
Abstract
A 67-year-old male was admitted with shortness of breath and diarrhea. His COVID-19 polymerase chain reaction test was positive, and he was found to be in acute heart failure. Troponin levels were elevated, echocardiogram showed ejection fraction of 24%, and his electrocardiogram was normal. Inflammatory markers were elevated. Further testing revealed suppressed thyroid-stimulating hormone and elevated free thyroxine (T4). Differential diagnosis at this point included possible myocarditis from the viral illness, exacerbation of heart failure from the viral infection or from thyrotoxicosis was considered. Patient’s heart failure improved with initiation of heart failure therapies; however, biochemically, his thyroid function tests (TFTs) did not improve, despite empiric methimazole. Thyroid antibody tests were unremarkable. Thyroid ultrasound showed mildly enlarged thyroid gland with no increased vascularity and 5-mm bilateral cysts. Thyroid dysfunction was attributed to subacute thyroiditis from COVID-19, methimazole was tapered, and prednisone was initiated. The patient’s TFTs improved. With the ongoing COVID-19 pandemic, it is imperative that clinicians keep a broad differential in individuals presenting with heart failure, and obtaining baseline TFTs may be reasonable. Rapid treatment of the underlying thyroiditis is important in these patients to improve the cardiovascular outcomes. In our experience, steroid therapy showed a rapid improvement in the TFTs.
Introduction
The world has seen an emergence of a novel coronavirus disease 2019 (COVID-19), which has led to a global pandemic causing numerous hospitalizations and deaths. Healthcare systems have grappled with varied manifestations of the disease ranging from asymptomatic presentation to mild viral pneumonia and to those presenting with acute respiratory distress syndrome, stroke, and myocardial infarction. The pathogenesis of the disease involves entry of the virus through the respiratory system using the angiotensin-converting enzyme 2 (ACE2) as a receptor. 1 Current data indicate that the major cause of acute respiratory distress syndrome and multi-organ failure is due to the overproduction of inflammatory markers resulting in a cytokine storm. 2 Endocrine systems have also been affected by the virus through unknown mechanisms. Thyroid dysfunction has been seen in these patients with some presenting with nonthyroidal illness syndrome to others presenting with thyrotoxicosis from subacute thyroiditis. mRNA encoding for ACE2 receptors have also been identified in thyroid tissue samples, making them a potential target for inflammation.3-6 In this article, we present a case of a 67-year-old male who presented with COVID-19-induced subacute thyroiditis and heart failure.
Case Report
A 67-year-old male with a past medical history of chronic systolic and diastolic heart failure, coronary artery disease, diabetes mellitus type 2, chronic kidney disease, and atrial fibrillation was admitted with shortness of breath and diarrhea. Chest X-ray showed bilateral infiltrates. N-terminal pro B-type natriuretic peptide (NT-proBNP) was elevated at 24591 pg/mL (<350 pg/mL). Troponin was high at 0.15 ng/mL (0.3-0.10). Electrocardiogram did not show any ST-segment changes. C-reactive protein (CRP) level, 5.3 mg/dL (0.1-0.4 mg/dL), and erythrocyte sedimentation rate (ESR) level 37 mg/dL (0-15 mg/dL) were both elevated. Echocardiogram showed left ventricular ejection fraction of 24%.
The patient’s COVID-19 polymerase chain reaction testing was positive. Patient was started on ceftriaxone and azithromycin for pneumonia, and intravenous diuretics for heart failure. He had acute onset of atrial fibrillation for a brief duration, with spontaneous return to regular rate and rhythm.
Thyroid function tests (TFTs) obtained for further evaluation of arrhythmia showed a low thyroid-stimulating hormone (TSH) of 0.029 uIU/mL (0.27-4.2 ulU/mL) and elevated free thyroxine (T4) of 2.1 ng/dL (0.8-1.7 ng/dL; Table 1). He had no neck pain or preexisting diagnosis of hyperthyroidism. There was no history of biotin, levothyroxine, or amiodarone use. Patient had symptoms of weight loss, fatigue, and diarrhea. His thyroid examination was normal, and he had no proptosis. It was initially unclear if the patient may have had early Graves’ disease, toxic nodule, or thyroiditis. The patient was started on methimazole 20 mg daily, and thyroid autoantibody testing was obtained.
