
Abstract
Takotsubo cardiomyopathy (TCM) is a syndrome of reversible left ventricular systolic dysfunction that, at presentation, can be easily conflated with acute coronary syndrome. TCM has a clinical preponderance for older, postmenopausal females. We report on a patient’s case who presented with complaints of upper and lower extremity weakness with evidence of rhabdomyolysis and hepatic injury. Her occupation as a field worker exposed her to a toxic chemical known as paraquat, which has been banned by multiple countries across the world; a chemical we presume culminated in both. The subsequent clinical cascade and resulting acute physiological illness and emotional distress primed her to develop TCM. However, she neither endorsed chest pain nor dyspnea. Her subtle clinical presentation could have led to a missed diagnosis as she was also not in a fluid overloaded state consistent with the depressed left ventricular function discovered on transthoracic echo. The diagnostic uncertainty until coronary angiography is obtained, and its association with severe and acute emotional and physical stress prompts to a greater reliance on patient history to identify occupational and toxic exposures that can contribute to its development.
Introduction
Takotsubo cardiomyopathy (TCM) is a syndrome of reversible left ventricular (LV) systolic dysfunction most commonly typified by LV apical ballooning and mid and apical segment hypokinesis but without evidence of obstructive coronary artery disease. Though its pathogenesis is not clearly established, given its association with severe and acute emotional or physical stress, the cascade resulting from catecholamine-excess remains a viable theory. We present a case of reversible TCM in a patient with rhabdomyolysis and transaminitis secondary to paraquat exposure.
Case Presentation
A 45-year-old Hispanic female with diabetes, hypertension, and dyslipidemia presented to our hospital with a chief complaint of migratory bilateral upper and lower extremity weakness of one month’s duration preceded by two months of fatigue. On presentation, she was diaphoretic but denied chest pain, shortness of breath, nausea, vomiting, or abdominal pain. Electrocardiogram (EKG) showed Q waves in the inferior and anterior leads but no ST elevations (Figure 1). Troponins were elevated to 2.57 prompting acute coronary syndrome (ACS) workup and management; she was started on