
Abstract
Subacute invasive aspergillosis is an infection that locally destroys lung parenchyma, and it affects patients with mild immunocompromise. The diagnosis is made by clinical symptoms, imaging, and laboratory results related to the infection. Early diagnosis and treatment is imperative for a favorable patient outcome. In this article, we present the case of a 19-year-old woman who was admitted to the intensive care unit for puerperal sepsis where a hysterectomy was performed. During her hospitalization, she presented atelectasis of the left lung and hemodynamic instability. Chest X-ray and chest computed tomography scan were performed and showed round opacities. It was decided to perform flexible bronchoscopy with bronchoalveolar lavage. An unusual subacute form of implementation of aspergillosis was confirmed by a bronchoalveolar lavage culture that showed the presence of Aspergillus. Images taken during bronchoscopy revealed Aspergillus implantation in the lung and serum galactomannan antigen test was positive. Voriconazole was introduced, 200 mg daily. The patient showed clinical improvement and was discharged from our hospital. We conclude that subacute invasive aspergillosis is a serious infection that can lead to high mortality. Bronchoscopy with bronchoalveolar lavage allows access and effective visualization of the airway as well as sampling for Aspergillus identification.
Introduction
Aspergillus is a saprophytic, filamentary, hyaline, ubiquitous fungi with universal distribution, and it can be found on soil, dust, plants, and water sources. 1 Aspergillus accounts for 180 species, and the most common human infection is Aspergillus fumigatus, which is transmitted by spore inhalation. 2
Pulmonary aspergillosis has a wide spectrum of presentation; it is classified by order of severity as invasive pulmonary aspergillosis, chronic pulmonary aspergillosis, and allergic bronchopulmonary aspergillosis. The clinical presentation varies depending on the interaction among Aspergillus’ pathogenicity, host immunological status, and its response toward the fungus. 3
Invasive pulmonary aspergillosis is the most severe form, and it affects lung blood vessels as well as the parenchyma causing thrombosis, ischemia hemorrhagic infraction, and necrosis. 4 Radiological features include single or multiple nodules; progressive consolidation; halo sign, nodule surrounded by a ground-glass appearance and it can progress to form a cavitation, which is denominated crescent sign; parabronchial infiltrates; and pleural effusion, and in massive Aspergillus exposure, a miliary pattern can be observed. 5
Subacute invasive aspergillosis (SAIA) is considered a mild form of invasive pulmonary aspergillosis with a slower progression, and it usually takes between weeks to months, producing a locally destructive disease in the lung parenchyma without invading other organs. 6 This pathology is seen in patients mildly immunocompromised mainly because of diabetes mellitus, malnutrition, alcoholism, chronic liver disease, advancing age, low-dose corticosteroid therapy or any immunosuppressive therapy, HIV (human immunodeficiency virus) infection, chronic obstructive pulmonary disease, connective tissue disorder, radiotherapy, and nontuberculous mycobacterium infection. 7
The diagnosis of SAIA is made on compatible symptomatology, imaging, and laboratory results. 8 Test results show elevated inflammatory markers, such as erythrocyte sedimentation rate, and either a positive serum Aspergillus precipitin test or positive Aspergillus species isolation from respiratory tract or pleural cavity. 9 The aim of an early diagnosis is to promptly treat the patient, which leads to a better prognosis.
We present an unusual case of a patient with puerperal sepsis who was diagnosed with SAIA by chest X-ray (CXR) and computed tomography (CT) imaging as well as by a positive isolation of the Aspergillus taken by a bronchoalveolar lavage (BAL).
Presentation of Clinical Case
A 19-year-old woman who worked as a laundress in a river presented to a primary health care facility 72 hours prior to admission, after giving birth by vaginal delivery. Her main complaints were transvaginal bleeding and persistent fever. In the primary health facility, the doctors performed a uterine aspiration, and 48 hours after the procedure, as the patient continued with the same symptomatology, she was referred to our hospital.
On examination, the patient presented fever, tachycardia, tachypnea, use of accessory breathing muscles, and oxygen saturation of 80%. Laboratory results showed slightly low hemoglobin of 11.1 g/dL and hematocrit 32.9% with elevated leukocyte count of 19 900 mm3 and a normal platelet count of 350 000 mm3, glucose 79 g/dL, serum sodium 138 mEq/L, potassium 2.5 mEq/L, chlorine 108 mEq/L, urea 5, and creatinine 0.9 g/dL. A pelvic abdominal CT scan evidenced a uterus with hyperdense areas outside the pelvic cavity.
