hemolytic anemia and thrombocytosis place this patient in a hypercoagulable state due to endothelial damage. In patients with normal platelet counts who have undergone splenectomy, there is evidence of increased platelet adhesiveness. 18 Although rare, a case report documented that a patient with pyruvate kinase deficiency began having recurrent thrombosis post-splenectomy. 18 We hypothesize that both the infectious odontogenic foci, and the tissue damage incurred during tooth extraction further exacerbated our patient’s persistent hypercoagulability, thus predisposing him to venous thrombosis.
Conclusion
In conclusion, we present a rare case of possible LS that originated from an odontogenic source in a patient with intrinsic hypercoagulable state due to hemolytic anemia and asplenia. The role of anticoagulation in the treatment of LS is still debatable, but somewhat supported in cases of progressive thrombosis and hypercoagulable states. It is our hope that adding to the scarce literature on LS will aid in creating definitive diagnostic guidelines and treatment regimens for future cases.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval to report this case was obtained from Kern Medical Institutional Review Board (21012).
Informed Consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.