aspirin, clopidogrel, and therapeutic heparin drip. High-dose atorvastatin was held as the patient had been on statin therapy prior to admission for unknown duration due to concerns for possible immune-mediated necrotizing myopathy. Transthoracic echocardiography (TTE) showed a LV ejection fraction of 20% to 25% with akinetic mid and distal segments and apical ballooning highly suggestive of TCM. We started the patient on guideline-directed medical therapy with lisinopril 2.5 mg daily and carvedilol 3.125 mg twice daily for systolic dysfunction. Left and right heart catheterization to rule out ischemic etiology of her cardiomyopathy was performed and showed lack of obstructive coronary artery disease (Figure 2).
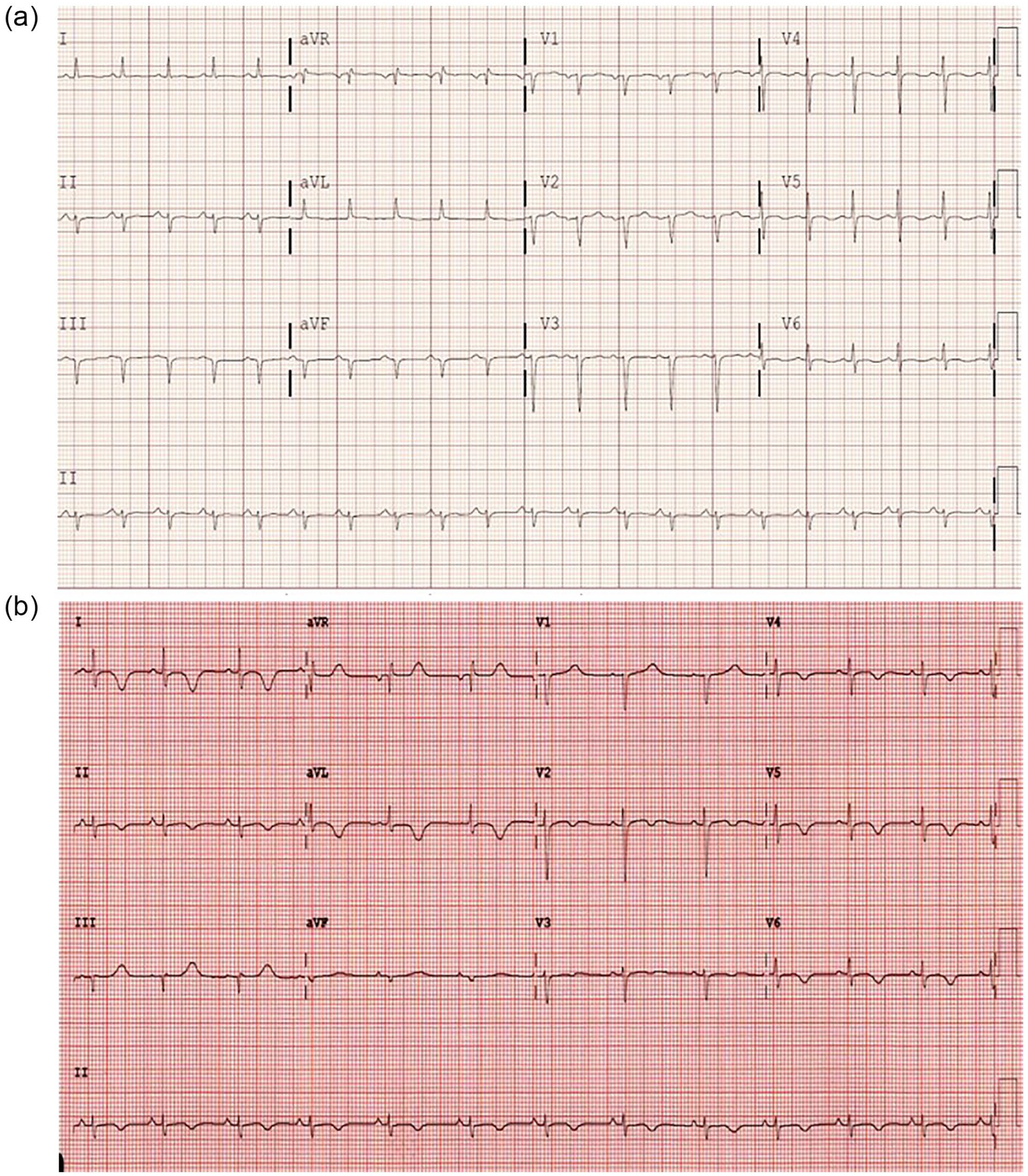
(a) Electrocardiogram (EKG) from admission showing Q waves in inferior and anterior leads. (b) EKG from clinic follow-up showing diffuse T wave inversions.

Coronary angiography of our patient showing clear and patent left anterior descending (LAD), left circumflex (LCx), and right coronary (RCA) arteries.
Pertinent laboratory values on presentation were a serum glucose of 134 mg/dL, creatine kinase (CK) of 14 848 U/L, lactate dehydrogenase of 1414 U/L, aldolase of 168.8 U/L, alanine transaminase of 748 U/L, and aspartate aminotransferase of 651 U/L (Table 1). There were no baseline laboratory values for comparison. Urinalysis had trace but insignificant levels of protein and evidence of large blood but also corresponding 5 to 10 red blood cells. An intensive workup for rheumatologic, infectious, and autoimmune causes of myopathy were undertaken. An antinuclear antibody of 1:80 returned positive but thyroid stimulating hormone, erythrocyte sedimentation rate, viral hepatitis serologies, workup for systemic lupus erythematosus, Sjogren’s, and rheumatoid arthritis along with viral causes of myocarditis returned within normal limits. Electromyography studies were consistent with active myopathy, magnetic resonance imaging of the brain was unremarkable, and magnetic resonance imaging of the pelvis showed diffuse muscular edema bilaterally through proximal thighs (Figure 3).
Pertinent patient laboratory values starting from the day of admission through follow-up.
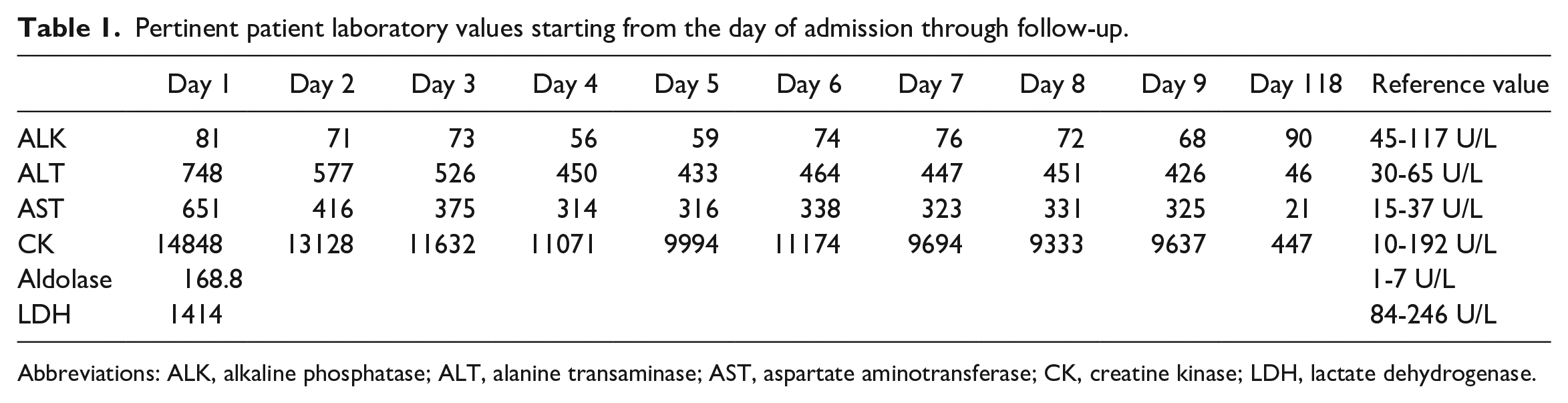
Abbreviations: ALK, alkaline phosphatase; ALT, alanine transaminase; AST, aspartate aminotransferase; CK, creatine kinase; LDH, lactate dehydrogenase.

