
Abstract
Right atrial (RA) masses are rare, challenging to diagnose, and potentially life-threatening with high mortality if untreated. We present a patient presenting with diffuse large B-cell lymphoma in the brain that was incidentally found to have a large RA mass. For a better definition of the RA mass, extensive workup using multimodality imaging including chest computed tomography, transthoracic echocardiography, transesophageal echocardiography, cardiac magnetic resonance imaging, and left heart catheterization was warranted. The imaging demonstrated a large RA mass extending through the tricuspid valve into the right ventricle and superior and inferior vena cava without a mobile component. The mass was then successfully resected, and further histology examination was performed to rule out lymphoma and rare subtypes of diffuse large B-cell lymphoma. The comprehensive workup proved the RA mass to be a calcified thrombus rather than a direct metastatic spread of lymphoma.
Keywords
Case Presentation
A 56-year-old Caucasian female was referred to our cardiology clinic with fatigue, forgetfulness, visual abnormalities, chest heaviness, abdominal bloating, and peripheral edema. The patient’s past medical history includes infiltrating ductal breast carcinoma with mastectomy and chemotherapy, 18 years prior, and access port thrombosis necessitated removal at that time. She drinks occasional alcohol but has never used tobacco or illicit drugs. Her family history was remarkable for malignancy.
The patient had a recent brain computed tomography (CT) scan demonstrating multiple lesions concerning possible demyelinating disease or malignancy. Subsequent brain magnetic resonance imaging (MRI) with contrast confirmed enhancing lesions in the left inferior frontal lobe, the left posterior Globus Pallidus, and the right parietal white matter with associated edema on FLAIR images (Figure 1). CT scan of chest, abdomen, and pelvis performed to scan for other lesions revealed an incidental calcified right atrial (RA) mass measuring 4.5 × 2.5 × 4.5 cm, which appeared to extend through the tricuspid valve into the right ventricle (RV). Transthoracic echocardiogram (TTE) and transesophageal echocardiogram (TEE) confirmed the presence of a calcified 4-cm RA mass without a mobile component and with no valvular pathology, nor patent foramen ovale (Figure 2E; Videos 1 and 2, available online). This mass was not identified on TTE performed 5 months earlier. Cardiac MRI further defined the mass as a probable calcified RA thrombus with extension into the RV, inferior vena cava, and superior vena cava with no enhancement to suggest metastatic disease (Figure 2A-D). The patient was started on anticoagulation with Apixaban and advised to follow-up with TTE. Repeat TTE a few months later indicated an apparent increase in the size of the RA mass. The initial decision was made to monitor the mass and the patient was then referred to our clinic for a second opinion.