Treatment and Laboratory Values.

Abbreviations: TSH, thyroid-stimulating hormone; T4, thyroxine; T3, triiodothyronine; TSI, thyroid-stimulating immunoglobulin; ESR, erythrocyte sedimentation rate; CRP, C-reactive protein; bid, twice daily.
TFTs did not improve, and evaluation 4 weeks after initiation of methimazole showed elevated free T4 levels of 2.36 ng/dL (0.8-1.7 ng/dL) and undetectable TSH. Thyroid-stimulating antibodies, thyroid peroxidase antibody, thyroglobulin antibody level, and thyroid receptor antibody levels were normal. Thyroid ultrasound showed mildly enlarged thyroid gland with no increased vascularity and 5-mm bilateral cysts.
At this point, he was presumed to have to subacute thyroiditis from COVID-19. He was started on prednisone, and methimazole was tapered. Within a week, patient’s free T4 decreased to 1.36 ng/dL (0.8-1.7 ng/dL), and TSH then became detectable at 0.007 ulU/mL (0.27-4.2 ulU/mL) (Figure 1). Initially methimazole and then prednisone was slowly tapered over months. Patient is currently off methimazole and prednisone. His most recent TFT shows TSH of 1.05 ulU/mL (0.27-4.2 ulU/mL) and free T4 of 1.1 ng/dL (0.8-1.7 ng/dL). Patient is clinically asymptomatic, and we are closely watching his TFTs.
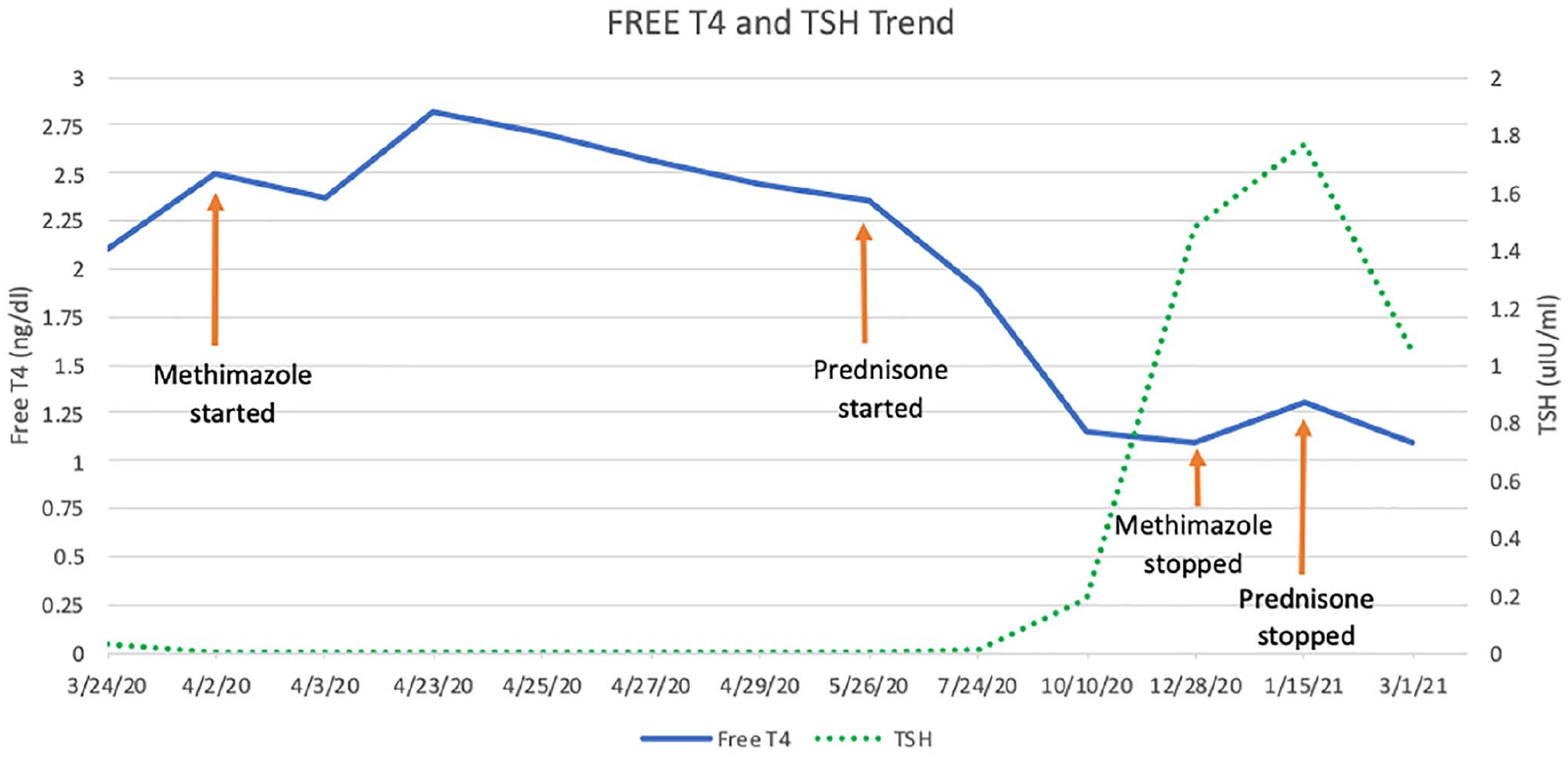
Free thyroxine (T4) and thyroid-stimulating hormone (TSH) trend.