Magnetic resonance imaging of the pelvis showing diffuse bilateral muscle edema without atrophy.
The patient was evaluated daily during the course of her admission and endorsed her muscle weakness was slowly improving. Further history from the patient elucidated her muscle weakness began around the time she started working in a new grape field where paraquat had been sprayed 1 month prior, as confirmed by the Southern Valley Chemical Spraying company. The patient also reports having drank water from a tub filled with hose water while there. Muscle biopsy was performed but electron microscopy of muscle sampled from the patient’s right gluteus muscle returned inconclusive. TTE repeated six days after admission showed an LV ejection fraction improved to 50% to 55% and no regional wall motion abnormalities coinciding with the patient’s improved clinical picture of increased upper and lower extremity muscle strength and resolving CK and transaminitis. The patient was subsequently discharged home. She returned to cardiology clinic one week after hospital discharge where she demonstrated complete resolution of muscle weakness. Statin therapy was not reinitiated as her calculated Atherosclerotic Cardiovascular Disease score was <2%.
Discussion
Takotsubo cardiomyopathy is colloquially referred to as “broken heart syndrome” for its strong association with severe and acute stressors. A systematic review reports TCM was preceded by physical and emotional stressors with incidences of 37.8% and 26.8%, respectively. 1 Physiologic stressors have included preceding asthma attack, bronchoscopy, colonectomy, or surgery. 2 Our patient denied any emotional triggers or upset such as death of a loved one, marital problems, financial distress, but we believe the emotional distress of sudden physical incapacitation in conjunction with her acute physical illness caused by the paraquat toxicity contributed to the development of Takotsubo. Also of note, there is an age predilection with a majority of TCM patients falling in the age range of late 50s to early 80s, along with a gender predilection with a higher proportion of females—as high as 90%—being diagnosed with TCM.1-3
The diagnosis of TCM typically requires EKG, cardiac enzymes, and angiography due to the conflated clinical picture of most patients who present with presumed ACS. Patients can present endorsing chest pain or dyspnea and some can present in cardiogenic shock.1-3 As the workup for ACS commences, EKG changes have been noted to show ST elevations in the acute phase, T wave inversions in the late phase, QT prolongation, or Q waves in the subacute phase as did our patient. 1 One study of 18 patients showed consistent ST elevations in leads V3-V6 during the acute phase—a hallmark also of anterior myocardial infarction (MI). 2 As reciprocal changes and Q waves were not observed, this led to stronger diagnostic certainty for TCM as opposed to anterior MI when the left anterior descending lesion among MI patients was more proximal. This observation, however, lost reciprocity if the LAD lesion was more distal as those patients also had an absence of such features. 2 Cardiac enzymes are often elevated, albeit with lower levels than observed in ACS, and resolve sooner.1,3 Echocardiography in the acute phase have shown both mid-ventricular dysfunction and apical hypokinesis or apical ballooning with akinesis. The ejection fraction will range from 20% to 49%. These patients will ultimately undergo angiography given there is no consistent nor reliable way to distinguish between TCM and ACS with EKG and cardiac markers alone. Angiography will then show clear coronary arteries without evidence of obstructive lesions or minimal stenosis <50%.1,3
Management of TCM is similar to heart failure with reduced ejection fraction: β-blockers, angiotensin-converting enzyme inhibitors, and diuretics.1,3,4 Given that our patient did not present with any signs or symptoms of fluid overload, we initiated her only on the former two. Overall prognosis for those with TCM is quite good, with improvements in EKG findings, cardiac markers, and ejection fraction taking place within days. 3 For our patient, the recovery of LV function within one week coincided with significant improvements in her clinical picture, with resolving weakness, CK, and transaminitis. This lends credence (1) that her acute illness precipitated her Takotsubo as her cardiomyopathy resolved once the illness started to show resolution and (2) to the β-2 adrenoreceptor/inhibitory G protein theory. The latter is a proposed pathophysiological mechanism for the development of TCM, which states that increased adrenaline during acute stress or illness leads to hyperstimulation of β-2 receptors. As the β-2 receptors are stimulated this leads to a switch in intracellular signaling from stimulatory G (Gs) to activation of inhibitory G (Gi) proteins. This results in reductions of cyclic adenosine monophosphate levels causing negative inotropy and ultimately, contractile dysfunction. There is a base to apex increase in density of β-2 receptors; hence, the observed hypokinesis is most pronounced at the cardiac apex in cases of TCM.1,3-5 The activation of Gi proteins with continued adrenergic stimulation is proposed to be a cardioprotective mechanism to protect against catecholamine-induced myocardial damage as demonstrated in an in vivo rat model study where Gi inactivation (blunting of this cardioprotective mechanism) with pertussis toxin prior to high-dose epinephrine administration led to increased mortality. 6 This mechanism may also explain the variance in prognosis between heart failure and TCM and rapid reversal of the latter. Of note, as the patient’s symptoms resolved in the setting of both atorvastatin cessation and discontinued paraquat exposure, we cannot reliably exclude immune-mediated necrotizing myopathy from atorvastatin usage as cause for her proximal muscle weakness, especially given that the muscle biopsy was inconclusive.