Brain magnetic resonance imaging, performed before diffuse large B-cell lymphoma diagnosis. (Image 1) Post-contrast T1-weighted image demonstrates enhancing lesions in the left inferior frontal lobe and posterior Globus Pallidus. (Image 2) Post-contrast T1-weighted image demonstrates a third smaller arc of enhancement in the right parietal deep white matter. (Image 3) FLAIR image demonstrates the extension of white matter edema from a more superior lesion into the level of image 3.
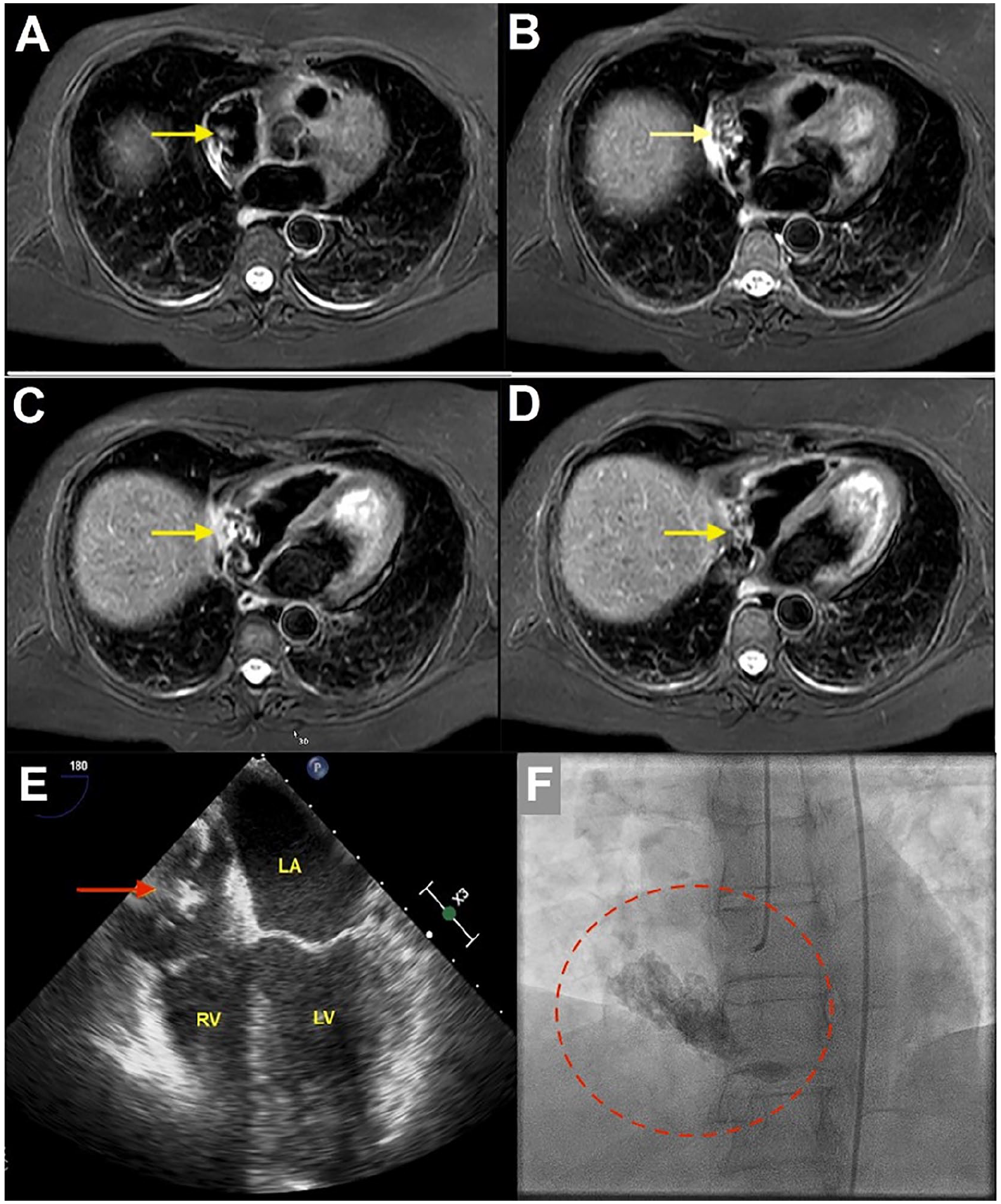
Cardiac magnetic resonance imaging demonstrating calcified right atrial (RA) thrombus (yellow arrows) (A and B) with extension into the right ventricle and inferior vena cava (yellow arrows) (C and D). TEE 4-chamber view, with calcified RA mass (red arrow) (E). Left heart catheterization identified a large calcified RA mass with extension into the right ventricle; no tumor blush detected (red circle) (F).
The case was discussed with interventional cardiology, and cardiovascular surgery and surgical excision with biopsy was recommended. At the time of admission to our hospital for surgery, the patient was hemodynamically stable with mild to moderate pedal edema and normal neurological examination, outside of the stable patchy loss of vision in the right eye. Laboratory studies including electrolytes, renal and liver function, C-reactive protein, and erythrocyte sedimentation rate were normal, platelet count was 159 000/µL, and prothrombin time-international normalized ratio was 1.1. HIV serology and blood cultures were negative. TEE and left heart catheterization were performed, demonstrating no coronary artery disease, normal left ventricular size, and systolic function, ejection fraction of 60%. A large calcified density was identified in the right atrium under fluoroscopy (Figure 2F; Video 3, available online) and on TEE.
During surgery, the RA mass was noted to be totally calcified and attached to the atrial wall extending to the RV and inferior vena cava. The origin point was not defined but was deemed close to the coronary sinus and the tricuspid valve annulus. The mass was resected along with the free wall of the right atrium to within about 5 to 6 mm of the tricuspid valve and right up to the edge of the orifice of the coronary sinus. The mass was then broken up to be completely removed and was sent for pathological examination. A bovine pericardial patch was then used to reconstruct the large defect in the right atrium. The patient tolerated the operation well with no complications and the postoperative period was uneventful. The initial pathology report was negative for malignancy and reported as a calcified amorphous cardiac tumor, a suspected calcified mural thrombus (Figure 3). Repeat MRI of the brain was performed after surgical resection of the RA mass for symptoms of increasing headache and visual disturbance. MRI demonstrated enlarging cerebral lesions. Cerebral diffuse large B-cell lymphoma (DLBCL) was diagnosed on subsequent biopsy with a germinal center-like phenotype. Further extensive pathologic analysis of the RA mass and additional pathology evaluation by outside consultants was performed, confirming the diagnosis of calcified mural thrombus, with minimal cellularity.