The patient was diagnosed with puerperal sepsis and a partial hysterectomy was performed. After the procedure, the patient was transferred to the intensive care unit where she remained with invasive mechanical ventilation on intermittent positive pressure ventilation mode; sedation and analgesia with propofol 1 mg/kg/h and fentanyl 1 µg/kg/h, respectively, and vasopressors with norepinephrine 0.1 to 0.2 µg/kg/min, for 3 days. Intravenous antibiotics were administered and included meropenem 2 g every 8 hours and vancomycin 1 g every 12 hours. Additionally, the patient presented vaginal mycosis, so fluconazole was introduced.
Chest X-ray and CT evidenced a nodular pattern and infiltrates in both lungs, and by the third day of admission, we observed a total atelectasis of the left (Figure 1).

Chest X-ray and computed tomography scan was done showing a nodular pattern and infiltrates in both lungs (black arrow).
A bronchoscopy was performed and revealed small grayish lesions in the right upper lobe, and decreased bronchial size due to persistent bronchospasm in the right middle lobe. In the upper left lung, light greenish mucus was found with plugs that occluded the main bronchus, which caused an extensive bronchial collapse (Figure 2). During the procedure, cytologic samples were taken and BAL of the left lung was performed, toward the identification of Mycobacterium tuberculosis, gram-negative bacteria, and fungi. During bronchoscopy, the patient presented desaturation. A control CXR showed complete recovery of the left lung atelectasis. Following the procedure, the patient’s condition improved; she was hemodynamically stable while weaning vasopressors and sustained an optimal renal function.
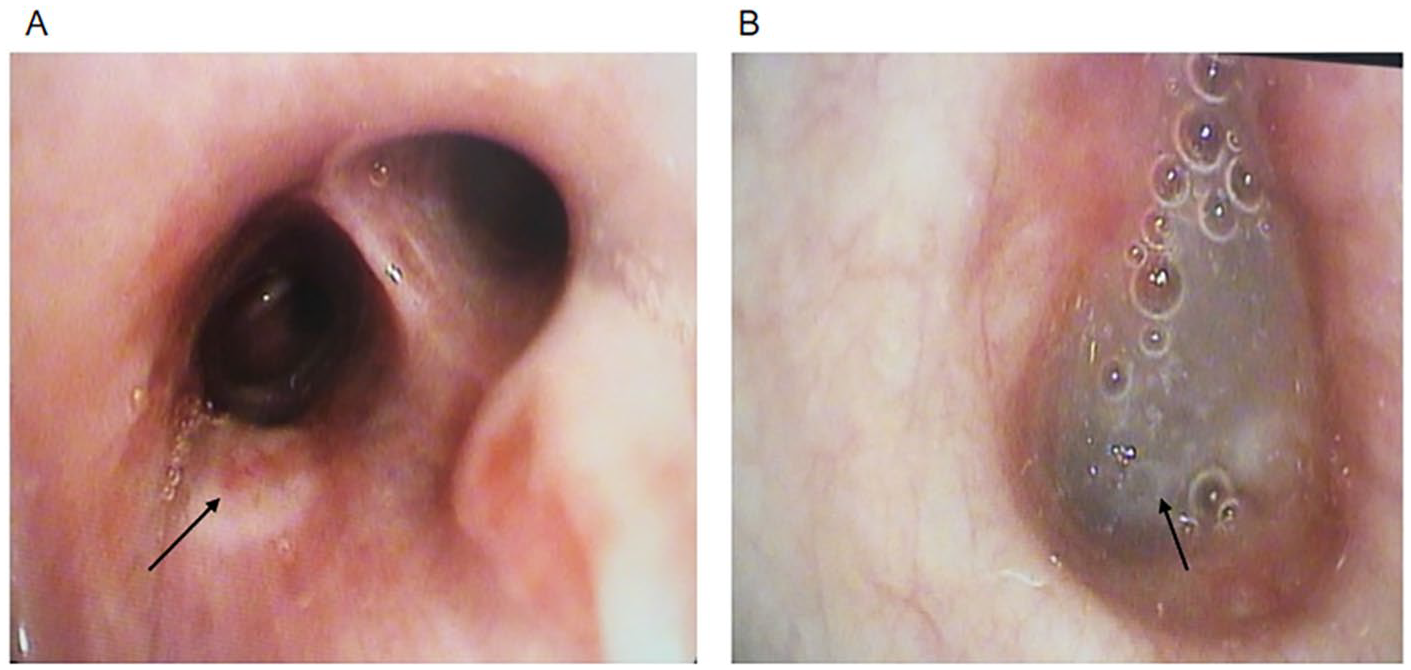
(A) Small grayish lesions in the right upper lobe (black arrow), but no lesions were found on the apex; decreased bronchial size due to persistent bronchospasm in the right middle lobe. (B) In the upper left lung, a light greenish mucus was found with plugs (black arrow) that occlude the main bronchus, which caused an extensive bronchial collapse.