We believe paraquat, a nonselective contact herbicide known to cause severe systemic toxicity, initiated the cascade of rhabdomyolysis and hepatic injury for our patient. Paraquat concentrates intracellularly where it undergoes redox cycling producing paraquat-radicals. The super oxide radicals are highly reactive and cause direct cellular damage. 7 Inhalation or ingestion of a large amount of paraquat is commonly associated with lung injury or pulmonary fibrosis progressing into respiratory failure and direct caustic damage throughout the gastrointestinal tract manifesting as nausea, vomiting, abdominal pain, and diarrhea. 8 Chronic low-dose exposure, however, is more likely to affect the liver, heart, and kidneys. Paraquat targets the biliary excretory pathways in the liver causing cholangiocellular injury of bile ducts in the portal areas. Paraquat-induced myopathy can also occur after prolonged exposure—the toxin causes degeneration of muscle fibers correlating with abruptly increased plasma CK levels. 9 Our patient’s exposure was primarily cutaneous and she did not demonstrate pulmonary or gastrointestinal manifestations, or parkinsonian features (tremor, rigidity, bradykinesia) as paraquat poisoning has been linked to an increased risk of Parkinson’s disease. 10 Although the patient was exposed to numerous herbicides working in the field, paraquat is the only agent known to cause hepatic, myocardial, renal, and skeletal muscle injury.
Conclusions
Our patient presented with bilateral extremity weakness from myopathy caused by paraquat exposure that led her to present to the emergency department. The clinical cascade of events surrounding her acute illness precipitated TCM as she was found to have elevated troponins, Q waves on presenting EKG, and an ejection fraction of 20% to 25% on TTE with normal coronary arteries on angiography. We optimized the patient with guideline-directed medical therapy at the time of diagnosis, and she had rapid recovery of LV function within seven days with repeat TTE showing LV ejection fraction of 50% to 55%. The resolution of her TCM was preceded by days of gradual proximal muscle weakness reversal and laboratory values reflecting down-trending CK and transaminitis. Reversible cardiomyopathy can develop in the setting of catecholamine surge prompted by severe physiological stressors as we discussed above. We believe our patient’s acute myopathy was triggered by exposure to an herbicide that has been banned by many countries across the world. When diagnosing a patient with multi-organ involvement, obtaining a detailed occupational and toxic exposure history plays a critical role in quickly and accurately identifying a reversible cause of what could be a fatal disease. Recognition of this presentation is crucial as disease progression can lead to severe multi-organ failure and early discontinuation of paraquat exposure can lead to an excellent outcome, as in this case.
Footnotes
Acknowledgements
Kern Medical Internal Medicine Department and Faculty.
Authors’ Note
This case report was presented as an oral presentation at the Western Medical Research Conference in Carmel, California, on January 25, 2019. An abstract of this case report was published in the Journal of Investigative Medicine, 2019;67:162-224.
Author Contributions
SJ: Collected clinical data, compiled references, authored and revised all drafts. TW: Corresponding author and edited all drafts. FJ, AH, and LM: Offered proof of concept. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Kern Medical Internal Medicine Department.
Ethics Approval
The institutional review board at our institution, Kern Medical, has approved this study (IRB Study # 18071).
Informed Consent
Written informed consent was obtained from the patient to utilize their unidentified information and images for publication of this case report.