Hematoxylin and Eosin-stained right atrial mass specimen, consistent with an acellular cardiac calcifying amorphous tumor, calcified thrombus. Magnification 194× (A) and 630× (B).
With an unremarkable postoperative course, the patient was successfully discharged after 4 days in the hospital. On a follow-up visit 2 weeks later, the patient endorsed improved symptoms with a marked decrease in chest heaviness, improved abdominal bloating, and decreased edema. Follow-up chest CT and TTE demonstrated a residual rim of calcified tissue in the right atrium at the site of prior mass attachment and some decrease in RV function.
Discussion
Right atrial mural thrombi are rare and most often related to central venous catheter (CVC) insertion: one retrospective autopsy study discovered RA mural thrombi in 24 out of 940 hearts. Twenty-three of these patients had CVC insertion before death. 1 The back-and-forth motion of the catheter within the RA cavity is believed to produce mechanical trauma in the RA, predisposing to mural thrombus formation. The prior history of prolonged CVC placement for chemotherapy in our case may have predisposed for thrombus formation; however, catheter placement and thrombosis were remote (18 years prior). Thromboembolism is a common complication with all cancer states and is frequent in patients with brain cancer subtypes. Goldschmidt et al found that 59.5% of central nervous system lymphoma subjects had thromboembolism and 7% were fatal, supporting anticoagulant prophylaxis in cancer patients. 2
RA tumors are either benign or malignant; the majority being metastatic. Current literature reports an 8.7% to 29% incidence of cardiac metastasis in patients with lymphoma. 3 Intravascular large B-cell lymphoma is a rare cancer subtype that allows malignant lymphoid cells to induce thrombus formation. 4 Diffuse large B-cell lymphoma with chronic inflammation (DLBCL-CI) is an Epstein-Barr virus-driven neoplasm associated with chronic inflammation in restricted spaces. Among this class, a rare form of DLBCL-CI is recognized as fibrin-associated diffuse large B-cell lymphoma (FA-DLBCL) with associated clusters, ribbons, or sheets of large atypical lymphoid cells within superficial layers of fibrin, most commonly involving atrial myxomas or thrombi (31%). 5 The rapid RA mass growth with cerebral DLBCL in our case warranted further histological analysis for FA-DLBCL and was negative.
Diagnostic imaging of RA masses is challenging because RA structures such as a prominent pectinate, crista terminalis, eustachian, and thebesian valves can be misinterpreted. 6 Echocardiography is the first-line imaging study; however, it is unable to (1) differentiate myxomas from mural thrombi; (2) fully assess an invading cardiac mass; and (3) perform tissue characterization. 7 Nonconclusive echocardiographic findings are indications for cardiac magnetic resonance (CMR) or cardiac computerized tomography (CCT). Magnetic resonance is superior to CT scan, which should be used only when CMR is unavailable or contraindicated. CMR differentiates mural thrombi from atrial tumors, identifies specific tissue characteristics of different tumors, and detects the anatomic relations of the mass with other cardiac structures. 8
While primary cardiac tumors are surgically resected to prevent life-threatening complications, metastatic tumors are not considered a justification for surgical resection unless for palliative purposes. 9 Treatment of right heart thromboembolism remains controversial. Various treatments include surgery, thrombolysis, and anticoagulation with heparin. Thrombolysis is the treatment of choice for patients with a right heart thrombus and secondary pulmonary embolism (PE). However, in the absence of PE, it is not clear which treatment is superior. The prognosis is generally poor, especially when a right heart thrombus is complicated by a PE: one case series of 38 patients with right heart free-floating thrombi reported a mortality rate of 45%. 10
In conclusion, RA masses have a wide differential diagnosis in patients with DLBCL including mural thrombi, primary or secondary tumors, and/or thrombus associated with lymphoma. RA thrombus formation is rare in general but higher in patients with DLBCL. Intravascular large B-cell lymphoma is a very rare subtype disease that allows malignant lymphoid cells associated thrombosis. FA-DLBCL is another subtype that most commonly involves atrial myxomas or thrombi. We report a case of large RA mural thrombus incidentally diagnosed in a DLBCL patient. The mass warranted extensive workup and histologic examination to rule out intravascular large B-cell lymphoma and FA-DLBCL. We also highlight the rule of multimodality imaging for mass definition before surgical resection.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.