
Abstract
An 80-year-old male patient presented with sepsis secondary to infected central line which was placed for native aortic valve endocarditis. He also had melena and abdominal pain prior to his presentation. Abdominal computed tomography (CT) was done, which showed cholelithiasis. Esophagogastroduodenoscopy was also done with no source of bleeding identified. Later, he developed hemodynamic instability requiring aggressive fluid resuscitation and multiple packed blood cell transfusions. In view of his hemodynamic instability, a repeat abdominal CT scan showed air droplets within the gallbladder pneumobilia, ascites, diverticulosis, and a bleeding infrahepatic hematoma measuring 6 × 10 cm, which was not on his prior scan 2 days prior. A mesenteric arteriogram was performed that identified an aneurysm of the right hepatic artery with no active bleeding; therefore, it was coiled. Due to his continued clinical decompensation, he underwent an urgent open cholecystectomy, in which serosanguineous fluid, cholecystocolic fistula, and old clot related to his previous bleed were encountered. However, control of bleeding was difficult, and the patient expired. We report this case of right hepatic artery aneurysm that we believe its etiology was related to eroding cholecystitis.
Introduction
Most of hepatic artery aneurysms are extrahepatic (80%) with 60% of these located in the common hepatic artery, 30% located in the right hepatic artery, and 5% located in the left hepatic artery. 1 Pseudoaneurysms of the hepatic artery are very rare and usually occur following blunt or penetrating trauma, iatrogenic sequelae of hepatic and biliary procedures, and less commonly due to chronic infection or inflammation. 2 Patients with hepatic pseudoaneurysms can present with abdominal pain, jaundice, melena, and/or a pulsatile mass. Diagnosis usually starts with ultrasound imaging and computed tomography (CT) with the gold standard for the diagnosis being made with angiography. However, diagnosis can be difficult and missed in the setting of advanced liver disease and sepsis as reported in this case below.
Case Presentation
An 80-year-old Caucasian male with a history of hypertension, infective endocarditis, and cirrhosis secondary to alcoholic liver disease presented with abdominal pain and melena. On examination, he was noted to have tachycardia, skin erythema, and palpable tenderness at the site of a peripherally inserted central catheter line. He had a recent history of methicillin-resistant Staphylococcus aureus bacteremia treated with intravenous daptomycin due to native aortic valve endocarditis for which the central line was placed. He was found to have a normal complete blood count, normal liver enzymes, bilirubin levels, and an international normalized ratio level of 2. His warfarin was held, and his central line was removed. Abdominal CT was done, which showed cholelithiasis. He subsequently underwent an esophagogastroduodenoscopy, given his presentation of melena with no source of bleeding was identified. He, thereafter, developed hemodynamic instability with hemoglobin drop from 12.4 g/dL at admission to 9.7 g/dL requiring aggressive fluid resuscitation and multiple packed blood cell transfusions. A repeat abdominopelvic CT scan with contrast noted to have air droplets within the gallbladder pneumobilia, ascites, diverticulosis, and an infrahepatic hematoma measuring 6 × 10 cm (Figure 1). A mesenteric arteriogram was performed that identified an aneurysm of the right hepatic artery with no active bleeding (Figure 2). The aneurysm was coiled with 12-mm, 10-mm, 7-mm, and 3-mm detachable coils (Figure 3). He underwent an urgent open cholecystectomy due to clinical decompensation, which showed once dissected, serosanguineous fluid, cholecystocolic fistula, and old clot related to his previous bleed that was coiled. However, control of bleeding was difficult, and the patient expired.

Computed tomography scan of the abdomen showing air droplets within the gallbladder pneumobilia, ascites, diverticulosis, and an infrahepatic hematoma measuring ~6 × 10 cm.

A mesenteric arteriogram showing aneurysm of the right hepatic artery with no active bleeding.