Discussion
On initial presentation, the patient had acute on chronic systolic heart failure. There was a preexisting history of chronic systolic congestive heart failure, which was likely exacerbated by COVID-19-induced thyroiditis. Myocarditis is also a differential diagnosis due to similarities in the clinical presentation. The clinical features of myocarditis may vary from subclinical disease to overt presentation of chest pain, heart failure, arrhythmias, and cardiogenic shock. The major causative agents in myocarditis are infectious causes, viral infections being a predominant factor. 7
Subacute thyroiditis is a self-limited inflammatory disorder of the thyroid gland. The most common etiology of subacute thyroiditis is due to inflammatory process by viral infection.
A strong association with HLA-B35 antigen has been noted, with a higher predilection in females.8,9 The association of subacute thyroiditis with viral infections was noted back in the 1930s to 1940s, with measles, malaria, and scarlet fever.10-12 Direct evidence of the virus in the thyroid tissue has been seen in patients infected with mumps and retrovirus. 13 It is interesting to note that previous epidemics with mumps have seen outbreaks of small clusters of subacute thyroiditis, 14 and the outbreak of SARS in 2002-2003 also reported thyroid dysfunction. 15 Classic symptoms of subacute thyroiditis include acute neck pain, tender thyromegaly, and thyrotoxicosis. TFTs show elevated free T4 levels with suppressed TSH response. 16 Inflammatory markers are usually elevated. 17 In situations when the diagnosis is in doubt, imaging studies such as radioactive iodine uptake and thyroid ultrasound can be helpful. Radioactive iodine uptake would show low activity. Thyroid ultrasound may show focal or diffuse heterogeneous/hypoechogenic areas, and the size of the thyroid gland would usually be normal. However, there are patients diagnosed with subacute thyroiditis who do have an enlarged thyroid gland on ultrasound. 18 Thyroglobulin antibodies and thyroid peroxidase antibodies have been seen in some cases of subacute thyroiditis, but it is generally absent. 19 In our case, the patient had suppressed TSH, with elevated free T4 levels and elevated markers of inflammation. Due to COVID-19 contact and droplet precautions, a radioactive iodine uptake scan was not performed. Therapy for subacute thyroiditis largely involves symptomatic measures and prednisone. Our patient improved with prednisone treatment.
COVID-19-induced thyroiditis and thyrotoxicosis cases are increasing,20-28 and COVID-19-induced myocarditis has already been recognized as the cause of death in many cases.29,30 As such, it is important for physicians to have a broader differential in mind when evaluating cases presenting with heart failure in the setting of COVID-19.
Conclusion
With the ongoing COVID-19 pandemic, it is imperative that clinicians keep a broad differential in individuals presenting with heart failure, and obtaining baseline TFTs may be reasonable. Rapid treatment of the underlying thyroiditis is important in these patients to improve cardiovascular outcomes. In our experience, steroid therapy showed a rapid improvement in the TFTs when tackling a case with subacute thyroiditis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient for their anonymized information to be published in this case report.