
Abstract
Pancreatitis is inflammation of pancreas associated most commonly with chronic alcoholism and gallstones. Other less common causes of pancreatitis are hyperlipidemia, infections, surgery, trauma, post endoscopic retrograde cholangiopancreatography, and drugs. Drugs are now increasingly recognized as a cause of pancreatitis, and high suspicion and exclusion of other most common causes is required before considering drug-induced pancreatitis. There are few case reports of acute pancreatitis in the literature after statin use, but out of these, only 3 are after starting pravastatin. We are reporting a case of 49-year-old male who presented with nausea, vomiting, and abdominal pain. His laboratory findings were significant for lipase more than 10 000 on admission, and computed tomography scan of abdomen was showing peripancreatic fat stranding and inflammation. After exclusion of most common causes of pancreatitis, pravastatin was found probable culprit for his symptoms, which he started taking 2 weeks ago. We also reviewed the literature on statins-induced acute pancreatitis. With increased uses of statins, physician need to be vigilant to suspect statins as a culprit in cases of pancreatitis with unknown etiology. Prompt discontinuation of statins is required in these cases.
Introduction
Acute pancreatitis is a life-threatening condition. It is one of the leading gastrointestinal causes of hospitalization in the United States. 1 Among the numerous documented etiologies of acute pancreatitis, gallstones and alcoholism are the most common. Among other less common causes, drug-induced causes account for less than 2%.2,3 Drug-induced pancreatitis has been reported since 1950s, and with time, new medications are added in the list. 4 Even with advances in diagnostic medicine, etiologies in 30% cases of pancreatitis remains unknown. 5 Previously, drug-induced pancreatitis was classified as definite, probable, or possible, but now used classification was introduced by Badalov and colleagues in which drugs are divided into 5 classes: 1a, 1b, II, III, and IV. This classification is based on number of case reports, ability to exclude other causes, latency period, and available rechallenge data. Pravastatin is defined as class 1a drug based on the presence of at least 1 case report and positive rechallenge data. 6 Few other drugs frequently used in clinical practice associated with pancreatitis are angiotensin-converting enzyme inhibitors, diuretics, oral contraceptives, highly active antiretroviral therapy, valproic acid, atypical antipsychotics, antibiotics, and antivirals.4,6
There are a few reported cases of statin-induced pancreatitis, and in our research, we found only 3 cases of pravastatin-induced pancreatitis. We are reporting the fourth case of pravastatin-induced pancreatitis. Drug-induced pancreatitis is a diagnosis of exclusion, and one needs a high index of suspicion to recognize it.
Case Presentation
A 49-year-old male with past medical history of dyslipidemia, hypertension, coronary artery disease status post coronary artery bypass grafting, diabetes mellitus, liver cirrhosis secondary to hepatitis C presented with a 3-day history of epigastric pain radiating to the back, nausea, and vomiting. He reported that the pain was started initially in the right lower quadrant but later migrated to epigastric area, 9/10 in intensity, and sharp in character. He also endorsed associated fever, shortness of breath, decreased appetite, and abdominal distention. On presentation, he was normotensive with blood pressure of 130/80 mm Hg, heart rate 78 beats/minute, temperature 97.8 °F, and respiratory rate of 18 breaths/minute. Physical examination was significant for severe epigastric tenderness. There was no rebound tenderness or rigidity. The patient denied any history of similar complaints in the past. He denied cigarette smoking, and there was no known alcohol or illicit drug abuse. He also denied any recent abdominal trauma. He denied family history of chronic pancreatitis and personal history of cystic fibrosis or any other autoimmune diseases.
