
Abstract
A 76-year-old Caucasian male with a history of rheumatoid arthritis, Raynaud’s phenomenon, pulmonary embolism on warfarin, and a previous amputation of his left partial ring and fifth finger presented with acute onset of rash in bilateral lower extremities. He was recently started on trimethoprim-sulfamethoxazole due to concern for cellulitis. Differential diagnosis for acute-onset rash with the patient’s history presented as a challenge to the internist, as the differential is broad. Our case goes through the differential diagnosis to contrast the different presentations of rash in a patient with vasculitis. Ultimately skin biopsy in conjunction with a past positive cryoglobulinemic level helped confirm the diagnosis of cutaneous vasculitis, following which he was started on appropriate treatment and recovered.
Introduction
Cryoglobulinemia refers to the presence of cryoglobulin in a patient’s serum. It is a rare condition with the most common clinical manifestations in >90% of patients being skin lesions, specifically orthostatic purpura and ulcers. 1
Cryoglobulinemic vasculitis (CryoVas) is a small-vessel vasculitis associated with chronic infections, in particular hepatitis C virus, autoimmune disorders, and B-cell lymphoproliferative disorders.
Around 2% to 15% of cryoglobulin-positive patients are considered to develop CryoVas. For correct diagnoses, the first step is detection of serum cryoglobulins in blood, for that blood samples must be collected and kept at 37 °C on the way to the laboratory. 2 We present this case of serum negative CryoVas. It illustrates some of the common barriers to timely diagnosis that are encountered in patients with CryoVas in rural settings. Our patient did not have access to resources resulting in there being difficulty in making the correct diagnosis. But once the diagnosis was made, the appropriate treatment recommendations for the patient were relatively straightforward.
Case Presentation
A 76-year-old Caucasian male with a history of rheumatoid arthritis, Raynaud’s phenomenon, pulmonary embolism on warfarin, and a previous amputation of his left partial ring and fifth finger presented with acute onset of rash in bilateral lower extremities. He had a 1-week history of worsening bilateral lower extremity rash, which initially looked like “a bad sunburn.” The rash eventually turned into clear blisters progressing into painful open sores that were oozing serosanguinous fluid. Significant laboratory results included leukopenia with white blood cell count of 2.0 K/µL with absolute neutrophil count >1500/µL, international normalized ratio 3.9, C-reactive protein 5.7 mg/dL, erythrocyte sedimentation rate 95 mm/h, low C4 level at 4 mg/dL, normal C3 level at 95 mg/dL, rheumatoid factor of 557.1 IU/mL, positive ANA IgG (immunoglobulin G), negative serum cryoglobulin, negative ANCA, and negative hepatitis C antibody. Serum protein electrophoresis showed albumin level of 3.3 g/dL and β-2 globulins of 0.8 g/dL. Urine protein electrophoresis showed urine protein/creatinine mass ratio of 309 mg/g creatinine. He was recently started on trimethoprim-sulfamethoxazole due to concern for cellulitis. Our differential at this point included trimethoprim-sulfamethoxazole–associated rash, warfarin-induced skin necrosis, vasculitis, rheumatoid arthritis–induced vasculitis, systemic lupus erythromatosis, pyoderma gangrenosum, and infection including osteomyelitis as his previous fingers’ biopsy showed periostitis. Venous and arterial Doppler ultrasound were negative for arterial or venous thrombosis bilaterally. We reached out to his rheumatologist, and we learnt that in his previous assessments he had a positive serum cryoglobulin level, hence a provisional diagnosis of vasculitis was made, and high-dose steroids were started. A punch biopsy was performed and revealed acute small vessel vasculitis with fibrin thrombin (Figures 1 and 2) consistent with CryoVas as likely true diagnosis explaining his presentation. The patient’s rash improved significantly; he was discharged on oral steroids with follow-up at rheumatology for further management of vasculitis.
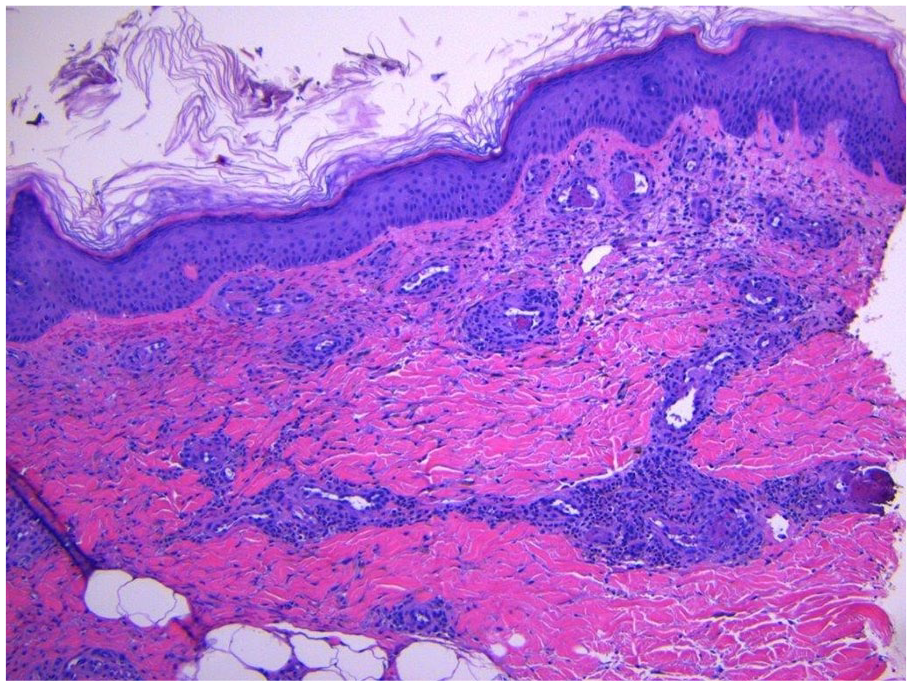
Punch biopsy of skin lesion showing acute vasculitis with thrombi formation.