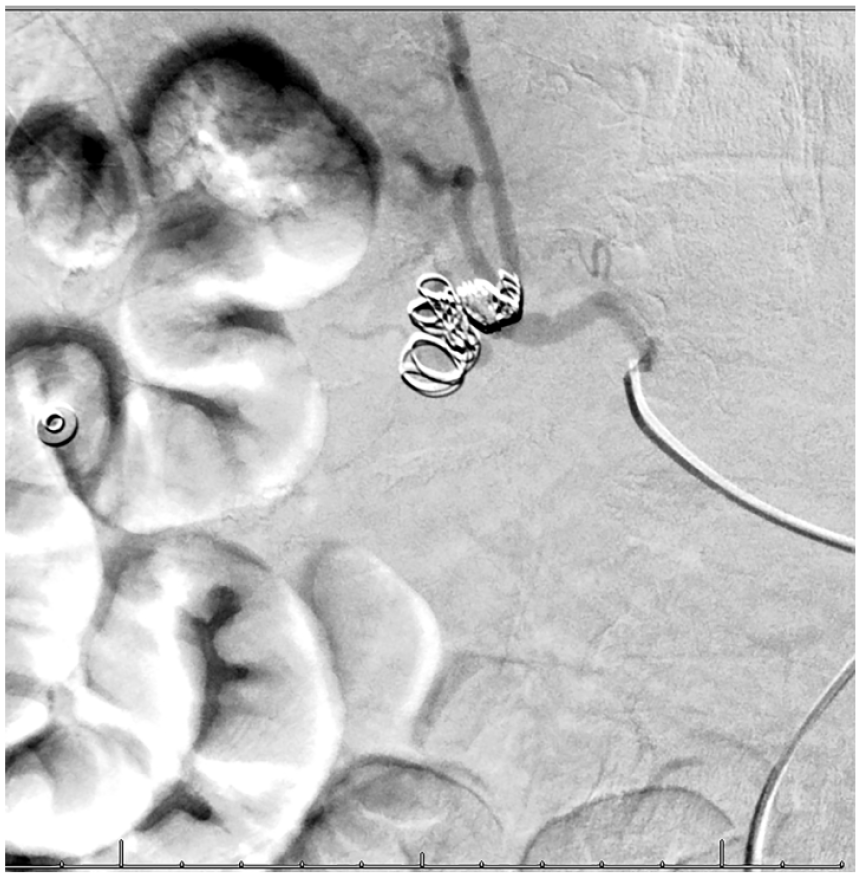
A mesenteric arteriogram showing the aneurysm of the right hepatic artery after it was coiled with 12-mm, 10-mm, 7-mm, and 3-mm detachable coils.
Discussion
Visceral artery aneurysms (VAAs) and pseudoaneurysms (VAPAs) are defined as aneurysms affecting the celiac, superior, or inferior mesenteric arteries and their branches. VAA and VAPA are relatively rare with a reported incidence of 0.1% to 0.2%, although the true incidence is not known since many are asymptomatic. 1
The splenic artery (VAA) and hepatic artery (VAPA) are most commonly involved, and the diagnosis is increasingly more frequent due to the detection of incidental disease using advanced imaging modalities often performed to evaluate unrelated complaints as seen in this case.
Atherosclerosis is considered the most common etiology (approximately 30% to 50%) followed by cystic medial necrosis (24%) and trauma (22%). 3 Penetrating or crush injuries, liver transplantation, or any surgical procedures such as percutaneous needle biopsy of the liver can result in posttraumatic false aneurysms. 4
Most hepatic artery aneurysms are incidentally identified on routine imaging to investigate unrelated symptoms and pathology. This is in contrast to the era prior to widespread abdominal imaging, in which most hepatic artery aneurysms presented with rupture or were discovered during autopsy. Symptomatic hepatic artery aneurysm presents with nausea and right upper quadrant or mid-epigastric pain radiating to the back. In many instances, hepatic artery aneurysm is discovered when the biliary tree and/or portal vein is eroded, which leads to development of portal hypertension, or rupture in the retroperitoneal space. Hemobilia, which is suggested by Quincke’s classic triad (jaundice, biliary colic, and gastrointestinal bleeding), occurs in one third of patients with hepatic artery aneurysm. 5 Rarely, large hepatic artery aneurysms may present as a pulsatile right upper quadrant mass and to lesser extent as infected (mycotic) aneurysms in less than 10% of cases, which was the dominant clinical presentation before the antibiotic era.
Conclusion
In the literature, there are very few cases reported with ruptured pseudoaneurysms to the peritoneum in the setting of cholecystitis as the diagnosis can be difficult and missed in patients with advanced liver disease, bleeding, and sepsis. Early recognition of hepatic artery aneurysms is required given risk for rupture, hemorrhage, and a higher mortality rate. Therefore, we report this case to emphasize the high level of awareness of the pseudoaneurysmal disease and inflammatory conditions.
Footnotes
Authors’ Note
This article was presented as a poster titled as “An Unusual Cause of an Intraperitoneal Bleed: Bleeding Hepatic Artery Pseudoaneurysm due to an Eroding Cholecystitis” at the American College of Physicians—Arkansas Chapter Scientific Virtual Meeting in Little Rock, Arkansas; September 2020.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal consent was obtained directly from the patient.