Investigations
At the time of admission, laboratory findings were significant for a lipase greater than 10 000 units/L. Other significant laboratory values were white blood cell 11.5, alanine aminotransferases 115 units/L, aspartate aminotransferases 102 units/L, creatinine 1.37 mg/dL, and alkaline phosphatase 78. Electrocardiogram and chest X-ray were unremarkable. Based on history, physical examination findings, and elevated lipase, a diagnosis of acute pancreatitis was made. This was confirmed with computed tomography scan of abdomen showing peripancreatic fat stranding consistent with acute pancreatitis, and it was negative for intra- or extrahepatic biliary ductal dilatation (Figures 1 and 2).

Computed tomography (axial view) scan of abdomen showing diffuse peripancreatic inflammatory changes and fat stranding.

Computed tomography (coronal view) scan of abdomen showing diffuse peripancreatic inflammatory changes and fat stranding.
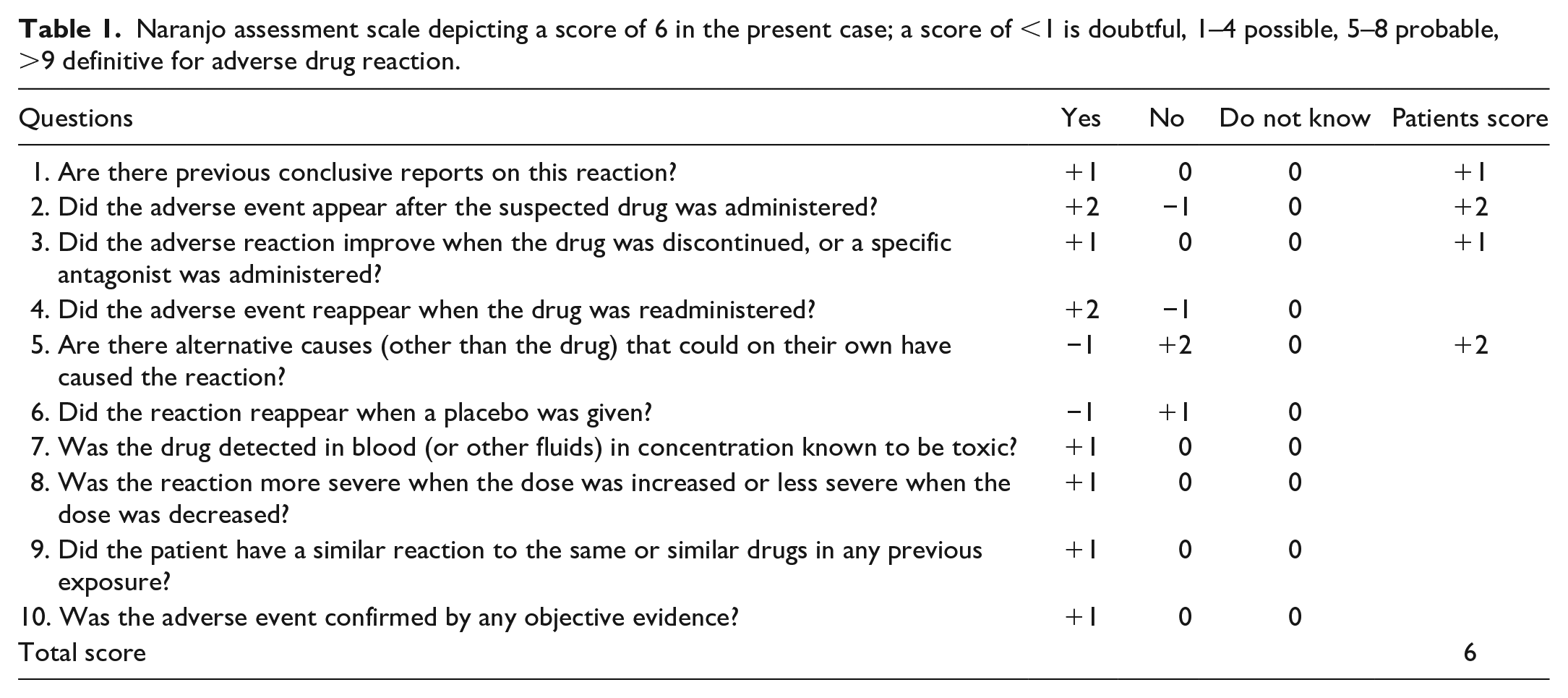
Further workup was done to find the etiology of his pancreatitis. Ultrasound of abdomen was negative for gallstones. Triglyceride level was 78 mg/dL and calcium were 8.8 mg/dL. A urine drug screen was negative. The patient denied alcohol intake and had no prior history of alcohol abuse. No other causes were identified. A review of his home medication revealed that he was recently started on 80 mg of pravastatin 2 weeks ago. We believe that pravastatin was the probable cause of his acute pancreatitis. The Naranjo Nomogram for adverse drug reaction assessment Naranjo score was 6 (Table 1).