Magnified image of punch biopsy of skin lesion showing vasculitic changes with lymphocytic infiltrate.
Discussion
Cryoglobulinemic vasculitis refers to a systemic inflammatory syndrome that generally involves small-to-medium vessel vasculitis due to cryoglobulin-containing immune complexes. Cutaneous manifestations develop in nearly all patients with cryoglobulin syndromes and tend to precede extra cutaneous manifestations by decades. Lesions may consist of erythematous macules and purpuric papules of the lower extremities (90% to 95%) as infractions, hemorrhagic crusts, and ulcers.
CryoVas creates a challenge to the physician as vasculitis can be complicated by heterogeneous presentations that can mimic several diseases. In our patient, the first diagnosis in our differential was rheumatoid arthritis–induced vasculitis as he had a positive rheumatoid factor, but the patient never had documented active synovitis on examination; therefore, he did not meet criteria for rheumatoid arthritis based on 2010 Rheumatoid Arthritis Classification Criteria. 3 Patients with CryoVas can have a positive rheumatoid factor (72% to 95%) circulating in their serum. 4
The second differential was systemic lupus erythematosus as he had a positive ANA and leukopenia 2.00 K/µL, but he had no other clinical symptoms to meet the Systemic Lupus International Collaborating Clinics (SLICC) Criteria. 5 Also his skin biopsy did not support the diagnosis. Up to 40% to 45% of the patients with CryoVas can have a positive ANA. 4
Another differential on the patient’s list was osteomyelitis given his chronic nonhealing ulcers (Figure 3), but given negative cultures, recurrent nature, lack any predisposing factor made it less likely.

Wound photo of the right leg showing chronic non healing ulcers.
Clinical presentation of CryoVas can also depend on the type of cryoglobulinemia. Type I is usually associated with symptoms of hyperviscosity; neurologic symptoms like dizziness, confusion, headache, and stroke or symptoms of vascular stasis; and livedo reticularis, acrocyanosis, and digital gangrene.
Types II and III are more commonly associated with myalgia, arthralgia, and purpura. Systemic manifestations include cutaneous ulcerations, peripheral neuropathy, and membranous glomerulonephritis.
Evaluation of patient with suspected vasculitis should include complete blood count, chemistries, ANA, ENA, ANCA, RF, C3, C4, cryoglobulins, hepatitis serology, SPEP, UPEP, chest X-ray, urine analysis, and skin biopsy.
First-line treatment for CryoVas involves immunosuppression with high-dose corticosteroids such as intravenous methylprednisolone followed by oral tapering for severe cases, mild-to-moderate presentations can be treated with oral prednisone.6,7 For steroid sparing and resistant vasculitis, cyclophosphamide, and/or plasmapheresis are thought to be effective treatment options. In our patient, once his cutaneous vasculitis was diagnosed, he was started on high-dose methylprednisolone with significant improvement in his symptoms. He was discharged to follow-up as an outpatient with a rheumatology for further treatment options.
Conclusion
This case highlights that vasculitis can mimic numerous other rheumatological conditions and even musculoskeletal infections. Since rural settings generally have paucity of rheumatology subspecialist, internal medicine physicians, hospitalists, and general practitioners should always keep in mind that the development of rash in a patient with history of or possible rheumatological disease should raise suspicion for underlying vasculitis and a biopsy can help in achieving the correct diagnosis. Training and recruitment of more rheumatologist to support the management of rheumatological conditions in rural settings would not only support the generalists but also the community at large as patients with untreated or poorly treated rheumatological conditions increases risk of coronary vascular disease morbidity and premature mortality. 8
Footnotes
Acknowledgements
Deborah Johnson, MD, Pathology, White River Health Systems, Batesville, AR, USA.
Authors’ Note
This article was originally presented as follows: Khalid Sawalha, Anthony Kunnumpurath, Shailendra Singh, Gilbert-Roy Kamoga. It’s just a rash they said! Acute skin manifestations in a patient with Vasculitis. SSCI-AFMR. New Orleans, LA, February 2020.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Informed consent for patient information to be published in this article was not obtained because the patient has passed away and further contact with his family was unsuccessful.