On the sixth day of admission, a second bronchoscopy was performed and BAL with 50 cc of saline in the right upper lobe, where thickened fibrous tissue was found, and in the left upper lobe, which evidenced edematous areas with reddish-white plaques adherent to the bronchial walls. Serum galactomannan antigen test was positive.
One week after admission, the patient was recovering, hemodynamically stable without vasopressors, successfully extubated, and discharged from the intensive care unit 2 days later.
The BAL’s cultures evidenced filamentous fungi, identified as Aspergillus fumigatus (Figure 3), so 200 mg/day of voriconazole was introduced. The patient showed clinical improvement and was discharged from our hospital.

Presence of filamentous fungi, identified as Aspergillus fumigatus (black arrow).
The pathological study of the uterus showed that the membranous-spongeous material of the endometrial cavity appeared to be adhered to the myometrial thickness of the uterus and cervix, and additionally dilated and congestive vascular structures were evidenced. Furthermore, macroscopic samples confirmed some fungal structures, tabicated hyphae and micelles.
Discussion
Patients who develop SAIA often share a history of community exposure, such as gardening, working in construction, or contact with natural water sources. 10 Medical facilities are also associated with Aspergillus outbreaks specially related to mechanical ventilators. 11
Immune alterations are the main determinant to develop an Aspergillus infection. Neutrophils play a crucial role in preventing the infection development, by the NADPH’s oxidase (nicotinamide adenine dinucleotide phosphate oxidase) dependent and independent pathways. 6
Pregnancy is characterized by multiple immune regulation processes to sustain fetal viability and reports support a suppression in adaptive responses, as well as functional modifications, especially in phagocytic cells. Furthermore, a decrease in the response of microbial elimination by neutrophils during pregnancy leads to an increase risk of susceptibility to infections in this population. 12
In this case, we reported a subacute pulmonary aspergillosis infection after puerperal sepsis in a patient whose background involved constant contact with natural water sources as she worked in the river.
The CT scan performed showed rounded opacities consistent with Aspergillus infection, and BAL and samples taken by bronchoscopy confirmed the infection.
Bronchoscopy and BAL were key to solve this case. Bronchoscopy and BAL provided relevant information; we could evidence the presence of a cavernous lesion gone unnoticed due to persistent bronchial bronchospasm and a plug occluding the main bronchus. Both are characteristic of an Aspergillus infection. The bronchial lavage allowed us to culture and confirm the Aspergillus infection, and serum galactomannan antigen test was positive.
It is crucial to initiate an early treatment due to the rapid and devastating progression of the disease.
Conclusion
Subacute invasive aspergillosis is a serious infection with high mortality rates. Bronchoscopy and BAL allows to access and examine effectively and safely the respiratory airways. Early BAL and diagnosis were critical for the patient’s prognosis.
Footnotes
Authors’ Note
This research study was conducted at Intensive Care Unit, Ecuadorian Institute of Social Security (IESS), Babahoyo, Ecuador.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
The study protocol was approved by the Ethics Committee of Clinical Research of the Ecuadorian Institute of Social Security (IEESS), Babahoyo (IESS-HG-BA-DTMC-2019-1231/CODIGO 008).
Informed Consent
Informed consent was obtained from the patient and his surrogate.