Naranjo assessment scale depicting a score of 6 in the present case; a score of <1 is doubtful, 1–4 possible, 5–8 probable, >9 definitive for adverse drug reaction.
Treatment and Outcome
The patient was placed on bowel rest, started on intravenous fluids and pain medications. All his medications were continued except pravastatin. His hospital course was complicated by small bowel obstruction, managed with nasogastric tube insertion connected to suction. After discontinuing pravastatin, his abdominal pain, nausea, and vomiting resolved. Repeat lipase at 48 hours was 378 U/L, and at 96 hours, it had dropped down to 90 U/L. His small bowel obstruction also resolved, and his diet was advanced as tolerated. At discharge, he was hemodynamically stable and asymptomatic. All his medications were continued except pravastatin. After stopping pravastatin, patient recovered well, and at 2-week follow-up in clinic, he was asymptomatic and pain free.
Discussion
Statins are generally well tolerated, but there are reported cases of acute pancreatitis with different statins that point toward a class effect.7,8 Exact mechanism of statin-induced pancreatitis is not well recognized, but different mechanisms are described, which include immune-mediated inflammatory response, direct cellular toxicity, and metabolic effect. 4
Our patient was not an alcoholic and had no family history of pancreatitis. In addition, other causes of pancreatitis were ruled out, which further strengthen the possibility that pravastatin was the probable etiology of acute pancreatitis. In literature, there are reports of pancreatitis due to atorvastatin,9-14 lovastatin,15-17 rosuvastatin,11,18 fluvastatin,19,20 pravastatin,21-23 and simvastatin.8,24-29 There are, so far, 3 reports of pravastatin-induced pancreatitis, and we are reporting the fourth case.
In previously reported cases, pancreatitis developed when statins were introduced in presence of another drug that led to pancreatitis.10,13,16,17 This could indicate a possible drug interaction as a mechanism of statin-induced pancreatitis. Our patient was on lisinopril for the past 3 years, which has been reported as a cause of drug-induced pancreatitis, 30 but lisinopril was not stopped and his symptoms were resolved. We, therefore, suggest that our patient developed pancreatitis due to pravastatin.
In majority of statin-induced pancreatitis, patient outcome was favorable except in 1 case where patient had a fatal outcome. 24 The exact time of developing pancreatitis is not well defined as in 1 case, it developed right after starting statins,9,27 and in other cases, it developed within months to years.13,17,26 In few cases, statins were reintroduced, which lead to recurrence of pancreatitis,15,19,21,25 except in one case where readministration of statin was not associated with recurrence. 17 We did not challenge our patient with statin.
We reviewed the literature in detail and found 22 case reports of acute pancreatitis secondary to statins between inception and April 10, 2021. The previously reported cases of statin-induced pancreatitis and our case are reported in Table 2.
Cases of Statins induced pancreatitis previously reported in the literature.

Abbreviation: BID, twice daily.
Based on these findings, statins should be considered a possible cause of pancreatitis in patients who are on statin and need immediate attention and discontinuation. More prospective studies are needed on a large population to look into this association of statin-induced pancreatitis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient for their anonymized information to be published in this article.